Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Protein (nutrient) wikipedia , lookup
List of types of proteins wikipedia , lookup
Model lipid bilayer wikipedia , lookup
Hedgehog signaling pathway wikipedia , lookup
Protein phosphorylation wikipedia , lookup
P-type ATPase wikipedia , lookup
G protein–coupled receptor wikipedia , lookup
Signal transduction wikipedia , lookup
Nuclear magnetic resonance spectroscopy of proteins wikipedia , lookup
From www.bloodjournal.org by guest on June 18, 2017. For personal use only.
● ● ● THROMBOSIS & HEMOSTASIS
Comment on Ağar et al, page 1336
A---------------------------------------------------------------------------------------------------------------snappy new concept for APS
Jacob H. Rand
ALBERT EINSTEIN COLLEGE OF MEDICINE
In this issue of Blood, Ağar and colleagues present data for a novel explanation of
how an antigenic target on 2GPI, a central protein in the APS disease process, can
become available for binding by antibodies.1
DV
+ +
DI
DI
+ +
DII
DIV
DII
DIII
Arg 39 & 34
Lys 19
Binding site
of antibodies
DIII
DIV
DV
-
-
-
-
+ +
-
Lys 305 & 317
-
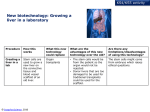
An adaptation of Ağar et al’s Figure 71 showing the transition between the 2 conformations of 2GPI.
Professional illustration by Paulette Dennis.
he antiphospholipid syndrome (APS), an
autoimmune thrombophilic disorder, was
recognized as a diagnostic entity by astute clinical
observations of the coincidence of thrombosis
and/or recurrent miscarriages with empirically
derived clinical tests.2 These include immunoassays that were derived from the biologic falsepositive syphilis test and blood tests that detect
inhibitors of phospholipid-dependent coagulation reactions, known as lupus anticoagulant
assays.
In retrospect, the “antiphospholipid” terminology is erroneous and reflects the initial
belief that phospholipids themselves are the
targets of the antibodies. This misconception— but not the name of the syndrome—
was corrected approximately 20 years ago,
when it was discovered that the actual target
antigens are phospholipid-binding proteins,
T
blood 2 6 A U G U S T 2 0 1 0 I V O L U M E 1 1 6 , N U M B E R 8
particularly 2-glycoprotein I (2GPI), a relatively abundant plasma protein whose biologic
function(s) has not been established.
X-ray crystallographic studies3,4 revealed
that the protein, with its 5 homologous domains, has a J-shaped structure that is analogous to a fishhook with a “barb” consisting of a
hydrophobic loop with surrounding positively
charged residues near the carboxyterminus on
domain V. This region allows the protein to
bind bilayers containing anionic phospholipids via affinity for negatively charged polar
heads and insertion of the loop within the hydrophobic middle of the bilayer (see figure).
While several investigators have reported
different specificities for the antibodies, there
is significant evidence that patients having
antibodies recognizing an epitope in domain I
are at an increased risk for thrombosis.5 It has
been proposed that the antibodies may dimerize or perhaps multimerize the protein and
that the multivalency of these antibody2GPI complexes for phospholipids would
increase their affinity/avidity for the bilayers
(and potentially other receptors), which in
turn would amplify the putative downstream
thrombogenic effects of the antibodies. The
latter might occur via disruption of endogenous anticoagulant mechanisms on vascular
endothelial cells or by triggering signaling
events that induce prothrombotic programs
(eg, expression of tissue factor or cell-adhesion
molecules).
Ağar et al address the specific question of
why these antibodies can only recognize domain I after the 2GPI has become bound to
phospholipid6 but not unbound 2GPI in
solution. The specifics of this process were not
previously understood, but were presumed
caused by conformational change(s). Ağar et al
provide convincing evidence for a simple and
elegant mechanism: unbound 2GPI present
in solution exists in a closed circular conformation—in effect, as a coiled fishhook—in
which domain V is noncovalently bound to
domain I and thereby shields the domain I
epitope from availability for antibody recognition. The binding of 2GPI to a phospholipid
bilayer via the “barb” on domain V unsnaps
this coiled protein into its open fishhook conformation, thereby exposing the epitope (see
figure). The authors present a convincing
body of evidence for this idea, including electron microscopic images, differential trypsin
digestion profiles, surface plasmon resonance
binding studies of the affinity of recombinant
domains for each other, and functional studies
that compare the anticoagulant effects of the
conformations.
These results add a significant detail in our
understanding of the APS disease process, which
can be outlined as follows: 2GPI is present in
plasma where it has been suggested to play a role
in the clearance of apoptotic cells and microparticles. The circular protein then undergoes a
conformational change when it comes into contact with membranes of cells that have entered
the apoptotic program and express anionic phospholipids; domain V unsnaps from domain I and
inserts into the bilayer and the fishhooks agglomerate into disc-like clusters,7,8 a process that is
probably required for the protein’s biologic role.
In patients who have a genetic susceptibility for
1193
From www.bloodjournal.org by guest on June 18, 2017. For personal use only.
developing APS, the exposure of the neoepitope
on domain I may trigger an autoimmune response and stimulate formation of aPL antibody2GPI immune complexes on the surface of the
cell membranes.8 In turn, these antiphospholipid
antibody-2GPI immune complexes may exert
a variety of effects on the cell membranes, including interference with membrane-mediated
antithrombotic mechanisms such as A5 crystallization, protein C activation, and annexin A2–
mediated fibrinolysis, as well as stimulation of a
prothrombotic and proadhesive phenotype, activation of complement, and perhaps effects on the
rigidity of the cell membranes.
There were a few limitations in this study.
Having the direct evidence of EM images of
2GPI bound to phospholipid would have
been helpful; however, the authors report that
this was not technically feasible because the
protein aggregated lipid vesicles. In addition,
the 2 conformations of purified 2GPI were
prepared by dialyzing the purified protein
against nonphysiologic buffers: alkaline pH
and a high salt concentration for the open conformation and an acidic buffer for the closed
conformation. Finally, IgG fractions from
only a small group of 3 patients were used to
show that the antibodies recognize the open,
but not the closed, conformation of 2GPI; it
would be interesting to know whether analysis
of a larger number of APS patients would confirm this to be a consistent finding or show
evidence for heterogeneity.
Nevertheless, this work is an important
contribution that advances the understanding
of an early step in the APS disease process and
may provide new insights for improved diagnosis and treatment of this disorder. Learning
whether this “coiled fishhook” model for conformational change is found to occur with
other binding proteins will also be interesting.
Conflict-of-interest disclosure: The author
declares no competing financial interests. ■
REFERENCES
1. Ağar C, van Os GM, Mörgelin M, et al. {beta}2-Glycoprotein I can exist in 2 conformations: implications for our
understanding of the antiphospholipid syndrome. Blood.
2010;116(8):1336-1343.
2. Hughes GR, Harris NN, Gharavi AE. The anticardiolipin syndrome. J Rheumatol. 1986;13(3):486-489.
3. Bouma B, de Groot PG, van den Elsen JM, et al. Adhesion mechanism of human beta(2)-glycoprotein I to phospholipids based on its crystal structure. EMBO J. 1999;18
(19):5166-5174.
4. Schwarzenbacher R, Zeth K, Diederichs K, et al. Crystal structure of human beta2-glycoprotein I: implications
for phospholipid binding and the antiphospholipid syndrome. EMBO J. 1999;18(22):6228-6239.
5. de Laat B, Derksen RH, Urbanus RT, de Groot PG.
IgG antibodies that recognize epitope Gly40-Arg43 in domain I of beta 2-glycoprotein I cause LAC, and their presence correlates strongly with thrombosis. Blood. 2005;105
(4):1540-1545.
6. de Laat B, Pengo V, Pabinger I, et al. The association between circulating antibodies against domain I of
beta2-glycoprotein I and thrombosis: an international
multicenter study. J Thromb Haemost. 2009;7(11):
1767-1773.
7. Gamsjaeger R, Johs A, Gries A, et al. Membrane binding of beta2-glycoprotein I can be described by a two-state
reaction model: an atomic force microscopy and surface
plasmon resonance study. Biochem J. 2005;389(Pt 3):665673.
8. Rand JH, Wu XX, Quinn AS, et al. Hydroxychloroquine directly reduces the binding of antiphospholipid
antibody-beta2-glycoprotein I complexes to phospholipid
bilayers. Blood. 2008;112(5):1687-1695.
● ● ● VASCULAR BIOLOGY
Comment on Zhang et al, page 1377
PLDing
a case for angiogenesis
---------------------------------------------------------------------------------------------------------------Anne Hamik and Mukesh K. Jain
CASE WESTERN RESERVE UNIVERSITY
In this issue of Blood, Zhang et al identify the Src-PLD1-PKC␥ axis as critically
involved in the process that causes ROP, highlighting new potential targets for
therapy.1
ascular endothelial growth factor
(VEGF) is acknowledged as the predominant regulator of angiogenesis; blockade of VEGF signaling is central in therapy
for numerous cancers and the vascular retinopathies of diabetes, age-related macular
degeneration, and retinopathy of prematu-
V
1194
rity (ROP). Although anti-VEGF monotherapy shows substantial results, in many
cases it is becoming increasingly appreciated
that combination therapy will be necessary.2
Tumors have demonstrated various degrees
of intrinsic refractoriness or the development of treatment-related resistance. For
age-related macular degeneration, expected
to soon affect nearly 3 million people in the
United States, the optimal therapy of longterm monthly intraocular injections of antiVEGF agents will likely prove unsustainable
for practical and clinical reasons. Thus, effective treatment will require the combination of anti-VEGF therapy with conventional chemotherapeutic agents, radiotherapy or phototherapy, or the targeting of
multiple components of VEGF-activated
processes.
The breadth of disease states in which
VEGF-induced angiogenesis plays a central
role correlates to a large and incompletely
defined population of regulatory molecules
of VEGF signaling, many likely to be tumor/
context-specific. The Zhang paper defines the
players in a model of ROP and thus identifies
potential new specific targets for therapy. In
their report, Zhang and colleagues demonstrate that an intact VEGF-signaling axis—
constituted by the sequential activation of Src,
phospholipase 1 (PLD1), and protein kinase
C␥ (PKC␥)—mediates the pathologic neovascularization seen in the oxygen-induced
retinopathy model of ROP. This axis was
delineated in vitro using chemical inhibitors
(1-butanol and propranolol) and in vivo
using intraocular administration of siRNAs
specific to individual components of the
pathway.
Previous work has identified the protein
tyrosine kinase activity of Src as a regulator
of both VEGF expression and of responses
to VEGF stimulation.3 Zhang et al are the
first to report activation of PLD1 by Src.
Furthermore, they demonstrate that Srcdependent PLD1 activation is required for
subsequent activation of PLC␥. The recent
development of selective small molecule
inhibitors that target Src and the demonstration that Src inhibition can attenuate
chemoresistance of some solid tumors suggests a possible clinical use of Src inhibition
in vascular retinopathy.
Investigation of the role of bioactive lipids in regulation of angiogenesis is a burgeoning area of research likely to result in a
new class of therapeutic agents.4-6 Of particular topical interest are the bioactive lipids PLD1, phosphatidic acid (PA), lysophosphatidic acid (LPA), and sphingosine1-phosphate (S1P). After activation by any
of a variety of intracellular factors (including
26 AUGUST 2010 I VOLUME 116, NUMBER 8
blood
From www.bloodjournal.org by guest on June 18, 2017. For personal use only.
2010 116: 1193-1194
doi:10.1182/blood-2010-06-288209
A snappy new concept for APS
Jacob H. Rand
Updated information and services can be found at:
http://www.bloodjournal.org/content/116/8/1193.full.html
Articles on similar topics can be found in the following Blood collections
Information about reproducing this article in parts or in its entirety may be found online at:
http://www.bloodjournal.org/site/misc/rights.xhtml#repub_requests
Information about ordering reprints may be found online at:
http://www.bloodjournal.org/site/misc/rights.xhtml#reprints
Information about subscriptions and ASH membership may be found online at:
http://www.bloodjournal.org/site/subscriptions/index.xhtml
Blood (print ISSN 0006-4971, online ISSN 1528-0020), is published weekly by the American Society
of Hematology, 2021 L St, NW, Suite 900, Washington DC 20036.
Copyright 2011 by The American Society of Hematology; all rights reserved.