Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Epigenetics of human development wikipedia , lookup
Artificial gene synthesis wikipedia , lookup
Gene expression profiling wikipedia , lookup
Epigenetics of neurodegenerative diseases wikipedia , lookup
Cancer epigenetics wikipedia , lookup
Skewed X-inactivation wikipedia , lookup
Neuronal ceroid lipofuscinosis wikipedia , lookup
Y chromosome wikipedia , lookup
Nutriepigenomics wikipedia , lookup
Designer baby wikipedia , lookup
Microevolution wikipedia , lookup
Polycomb Group Proteins and Cancer wikipedia , lookup
Public health genomics wikipedia , lookup
Comparative genomic hybridization wikipedia , lookup
Neocentromere wikipedia , lookup
X-inactivation wikipedia , lookup
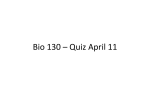
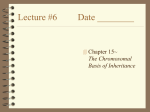
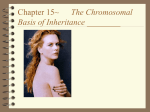
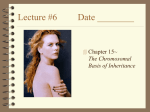
University of Groningen Soft tissue sarcoma at the turn of the millennium Nijhuis, Paulus Henricus Antonius IMPORTANT NOTE: You are advised to consult the publisher's version (publisher's PDF) if you wish to cite from it. Please check the document version below. Document Version Publisher's PDF, also known as Version of record Publication date: 2001 Link to publication in University of Groningen/UMCG research database Citation for published version (APA): Nijhuis, P. H. A. (2001). Soft tissue sarcoma at the turn of the millennium: aspects of epidemiology, cytogenetics, diagnosis and treatment s.n. Copyright Other than for strictly personal use, it is not permitted to download or to forward/distribute the text or part of it without the consent of the author(s) and/or copyright holder(s), unless the work is under an open content license (like Creative Commons). Take-down policy If you believe that this document breaches copyright please contact us providing details, and we will remove access to the work immediately and investigate your claim. Downloaded from the University of Groningen/UMCG research database (Pure): http://www.rug.nl/research/portal. For technical reasons the number of authors shown on this cover page is limited to 10 maximum. Download date: 18-06-2017 Chapter 6 67 Chapter 6 Prognostic relevance of cytogenetic changes in soft tissue sarcomas Nijhuis P.H.A.1, Hoekstra H. J.1, Plaat B.E.C.2, van der Graaf W.T.A.3, Sluiter W.J.4, Molenaar W.M.2, van den Berg E.5 1.Department of Surgical Oncology, Groningen University Hospital, Groningen, The Netherlands 2. Department of Pathology, Groningen University Hospital, Groningen, The Netherlands 3. Department of Medical Oncology, Groningen University Hospital, Groningen, The Netherlands 4. Department of Internal Medicin, Groningen University Hospital, Groningen, The Netherlands 5. Department of Medical Genetics, University of Groningen, Groningen, The Netherlands submitted 68 Prognostic relevance of cytogenetic changes in soft tissue sarcomas Chapter 6 Introduction The prognosis of soft tissue sarcomas (STS) largely depends on tumor-specific characteristics, as histological (sub) type, tumor grade, size and site [1-3]. In recent years, significant progress has been made in identifying chromosomal abnormalities in solid tumors. Characteristic cytogenetic alterations have been demonstrated in several STS, and often have diagnostic relevance [4-7]. Well-known rearrangements include the translocation t(11; 22)(q24; q11.2-12) in Ewings sarcoma and primitive neuroectodermal tumors, t(12;16) (q13; p11) in myxoid liposarcomas (MXLPS), t(X;18)(p11.2; q11.2) in synovial sarcomas, and t(2;13)(q35- 37;q14) in alveolar rhabdomyosarcomas [7-9]. Most studies deal with the specific chromosomal rearrangements within histological tumor types and refer to their diagnostic relevance, whereas only a few report on prognosis of such aberrations [10-14]. The present study analyzes the prognostic significance of cytogenetic changes observed in soft-tissue sarcomas, using a computer-assisted cytogenetic analysis [13]. A database was constructed, which permits the detection of statistically significant, non-random chromosomal aberrations and allows direct comparison of different karyotypes. Special attention was paid to cytogenetic differences between metastatic and non-metastatic STS and between patients who died of the disease and who did not. Materials and methods For this study, material for cytogenetic analysis was obtained from consecutive STS specimens submitted for pathologic examination at the Department of Pathology of the Groningen University Hospital from 1984- 1993. All STS were reviewed by a pathologist with special interest and experience in STS (WMM), and histopathologically classified according to the criteria described by Enzinger and Weiss [6]. Cytogenetic analysis was performed at the department of Medical Genetics at the University of Groningen. The criteria for inclusion in the current study were 1) a (reviewed) histological diagnosis of a primary or locally recurrent malignant mesenchymal tumor, located in the soft tissues, which had not been previously treated with radiotherapy and/or chemotherapy, 2) a successful karyotype, and 3) the availability of complete clinical follow-up. Mesenchymal proliferations of parenchymal organs were excluded. For genetic analysis, part of the tissue specimen was minced with scalpels, incubated in a collagenase-DNAse solution and cultured in RPMI 1640 supplemented with 16% FCS, glutamine and antibiotics. After short-term culture, cells were harvested, chromosomes were G-banded using trypsin/pancreatin, and karyotypes were described according to the ISCN 1995 Guidelines for Cancer [15]. If more than one tumor per patient was described, it was decided to use the karyotype of one tumor, preferably the primary tumor, to avoid overrepresentation. The database consisted of four main parts related to the described karyotype: 1) patients characteristics, 2) histopathological data, 3) gain and loss of chromosomal material, and 4) structural rearrangements. After interpretation of the karyotype, the gains and losses of chromosomal material were entered, as described by Plaat et al [13]. Each chromosome was divided according to the ideogram at 400 bands level as described by the ISCN, in such a Chapter 6 Prognostic relevance of cytogenetic changes in soft tissue sarcomas 69 way that the net gains and losses in 1p11-13 were summarized in 1p1, changes in 1p21-22 were summarized in 1p2, etc. In case of loss in a particular region a 1 was entered. If the same region was lost in both chromosomes, a 2 was entered. Similarly, if gain occurred in one of the chromosomal regions a +1 was entered, etc. Only changes as compared to the constitutional karyotype were evaluated. Data were analyzed for the number of tumors with gains or losses in a particular chromosomal region, and the mean change in chromosomal material per chromosomal region. Mean change in chromosomal material in each of the 86 chromosomal regions was expressed as a chromosomal change ratio (CCR), which was defined as the change in a specific chromosomal region as compared to a normal diploid karyotype. Only full abnormal karyotypes were used for the analysis of the over- or under representation of chromosomes or chromosomal regions. In the analysis of over- or under representation, markerchromosomes were not included, because of the fact that these are structurally rearranged chromosomes, in which no part can be identified. Chromosomal changes were compared between patients with metastasizing STS and those with STS that had not metastasized, and between patients with no evidence of disease and patients who had died from their disease. Graphs were constructed to visualize the change in chromosomal material, and the differences between selected groups. To identify chromosomal regions with significant gains or losses, 95% confidence intervals (CI) were determined. Survival curves were calculated by the method of Kaplan and Meier. Coxs proportional hazards regression model was used to assess the importance of specific chromosomal alterations in overall and metastasis-free survival. A P-value <0.05 was considered statistically significant. Results Patients Forty-three patients met the inclusion criteria, 23 males and 20 females (53% and 47%, respectively), with a mean age of 45 (range 2-81) years. Most STS (n=38) were primary tumors (88%), the others (n=5) were local recurrences (12%). Liposarcoma (LPS) was the most common histological type (n=20, 47%), followed by synovial sarcoma (n=5, 12%), malignant fibrous histiocytoma (MFH) (n=4, 9%), and rhabdomyosarcoma (n=2, 5%) [Table 1]. Table 2 presents the patients status of disease after a median and mean follow-up of 55 and Table 1. Distribution according to histopathology (n=43). Histopathology Liposarcoma Synovial sarcoma Sarcoma nos Malignant fibrous histiocytoma Rhabdomyosarcoma Others Sarcoma nos: sarcoma with no other specification n 20 5 5 4 2 7 70 Prognostic relevance of cytogenetic changes in soft tissue sarcomas Chapter 6 Table 2. Clinical status at follow-up. Primary STS Local recurrence Total AWD DOC DOD NED Total (34-195; 95; 116)1 (85) 1 (2-238; 34; 50) 1 (22-145; 71; 79) 1 (2-238; 55; 73) 1 3 3 6 1 1 15 1 16 19 1 20 38 5 43 AWD: Alive with disease; DOC: Dead of other cause:DOD: Dead of disease; NED: No evidence of disease. 1 Follow-up in months (range; median; mean). 73 months, respectively (range 2-238 months). Twenty patients (47%) showed no evidence of disease, after a median and mean follow-up of 71 and 79 months, respectively (range 22145 months). Sixteen patients had died from their disease (37%), after a median and mean follow-up of 34 and 50 months, respectively (range 2-238 months). Fourteen of these sixteen patients died from distant metastatic disease; the other two from irresectable local recurrences. One patient had died from a cerebral hemorrhage. Six patients (14%) were alive with recurrent disease, two of which had pulmonary metastases, whereas the other four (all retroperitoneal liposarcomas) had local recurrences. The mean and median metastasis free period in the metastasis group was 15 and 28 months, respectively, with a range of 0-128 months. The lung was the most common site of distant failure (n=13, 81%), followed by bone (n=3, 19%), liver (n=2, 13%), and soft tissues (n=1, 6%). Chromosomal loss and gain Construction of 95% confidence intervals (CI) revealed no statistically significant loss or gain of chromosomal material, expressed as chromosomal change ratio (CCR). Although not statistically significant, notable loss was seen in the chromosomal regions 15p, 21p, and 22q. Notable gain in chromosomal material was observed in region 7p1, 7p2, and 7q1 [Fig. 1]. The difference in CCR between patients still alive without evidence of disease, and patients who died from (recurrent) disease, is presented in Fig. 2. At univariate analysis, overall survival was influenced negatively by gain of chromosomal material in region 1q1-4, and by loss of chromosomal material in region 18q1-2, 14p, 18p, 10q1, Yp, Yq1, 2q23, 12p, 9p2, 17p, 17q1-2, and 4p (Table 3). At stepwise backward multivariate analysis, chromosomal gain in 1q (RR 38.7, P<0.001), and loss in 4p (RR 6.3, P=0.002) were the only negative prognostic factors regarding overall survival. Survival curves according to chromosomal change in the significant regions are presented in Fig. 3 a- c. The difference in CCR between patients who developed metastases during follow-up (n=16) and patients without distant metastases (n=27) is presented in Fig. 4. At univariate analysis, significant poor prognostic factors regarding distant relapse were gain of chromosomal material in region 1q1-2, and loss in regions 18p, 18q1-2, 10q1, 2q2-3, Yp, Yq, 10q2, 14p, and 22p (Table 4). At stepwise backward multivariate analysis, chromosomal loss in 18p (RR 8.3, P<0.001) remained the only significant negative prognostic factor regarding metastasis-free survival (Fig. 5). Furthermore, there was a strong association between loss in 18p and gain in 1q in patients with the shortest survival. Chapter 6 Prognostic relevance of cytogenetic changes in soft tissue sarcomas 71 Figure 1. Mean CCR with 95% Confidence Interval of all cases Figure 2. Mean CCR in patients with no evidence of disease (NED) versus patients who died of the disease (DOD) 72 Prognostic relevance of cytogenetic changes in soft tissue sarcomas Chapter 6 Table 3. Overall Survival: statistically significant chromosomal changes at univariate analysis. Chromosomal Change Gain of 1q1 Loss of 14p Loss of 18p Gain of 1q3 Gain of 1q2 Loss of 10q1 Gain of 1q4 Loss of Yp Loss of Yq Loss of 2q2 Relative Risk (RR) 7.7 6.3 6.3 6.3 5 5.6 4.4 5.6 5.6 5 P-value <0.001 <0.001 <0.001 0.001 0.006 0.009 0.01 0.01 0.012 0.013 Chromosomal Change Loss of 2q3 Loss of 12p Loss of 18q2 Loss of 9p2 Loss of 17p Loss of 17q1 Loss of 18q1 Loss of 4p Loss of 17q2 Figure 3a. Overall survival and gain in chromosome 1q Figure 3b. Overall survival and loss in chromosome 4p Relative Risk (RR) P-value 5 3 4.8 2.2 2.2 2.2 7.7 3 2.1 0.013 0.016 0.029 0.037 0.037 0.037 0.044 0.045 0.045 Chapter 6 Prognostic relevance of cytogenetic changes in soft tissue sarcomas 73 Figure 3c. Overall survival and loss in chromosome 18p Figure 4. Mean CCR in patients with metastasizing STS versus STS that did not metastasize Table 4. Metastasis-Free Survival survival: statistically significant chromosomal changes at univariate analysis. Chromosomal Change Gain of 1q1 Loss of 18p Loss of 10q1 Loss of 10q2 Loss of 2q2 Loss of 2q3 Loss of Yp Relative Risk (RR) 9.7 8.3 5.9 4.2 4.5 4.5 4.5 P-value <0.001 <0.001 0.005 0.014 0.015 0.015 0.02 Chromosomal Change Loss of Yq Loss of 14p Loss of 22p Loss of 18q2 Gain of 1q2 Loss of 18q1 Relative Risk (RR) P-value 4.5 3.3 2.2 4.2 5.9 6.3 0.02 0.025 0.031 0.037 0.048 0.049 74 Prognostic relevance of cytogenetic changes in soft tissue sarcomas Chapter 6 Figure 5a. Metastasis-free survival and loss in chromosome 18p Figure 5b. Metastasis-free survival and gain in chromosome 1q Discussion Cytogenetic analysis has demonstrated that both benign and malignant tumors often have characteristic chromosomal aberrations and that the karyotype may be important in diagnosis and treatment [5,7,16,17]. STS often reveal a very complex karyotype due to a large number of chromosomal abnormalities [13]. As all these chromosomal changes, either alone or in combination, might be responsible for certain steps in oncogenesis, it is very difficult to relate these changes to the oncogenetic process. Another problem is the difficulty to interpret and compare different studies, as most of them have presented karyotypes in such a way that comparison and statistical analysis is hardly possible. To overcome this problem, we started a database in which all karyotypes are interpreted and entered in a uniform fashion, which makes a computer-assisted analysis of large groups of karyotypes possible, as described by Plaat et al. [13]. Data from the database were linked to clinical outcome to determine the prognostic importance of shared cytogenetic abnormalities. In the present series, overrepresentation of STS with balanced translocations (especially the myxoid and round-cell liposarcoma subtype, characterized by the t(12;16) (q13;p11) Chapter 6 Prognostic relevance of cytogenetic changes in soft tissue sarcomas 75 translocation) seems to be of minor importance, as such translocations do not result in net gain or loss of chromosomal material. Correlation between cytogenetic alterations and prognosis has been documented in other human malignancies [18-22]. For STS, however, hardly any data exist on the prognostic relevance of specific chromosomal aberrations [23-25]. In the present study, univariate analysis of involved chromosomal changes revealed many regions with chromosomal alterations as negative prognostic factors. Several studies have identified cytogenetic bands in these regions involved in human tumor development and progression. Specific information on STS, on the other hand, is very scanty. In the present study, chromosomal gain in 1q1 was the most important negative prognostic factor regarding survival. A relation between alterations at the long arm of chromosome 1 and human malignancies has been demonstrated in various tumor types, suggesting the existence of oncogenes (breast cancer [26], prostate cancer [27], and endometrium cancer [28]), as well as tumor suppressor genes (breast cancer [26]) and medulloblastoma [29]). In liposarcomas, there are indications that amplification of genes located at 1q21-24, often with concomitant gain in 12q14-21, plays a significant role in development and progression [30]. Furthermore, the long arm of chromosome 1 is a region of particular interest with regard to metastasis, as it harbors the KiSS-1 metastasis-suppressor gene at 1q32, which has been identified as a metastasis-suppressor gene in malignant melanoma and breast cancer [31]. However, as gain of chromosomal material at the long arm of chromosome 1 was a negative prognosticator for metastasis-free survival, it seems very unlikely that this metastasis-suppressor gene is involved in the metastatic process of STS. The other negative prognostic factor regarding survival, loss in 4p, was surprising, as there is only very limited information on its role in human malignancies [32,33]. In their search for the human homologue of the SH3BP2 protein in bladder cancer, Bell et al. identified an interesting gene at 4p16.3 that is a potential negative regulator of the Abl gene [34], a proto-oncogene that has been related to differentiation and apoptosis inhibition in chondrosarcoma [35]. The association between high malignancy grade, a wellknown negative prognostic factor regarding disease-specific survival, and low amounts of apoptosis in STS [36], might further support a potential role of SH3BP2 and Abl genes in STS prognosis. At univariate analysis, aberrations in many other chromosomal regions were related to survival. Because of the magnitude of genes, located at these regions, and the fact that we did not investigate specific gene products, it is impossible to predict which chromosomal bands and which genes will be involved, although some regions (9p, chromosome 17, and 18p) are very intriguing. The negative prognostic importance of loss in region 9p2 was not unexpected, as this region contains the p16 (CDKN2A/ IKN4A) and p15 (CDKN2B/ IKN4B) genes, which act as negative regulators of proliferation of normal cells. Deletions or mutations of these CDK (cyclin-dependent kinase)- 4 and 6 inhibitors lead to unchecked cell growth, which has been demonstrated in many human cancer types [18,21,37]. In Ewings sarcoma, Wei et al. demonstrated that p16 deletion was a very strong negative prognostic factor (P<0.001) [37]. In Wilms tumors, loss of p16 also seems 76 Prognostic relevance of cytogenetic changes in soft tissue sarcomas Chapter 6 to be of prognostic importance, as it correlates with advanced tumor stage [39]. In STS, however, the prognostic impact of both p16 and p15 alterations remains contradictory. Orlow et al. reported a significant relation between p16 deletions or alterations and poor survival in 46 STS (P=0.036 and 0.005, respectively), with alteration of the IKN4A/B gene being the only statistically significant predictor for poor survival when controlling for tumor grade and size (P=0.03) [40]. Yao and Meye investigated the role of the p16 gene status and expression in STS, and reported a low frequency of deletions and mutations of this gene in STS, in contrast to Simons et al., who demonstrated a loss of 9p21 in 55% of MFH [42-44]. Moreover, Yao et al. suggested that CDK4 might act as an oncogene in STS, which is in contrast to findings in other human malignancies where CDK4 acts as a tumor suppressor gene [41]. In the present study, however, loss of region 9p2 is a statistically significant negative prognostic factor (P=0.037), suggesting the location of a STS suppressor gene in this region. The prognostic importance of chromosomal loss at the short arm of chromosome 17 is very interesting, as some important tumor suppressor genes are located there. TP53, located at 17p13.1, is the most common tumor suppressor gene, altered in many malignancies. A study from the Memorial Sloan Kettering Cancer Center demonstrated that 17p deletions and p53 mutations were common events in adult STS [44]. Dei Tos et al. demonstrated a 30% incidence of p53 aberrations in myxoid and round cell liposarcoma [45]. However, these studies did not provide any information on the prognostic importance of the p53 alteration. In a series of 113 bone and soft tissue sarcomas, Mousses reported p53 alterations at different frequencies in various sarcomas; furthermore, these alterations were not associated with prognosis [46]. As p53 expression was not examined in the present study, we can not be sure whether this gene product is responsible for the poor prognosis in patients with loss of the short arm of chromosome 17, or whether other suppressor genes at 17p are involved, as has been reported in sporadic breast cancer [47]. Besides chromosomal loss at the short arm of chromosome 17, also loss at its long arm had prognostic importance. One of the genes that might contribute to this is the protooncogene c-erbB-2, at band 17q21.1. Although a correlation between loss of 17q and a high degree of amplification of c-erbB-2 has been demonstrated in human breast cancer [48], no reports on its prognostic importance in STS are available. Loss of the short arm of chromosome 18 (18p1) was another important negative prognostic factor, both in metastasis-free and overall survival, suggesting the location of (a) putative suppressor gene(s). In the literature, there is some evidence for the presence of tumor suppressor genes on the short arm of chromosome 18, involved in breast carcinoma, NSCLC, and brain tumors [49]. Apart from that, information on the role of 18p in human malignancy is extremely scarce. Except for retroperitoneal STS, survival in STS has been related directly to metastasis. In human malignancies in general, and in STS in particular, the cytogenetic base for metastasis remains obscure. As reports revealing possible clues are awaited, the finding that loss of 18p was the only statistically significant negative prognostic factor regarding metastasis-free survival is very interesting, as it suggests the location of a putative (sarcoma-) metastasis suppressor gene. Chapter 6 Prognostic relevance of cytogenetic changes in soft tissue sarcomas 77 The computer-assisted approach, used in the present study, is valuable in the analysis of large groups of complex karyotypes to detect common chromosomal alterations. The strong association between gain in the long arm of chromosome 1 and loss in the short arm of chromosome 18 in patients with the shortest survival has not been reported before, and its importance in STS prognosis remains unclear. In conclusion, the present study provides indications for correlations between cytogenetic changes and metastasis and prognosis in STS. Some of these findings confirm earlier reports, whereas many are novel in STS, and need to be confirmed in additional studies. The strong association between alterations in the long arm of chromosome 1 and the short arm of chromosome 18 in non-survivors is very challenging and may have prognostic value in STS. References 1. Pisters PW, Leung DH, Woodruff J, Shi W, Brennan MF. Analysis of prognostic factors in 1.041 patients with localized soft tissue sarcomas of the extremities. J Clin Oncol 1996; 14: 1679-1689. 2. Pisters PWT and Pollock RE. Staging and prognostic factors in soft tissue sarcoma. Sem Radiat Oncol 1999; 9: 307-314. 3. Coindre JM, Terrier P, Bui N, et al. Prognostic factors in adult patients with locally controlled soft tissue sarcoma: A study of 546 patients from the French Federation of Cancer Centers Sarcoma Group. J Clin Oncol 1996; 14: 869-877. 4. Molenaar WM, Jong de B, Buist J, Idenburg VJS, Seruca R, Vos AM, Hoekstra HJ. Chromosomal analysis and the classification of soft tissue sarcomas. Lab. Invest 1989; 60: 266-274. 5. Fletcher JA, Kozakewich HP, Hoffer FA, Lage JM, Weidner N, Tepper R, Pinkus GS, Morton CC, Corson JM. Diagnostic relevance of clonal cytogenetic aberrations in malignant soft tissue tumors. N Engl J Med 1991; 324: 436-442. 6. Enzinger FM, and Weiss SW. (eds.) Soft Tissue Tumors, 3rd ed. St. Louis, C.V. Mosby, 1995. 7. Dei Toss AP, Dal Cin P. The role of cytogenetics in the classification of soft tissue tumors. Virchows Arch 1997; 431: 83-94. 8. Sreekantaiah Ch, Ladanyi M, Rodriguez E, Chaganti RSK. Chromosomal abberations in soft tissue tumors. Relevance to diagnosis, classification, and molecular mechanisms. Am J Pathol 1994; 144: 1121-1134. 9. Rydholm A. Chromosomal abberations in musculoskeletal tumours: clinical importance. J Bone Joint Surg 1996; 78-B: 501-506. 10. Fletcher CDM, Akerman M, Dal Cin P, et al. Correlation between clinicopathologic features and karyotype in lipomatous tumors. Am J Pathol 1996; 148: 623-630. 11. Szymanska J, Virolainen M, Tarkkanen M, et al. Overrepresentation of 1q21-23 and 12q13-21 in lipoma-like liposarcomas but not in benign lipomas: a comparative genomic hybridization study. Cancer Genet Cytogenet 1997; 99: 14-18. 12. Mertens F, Fletcher CDM, Dal Cin P, et al. Cytogenetic analysis of 46 pleomorphic soft tissue sarcomas and correlations with morphologic and clinical features: a report of the CHAMP study group. Genes, chromosomes Cancer 1998; 22: 16-25. 13. Plaat BEC, Molenaar WM, Mastik MF, Hoekstra HJ, Meerman te GJ, Berg van de E. Computerassisted cytogenetic analysis of 51 malignant peripheral nerve sheath tumors: sporadic vs. neurofibromatosis type 1-associated malignant schwannomas. Int J Cancer 1999; 83: 171-178. 14. Plaat BEC, Muntinghe FLH, Molenaar WM, et al. Clinical outcome of patients with previously 78 15. 16. 17. 18. 19. 20. 21. 22. 23. 24. 25. 26. 27. 28. 29. 30. 31. 32. 33. 34. Prognostic relevance of cytogenetic changes in soft tissue sarcomas Chapter 6 untreated soft tissue sarcomas in relation to tumor grade, DNA ploidy and karyotype. Int J Cancer 1997; 74: 396-402. ISCN (1995): An International System for Human Cytogenetic Nomenclature. F. Mitelman (ed); S. Karger, Basel, 1995. Sandberg AA, Turc Carel C. The cytogenetics of solid tumors. Relation to diagnosis, classification and pathology. Cancer 1987; 59: 387-395. Heim S and Mitelman F. (eds.) Cancer Cytogenetics, 2nd ed. New York, Wiley-Liss, 1995. Parris CN, Harris JD, Griffin DK, Cuthbert DK, Silcer AJ, Newbold RF. Functional evidence of novel tumor suppressor genes for cutaneous malignant melanoma. Cancer Res 1999; 59: 516-520. Hermsen MA, Baak JP, Meijer GA, et al. Genetic analysis of 53 lymph node-negative breast carcinomas by CGH and relation to clinical, pathological, morphometric, and DNA cytometric prognostic factors. J Pathol 1998; 186: 356-362. Tomizawa Y, Adachi J, Kohno T, et al. Prognostic significance of allelic imbalances on chromosome 9p in stage I non-small cell lung carcinoma. Clin Cancer Res 1999; 5: 1139-1146. Heyman M, Rasool O, Borgonovo-Brandter L, et al. Prognostic importance of p15INK4B and p16INK4A gene inactivation in childhood acute lymphocytic leukemia. J Clin Oncol 1996; 14: 1512-1520. Moch H, Presti Jr JC, Sauter G, Buchholz N, Jordan P, Mihatsch MJ, Waldman FM. Genetic aberrations detected by comparative genomic hybridization are associated with clinical outcome in renal cell carcinoma. Cancer Res 1996; 56: 27-30. Choong PFM, Mandahl N, Mertens F, et al. 19p+ marker chromosome correlates with relapse in malignant fibrous histiocytoma. Genes Chromosom Cancer 1996; 16: 88-93. Tarkkanen M, Elomaa I, Blomqvist C, et al. DNA sequence copy number increase at 8q: a potential new prognostic marker in high-grade osteosarcoma. Int J Cancer 1996; 84: 114-121. Sanjuan X, Sobel ME, Yang J, Merino MJ. Alveolar soft part sarcoma: the role of prognostic markers. Ann Diagn Pathol 2000; 4: 135-142. Bieche I, Champeme MH, Lidereau R. Loss and gain of distict regions of chromosome 1q in primary breast cancer. Clin Cancer Res 1995; 1: 123-127. Valeri A, Drelon A, Paiss T, et al. Genetic analysis of familial prostatic cancer: localization of a gene predisposing to prostatic cancer (PcaP) on chromosome 1q42.2-43. Prog Urol 1999; 9: 680-688. Suzuki A, Fukushige S, Nagase S, Ohuchi N, Satomi S, Horii A. Frequent gains on chromosomal arms 1q and/or 8q in endometrial cancer. Hum Genet 1997; 100: 629-636. Pietsch T, Koch A, Wiestler OD. Molecular genetic studies in medulloblastomas: evidence for tumor suppressor genes at the chromosomal regions 1q31-32 and 17p13. Klin Pediatr 1997; 209: 150-155. Szymanska J, Tarkkanen M, Wiklund T, et al. Gains and losses of DNA sequences in liposarcomas evaluated by comparative genomic hybridization. Genes Chromosom Cancer 1996; 15: 89-94. Lee JH, Welch DR. Suppression of metastasis in human breast carcinoma MDA-435 cells after transfection with the metastasis suppressor gene, KiSS-1. Cancer Res 1997; 57: 2384-2387. Gryfe R, Swallow C, Bapat B, Redston M, Gallinger S, Couture J. Molecular biology of colorectal cancer. Curr Probl Cancer 1997; 21: 233-300. Kitamura Y, Shimizu K, Tanaka S, Ito K, Emi M. Association of allelic loss on 1q, 4p, 7q, 9p, 9q, and 16q with postoperative death in papillary thyroid carcinoma. Clin Cancer Res 2000; 6: 1819-1825. Bell SM, Shaw M, Jou YS, Myers RM, Knowles MA. Identification and characterization of the human homologue of SH3BP2, an SH3 binding domain protein within a common region of deletion at 4p16.3 involved in bladder cancer. Genomics 1997; 44: 163-170. Chapter 6 Prognostic relevance of cytogenetic changes in soft tissue sarcomas 79 35. ODonovan M, Russell JM, OLeary JJ, Gillan JA, Lawler MP, Gaffney EF. Abl expression, tumour grade, and apoptosis in chondrosarcoma. Mol Pathol 1999; 52: 341-344. 36. Nakanishi H, Ohsawa M, Naka N, et al. Immunohistochemical detection of bcl-2 and p53 proteins and apoptosis in soft tissue sarcoma: their correlations with prognosis. Oncology 1997; 54: 238-244. 37. Nakanishi H, Wang XL, Imai FL, et al. Localization of novel tumor suppressor gene loci on chromosome 9p21-22 in oral cancer. Anticancer Res 1999; 19: 29-34. 38. Wei G, Antonescu CR, de Alava E, et al. Prognostic impact of INK4A deletion in Ewing sarcoma. Cancer 2000; 89: 793-799. 39. Arcellana-Panlilio MY, Egeler RM, Ujack E, Pinto A, Demetrick DJ, Robbins SM, Coppes MJ. Decreased expression of the INK4 family of cyclin-dependent kinase inhibitors in Wilms tumor. Genes Chromosom Cancer 2000; 29: 63-69. 40. Orlow I, Drobnjak M, Zhang ZF, Lewis J, Woodruff JM, Brennan MF, Cordon-Cardo C. Alterations of INK4A and INK4B genes in adult soft tissue sarcomas: effect on survival. J Natl Cancer Inst 1999; 91: 73-79. 41. Yao J, Pollock RE, Lang A, et al. Infrequent mutation of the p16/MTS1 gene and overexpression of cyclin-dependent kinase 4 in human primary soft tissue sarcoma. Clin Cancer Res 1998; 4: 1065-1070. 42. Meye A, Wurl P, Hinze R, et al. No p16INK4A/CDKN2/MTS1 mutations independent of p53 status in soft tissue sarcomas. J Pathol 1998; 184: 14-17. 43. Simons A, Schepens M, Jeuken J, et al. Frequent loss of 9p21 (p16(INK4A)) and other genomic imbalances in human malignant fibrous histiocytoma. Cancer Genet Cytogenet 2000; 118: 89-98. 44. Latres E, Drobnjak M, Pollack D, et al. Chromosome 17 abnormalities and TP53 mutations in adult soft tissue sarcomas. Am J Pathol 1994; 145: 345-355. 45. Dei Tos AP, Piccinin S, Doglioni C, Vukosavljevic T, Mentzel T, Boiocchi M, Fletcher CD. Molecular aberrations of the G1-S checkpoint in myxoid and round cell liposarcoma. Am J Pathol 1997; 151: 1531-1539. 46. Mousses S, McAuley L, Bell RS, Kandel R, Andrulis IL. Molecular and immunohistochemical identification of p53 alterations in bone and soft tissue sarcomas. Mod Pathol 1996; 9: 1-6. 47. Liscia DS, Morizio R, Venesio T, Palenzona C, Donadio M, Callahan R. Prognostic significance of loss of heterozygosity at loci on chromosome 17p13.3-ter in sporadic breast cancer is evidence for a putative tumour suppressor gene. Br J Cancer 1999; 80: 821-826. 48. Borresen AL, Ottestad L, Gaustad A, et al. Amplification and protein over-expression of the neu/ HER-2/c-erbB-2 proto-oncogene in human breast carcinomas: relationship to loss of gene sequences on chromosome 17, family history and prognosis. Br J Cancer 1990; 62: 585-590. 49. Tran Y, Benbatoul K, Gorse K, Rempel S, Futreal A, Green M, Newsham I. Novel regions of allelic deletions on chromosome 18p in tumors of the lung, brain and breast. Oncogene 1998; 17: 3499-3505. 80 Prognostic relevance of cytogenetic changes in soft tissue sarcomas Chapter 6