Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Ligand binding assay wikipedia , lookup
Community fingerprinting wikipedia , lookup
Photosynthetic reaction centre wikipedia , lookup
Adenosine triphosphate wikipedia , lookup
NADH:ubiquinone oxidoreductase (H+-translocating) wikipedia , lookup
Fatty acid synthesis wikipedia , lookup
Amino acid synthesis wikipedia , lookup
Evolution of metal ions in biological systems wikipedia , lookup
Biosynthesis wikipedia , lookup
Lactate dehydrogenase wikipedia , lookup
Oxidative phosphorylation wikipedia , lookup
Nicotinamide adenine dinucleotide wikipedia , lookup
Citric acid cycle wikipedia , lookup
Biochemistry wikipedia , lookup
Cryopreservation wikipedia , lookup
I
CLIN. CHEM. 36/9, 1605-1613
Triglyceride
(1990)
Measurements:
a Review
of Methods
and Interferences
SIgrid G. Klotzsch1 and JudIth R. McNamara2
The
National
Cholesterol
Education
Program
has empha-
sized the need to identify
individuals
at risk for coronary
artery disease
(CAD). Because
increased
triglycerides
may
be a risk factor for CAD and because
triglycerides
are used
to estimate
concentrations
of low-density
lipoprotein
(LDL)
cholesterol,
which has definitely
been shown to be a risk
factor for CAD, it is important
that reliable
results
be obtained. Many methods
are available
for measuring
triglyceride concentrations
in serum or plasma,
but there is no
definitive method that confirms
the reliability of any of these
procedures.
Accuracy and precision guidelines are extremely
difficult to determine,
owing to broad biological
variability
both within and among individuals.
Here, we review the major
triglyceride
quantification
methods in the literature, some of
the potential interference
problems,
and the limitations
regarding
standardization
that should be addressed
when
establishing
such guidelines.
Assessment
of the Needs for Accuracy
in Triglyceride
Quantification
The
and Precision
National
Cholesterol
Education
Program
Adult
has recommended
that triglyceride
concentrations
<2.82 mmol/L (<2.50 gIL) be classified as
desirable, 2.82-5.65
mmol/L
(2.50-5.00
g/L) as borderline,
and >5.65 mmol/L
(>5.00 g/L) as distinctly abnormal (1).
These ranges are relatively broad, but it has been difficult
to assign specific concentrations
at which medical intervenTreatment
Panel
hon is recommended
because
of controversy
regarding
the
role of triglycerides
in coronary
artery disease
(CAD).3 The
association
of triglycerides
with CAD has been variable
in
population
studies
that evaluated
triglyceride
concentration as an independent
risk factor (2, 3).
If triglyceride
concentrations
in serum were not considered to be an important
risk
factor
for CAD,
if only
extremely
high concentrations
were felt to be important
in
terms
of diagnostic
value,
or if low-density
lipoprotein
(LDL)
cholesterol
concentrations
could easily
be deterrnned independently
of triglycerides,
then efforts toward
tandardization
of laboratory
methodology
might
not be
Lecessary. If, however,
triglyceride
concentrations
do mdiate some degree of risk, even if only in a certain
subset of
ndividuals
(4, 5), and if triglyceride
concentrations
coninue to be a necessary
tool for estimating
LDL cholesterol
6-B), then it is important
to eliminate
as much
assay
‘Technicon
Instruments
own, NY 10591-5097.
2Upid
Metabolism
Corp.,
Laboratory,
Division
USDA
of Miles,
Human
Inc.,
Nutrition
Tarry-
Re-
earch Center on Aging, Tufts University,
Boston, MA.
3Nonstandard
abbreviations:
CAD, coronary
artery disease;
DC, Centers for Disease Control;
BSA, bovine serum albumin;
nd GPO, glycerol-3-phosphate
oxidase.
Received October 1989; accepted June 22, 1990.
variability
as possible.
In the laboratory,
this means reduction of inaccuracy
and imprecision
to values
comparable
with
those for cholesterol.
In patient
management
this
means setting
fasting
times and pretesting
dietary
guidelines to minimize
biological
variation.
It also means careful
interpretation
of laboratory
results
(6, 9, 10).
Defining
the reliability
required
for any triglyceride
method
being considered
for laboratory
standardization
is
difficult,
because biological
variability
of triglyceride
concentrations
differs greatly
among individuals
(11, 12). Our
studies show marked
differences
among subjects
receiving
the same amount
of fat per kilogram
of body weight (12). In
addition,
some individuals
show variability
in their fasting
triglyceride
concentrations
when sampled on different
days
within
a short period (unpublished
data, J.R.M).
The ubiquitous
nature
of glycerol
interference
must be
taken
into account.
Glycerol
may derive from the sample
itself (13, 14) or from medications
given
to the patient
(15-19),
or samples,
sample cups, tubing,
etc., used in the
laboratory
may contain
traces
of lubricants
that cause
glycerol
interference
(20). The amount
of glycerol present
in skin-care
products
is not negligible
(21, 22). A sample
probe in a random-access
analyzer
aspirating
5 .iL of
sample,
equivalent
to an average
of 0.5 ng of free glycerol
in the assay mixture,
is conceivably
delivering
extraneous
glycerol
or glycol exceeding
this amount
into the system.
As a first step toward a critical evaluation
of triglyceride
determinations
we have reviewed
available
methodology,
interferences,
and standardization
limitations.
History
and
Principal
Methods
Early analytical
methods for determining
triglycerides
involved titrimetric
procedures
of total lipids. After extraction with
organic
solvents,
extracts
were saponified
and
then back-titrated
to assess the amount
of alkali
that was
not neutralized
by the released
fatty acids. Later methods
quantified
the glycerol
that was formed
(see Table 1), as
first described
by Van Handel
and Zilversmit
(23), who
extracted
the lipids with chloroform,
removed
phospholipids by adsorption
on silicic
acid, and then saponified
the
glyceride
esters to glycerol.
They determined
glycerol
by
oxidation
with
periodate,
using a colorimetric
measurement of the product
from the reaction
of formaldehyde
and
chromotropic
acid in sulfuric
acid. Although
some monoand diglycerides
of fatty acids are present
in serum (-3%),
results
were calculated
as “triglycerides.”
Subsequently,
the term triglycerides
was commonly
used for the total of
free and protein-bound
glyceride
esters.
Kessler
and Lederer
(24) adapted
this method
to the
AutoAnalyzer#{174}
(Technicon,
Tarrytown,
NY). They used
isopropanol
extracts
of serum,
added zeolite/Lloyd’s
reagent
to adsorb phospholipids
and other interferences,
and
then introduced
an on-line saponification
step. The glycerol
reacted with periodate
and produced
formaldehyde,
which
CLINICAL
CHEMISTRY,
Vol. 36, No. 9, 1990
1605
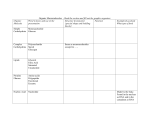
Table
1. Principles
of Analyses
Reference
23
24
25
26
Principle
extracted with organic solvents;
removed by adsorption
2. Triglycerides
ROH/OH
+
H2S04
+
-e
ary
H20
+
-e
3, 5-diacetyl-
+ ATP
glycerol 3-phosphate
3-phosphate
+ NAD
G3pDH
1.,2.
dihydroxyacetone
as above
4. ADP
+
phosphate
ATP
glycerol
PEP
+
5. Pyruvate
+
ATP
NADH
H
+
3-phosphate
glycerol
lactate
H
+
+
ADP
NAD
3-phosphate
NAD
+
phosphate
INT
+
+
ADP
pyruvate
H* !i
3-phosphate
dihydroxyacetone
5. NADH
+
+
1., 2. as above
3. Glycerol + ATP
4. Glycerol
+ NADH
+
G.3PDI
NADH
+
NAD
diaphoras
Modification
of ref. 27, elimination
1. Triglycerides
S
glycerol
+
+
+
ADP
H
INT(reduced)
of adsorption
step
2. Glycerol + ATP
glycerol 3-phosphate
+ ADP
3. ADP + PEP
ATP + pyruvate
4. Pyruvate
+ NADH + H
!!i lactate + NAD
35
1. Triglycerides
2. Glycerol
+
E!!3
glycerol
ATP
glycerol
3-phosphate
+
ADP
3. Glycerol 3-phosphate
+ NAD
03-PDIt
dihydroxyacetone
phosphate
#{247}
NADH + H
4. NADH + H + INT diaphoraee
NAD + INT(reduced)
36
1., 2. as above
3. Glycerol
+
NAD
dehydrOgefla3
glycerOl
37
dihydroxyacetone
+ NADH
1. Triglycerides
!!E5f glycerol
38
2. Glycerol + NAD
dihydroxyacetone
1., 2. as above
39
3. NADH + H
1. Triglycerides
2. Glycerol
glyol
+
dohydrogonas1
+ resazurin
!!2
glycerol
+ 02
glycerol
+ H
NADH
+
diaphoras
H
NAD
dihydroxyacetone
oxldasq
+ resorufin
41
+ phenol derivative
chromophore
1. H202
1. Triglycerides
!!E2
+
4-aminoantipyrine
t!9
glycerol
2. Glycerol + ATP
glycerol 3-phosphate
+ ADP
3. Glycerol 3-phosphate
+ 02 GPQ dihydroxyacetone
phosphate
+ H202
4. H202 + 3,5-dichloro-2-hydroxybenzene
sulfonate
4-aminoantipynne
!i
chromophore
+
GK, glycerol kinase; G-3-O-PDH, glycerol-3-phosphate
dehydrogenase;
PEP, phosphoenok,yruvate; PK, pyruvate kinase; LDH, lactate dehyrogenase;
HPO, horseradish peroxidase; and INT, 2-(4-iodophenyl)-3-(4-nitrophenyl)-5phenyltetrazolium
chloride.
measured
fluorometrically
after a Hantzsch-type
condensation
with diacetylacetone
and ammonia.
Carlson and Wadstr#{246}m’smodification
(25) of the above
methods became the procedure used by the Lipid Research
was
1606
CLINICAL
CHEMISTRY,
Vol. 36, No. 9, 1990
accuracy
and
reference,
calibration
good
The assay was standardized
by
Control
(CDC)-National
Heart,
Lipid Standardization
Program
precision
make
but only CDC
material
that
has
this
calibrators,
been
procedure
an
or a second.
analyzed
by
the
lipase together
with a protease,
instead
ysis. This procedure
became
the most
technique
for determining
triglycerides.
of chemical
hydrolpopular
ultraviolet
It could be used
with most manual
and automated
laboratory
instruments
and received
widespread
recognition
in clinical
laboratories. Free glycerol
could be blanked
by a separate
assay
with use of reagents
without
lipase or glycerol
kinase. The
colorimetric
method
of Klotzsch
et al. (28), in conjunction
with lipase instead
of chemical
hydrolysis,
was publish
by Megraw
et al. (35) and became a convenient
techniqu
for use with centrifugal
analyzers
and other medium-si
+
H202
40
studies.
CDC method, can be used if interlaboratory
results are te
be compared.
The various analytical
steps require a high
degree of technical
competence.
The measurement
of glycerol by an enzymatic
spectro
photometric
procedure
was introduced
by Wieland
(26
after the enzyme glycerol kinase (ATP:glycerol
3-phospho.
transferase;
EC 2.7.1.30)
became commercially
available,
Eggstein
and Kreutz
(27) used the reverse enzymatic
reac
tion, after a chemical
saponification
step, to assay neutra]
fats. Both methods
are based on the oxidation!
reduction
ol
NADH!NAD
and the corresponding
change
in absor.
bance. Chemical
saponification
is usually
performed
in an
alkaline
medium,
with subsequent
neutralization
by per.
chlorate
or magnesium
sulfate
(42), whereby
most proteine
are inactivated.
Phospholipids
are also hydrolyzed,
which
necessitates
adsorption
on zeolite if the Wieland
method if
used, because
the subsequent
step quantifies
the glycerol
3-phosphate
produced.
A semiautomated
enzymatic
analysis, introduced
by Klotzsch et al. (28), added a colorimetric
indicator
reaction
to the Wieland
principle
and introduced
the method to the AutoAnalyzer.
The colorimetric
reaction took place after samples
were
subjected
to the adsorption
step with zeolite, before on-line
saponification
with alcoholic
KOH.
This step eliminated
interference
from endogenous
alkaline
phosphatase
(EC
3.1.3.1) and lactate dehydrogenase
(EC 1.1.1.27).
However,
the technique
did not save much time by automation
and
was later improved
by Stavropoulos
and Crouch (29-31).
They avoided extraction
and adsorption
by combining
alcoholic base saponification
with the precipitation
technique
o
Schmidt
and von Dahl (42) using
magnesium
salts. Chernick
(43) claimed
that the use of tetraethylan,moniuni
hydroxide
hydrolyzed
triglycerides
without
cleavage of phospholipids.
Bucolo
and David
(32-34) substantially
improved
the
ultraviolet
test of Eggstein
and Kreutz
by using microbial
1., 2. as above
3. Glycerol
29-31
32-34
HCOOH
+
4. HCHO + NH4 + acetylacetone
1 ,4-dihydrolutidine
(fluorescent)
1-4. as above, modified
4. Glycerol
28
High
excellent
glycerol
3. Glycerol + l04
-e
HCHO
103
4. HCHO + chromotropic
acid
chromophore
1 .-3. as above, modified
population
the Centers
for Disease
Lung, and Blood Institute
of assay
1. Triglycerides
phospholipids
3. Glycerol
27
Clinics
for Triglycerides
instruments
(44).
The
enzyme
glycerol
dehydrogenase
2-oxidoreductase,
EC 1.1.1.6)
was introduced
Hagen (45) in 1962, when it was suggested
(glycerol:NAD
by Hagen
an
for determinin
(36) extended this principl
et al. (37) and Grossman
e
glycerol.
Bowie and Gochman
to triglyceride
assays. Rautela
al. (46) modified
it to be applied
to the aca#{174}
(Du Pon
Instruments,
Wilmington,
DE) and CentrifiChem#{174} (Bake
Instruments,
Evansville,
WI).
Because
the equilibrium
of the enzymatic
reaction
i
unfavorable
to the production
of dihydroxyacetone,
a ki
netic (pseudo-first-order)
mode was chosen to overcome
th
time constraints
of the instruments.
Sigiura
et al. (47)
modified
the reaction
for a colorimetric
measurement
in
combination
with a tetrazolium
salt; Winartasaputra
et al.
(38) introduced
the reaction
for fluorometric
assays.
During
the following
years, many additional
modifications were made to apply the enzymatic
methods
to the
newly
developed
automated
laboratory
instrumentation
(38,48-53).
When glycerol
oxidase (glycerol:oxygen
oxidoreductase;
EC not assigned)
became
available,
a new approach was presented.
Terada
et al. (39, 54) and Gauhl et
al. (55) combined
the oxidase
reaction
with the reaction
sequence
of Trinder
(40), which
coupled
peroxidase
to a
phenol
derivative
and 4-aminoantipyrine.
Glycerol
oxidase, however,
is nonspecific
and reacts with many glycols,
such as ethylene
glycol and propylene
glycol (16). Greater
specificity
was achieved
by oxidative
phosphorylation.
Fossati and Prencipe
(41) and McGowan
et al. (56) used the
enzyme
glycerol-3-phosphate
oxidase
(GPO; sn-glycerol-3phosphate:oxygen
2-oxidoreductase,
BC 1.1.3.2 1) in conjunction
with a Trinder-type
reaction.
This method continued to be modified
as its application
to new instruments
nurtured
innovative
changes
(57).
Other methods
have been developed,
such as bioluminescence assays
(58), but have not become
popular,
either
because of improper
blanking
that results in poor precision
or because
commercial
availability
has been limited.
An
HPLC procedure
based on adsorption
chromatography
and
refractive
index
detection
of triglycerides,
presented
by
Ambrose
and Smith
(59), appears
to be highly
specific
because
it does not include
di- or monoglycerides
in the
measurements.
The method has its constraints,
owing to
the instrumentation
and the time required,
but may be
worth considering
as a reference
procedure.
Factors
Problems
Affecting
Test Results
with Chemical
The hydrolysis
can be achieved
Saponification
Methods
of triglycerides
to glycerol and fatty acids
by chemical
saponification,
in which the
sample
is treated
with alcoholic
KOH or NaOH
at high
temperatures
and subsequently
neutralized
with magnesium sulfate. Enzymes
in the samples are inactivated
and
fatty acids are coprecipitated
as magnesium
salts. After
centrifugation,
the clear supernate
is used for the assay
(42). Ascorbate
and other unstable
compounds,
such as
conjugated
bilirubin,
are decreased
or eliminated
simply by
controlling
the time in which
the sample
is subjected
to
eat and alkali.
However,
glucose, lactate,
hydroxybutyrate,
and residal alcohol remain
candidates
for potential
interference.
hospholipids
are hydrolyzed
to glycerophosphates,
which
stable in alkaline
solutions.
Only those methods
that
easure
the formation
of glycerol
3-phosphate
require
heir removal
by adsorption,
unless
the procedures
of
tavropoulos
and Crouch (29) or Chernick
(43) are used.
echnical
problems
are mainly related to the high temperture, the caustic nature
of the reagents involved,
and the
ength of time. The temperature
inside the sample tubes
not the water bath) must be the same for calibrator
and
lank; the length of time required
varies with the tempertore and must be equal for each sample within
a series.
e stoppers of the sample tubes must be vented to avoid
reakage,
but evaporation
of the alcohol must be preented. The subsequent
precipitation
of Mg(OH)2
causes
olume displacement
of the liquid from which an aliquot is
taken for further testing. The reagent blank must include
the saponification
step because preparations
of KOH are
not always
free of glycerol.
The volume
of magnesium
sulfate
needed to neutralize
the alcoholic
base in aqueous
solutions
(reagent
blanks
and calibrators)
is different
for
proteinaceous
samples.
To keep all volumes
the same, it is
advisable
to add fatty acid-free
bovine
serum albumin
(BSA), 60 mg/mL,
to blanks and calibrators.
Problems
with Enzymatic
Cleavage
of Triglycerides
Choosing
the best lipase (triacylglycerol
acylhydrolase;
EC 3.1.1.3) requires
selection from a wide variety
of commercially
available
preparations.
We have found that the
source of lipase determines
the rate and degree of lipolysis:
lipase from Chromobacterium
sp. acts with
higher specificity toward
the glycerides
of long-chain
fatty
acids,
whereas the lipase from Pseudomonas
sp. hydrolyzes
the
short-chain
esters much faster. Microbial
lipases on the
market have distinct properties,
and use of several sources
may yield the best results for a specific instrument
application (60-62).
Lipases require emulsified
substrates,
rather than true
solutions,
which explains
the different
rates of hydrolysis
for tn-, di-, and monoglycerides.
Many substances
can act
as emulsifiers,
but lipase preparations
that are inhibited
by
specific surfactants
such as Triton#{174} (Rohm
and Haas,
Philadelphia,
PA) are offered commercially.
Other lipase
preparations
are markedly
activated
by such non-ionic
surfactants,
by bile acids, and by lauramide
or cocoamide
esters. Furthermore,
the effects of mono- and divalent
ions
need to be tested because various
lipases depend on either
potassium,
calcium, or magnesium
ions for optimal performance. Instead of surfactants,
BSA has been suggested as
an emusifier
for lipid micelles (32).
The presence
of a colipase
is not required
for these
assays. Colipase,
a pancreatic
protein, negates the inhibition of pancreatic
lipase by bile acids (63). In contrast,
the
microbial
lipases used for triglyceride
determinations
are
not inhibited,
but activated,
by bile acids.
Esterase
in the lipase mixture
(for instance,
carboxylesterase,
EC 3.1.1.1; or triacylglycero-protein
acyihydrolase, EC 3.1.1.34)
increases
the rate of hydrolysis
(64, 65).
Microbial
lipases generally
exhibit
both lipolytic
and hydrolytic
activity,
which
are stimulated
by proteases,
e.g.,
chymotrypsin
(EC 3.4.21.1),
as demonstrated
by Bucolo
and David
(32). The presence
of proteases
can have a
negative
effect
on the stability
of a reagent
solution.
Digesting
proteases
can attack
other enzymes
in the assay
system,
leading
to poor stability
of glycerol
kinase
and
pyruvate
kinase at pH 7.0.
Interference
from
Extraneous
Sources:
Reagents
Manufacturers
of enzymes
and biochemical
substrates
offer products
of refined purity
(66); however,
they cannot
predict
the use of a particular
reagent
component
in a
specific assay system. Although
a listed contamination
of
0.01% may not appear to be significant,
its effects may
accumulate
when three or four enzymes
are used in a
reaction sequence.
The following
interferents
(in alphabetical order) have been detected
in our laboratory
and can be
present in commercially
available
materials.
Adenylate
kinase:
ATP:AMP
phosphotransferase
(EC
2.7.4.3)
can be a contaminant
in glycerol
kinase
(EC
2.7.1.30),
lactate
dehydrogenase
(EC 1.1.1.27),
pyruvate
kinase
(EC 2.7.1.40),
and glycerol-3-phosphate
dehydrogeCLINICAL
CHEMISTRY,
Vol. 36, No. 9, 1990
1607
nase (NAD)
(EC 1.1.1.8).
Depending
on the assay
conditions, interference
results
from the formation
of ADP,
which
reacts
with the AMP present in ATP. (AMP
is a
normal
contaminant
in ATP.)
Adenosine
5-diphosphate:
ADP is present
in APP, especially
if reagent
solutions
are stored or if ATP has been
processed
with other reagents
such as in a lyophilized
product.
ADP
can also be generated
by the action of
alkaline
phosphatase
at pH 7.0-9.0.
Its effect can be negated with a reagent
blank;
but consumption
of NADH
during
pre-incubation
reduces the dynamic
range of the
reaction,
and samples with high concentrations
of alkaline
phosphatase
may no longer give results that are in the
linear range of the assay, in the presence of this contaminant.
Akohol
dehydrogenase:
Alcohol:NAD
oxidoreductase
(EC 1.1.1.1)
is a likely
contaminant
of enzymes
isolated
from yeast. Its presence in glycerol kinase from Candida
sp. can produce a side reaction
with NAD
and alcohol that
is carried
over from chemical
saponification
or introduced
as a contaminant
in NAD.
If blanking
is performed
without glycerol kinase, the total assay will produce falsely
high (NAD-coupled
reactions)
or falsely
low (NADHdependent
reactions)
values.
Alkaline
phosphatase:
Orthophosphoric-monoester
phosphohydrolase
or nonspecific
phosphatases
are the most
significant
and severe interferents
in triglyceride
assays,
regardless
of methodology.
Alkaline
phosphatase
activity
is found
primarily
in lipase,
but some contamination
in
other
enzymes
is possible.
Alkaline
phosphatase
reacts
with glycerophosphate,
dihydroxyacetone
phosphate,
phosphoenolpyruvate,
and APP at neutral
or alkaline
pH and
can be inhibited
by EDTA
and phosphates
(67).
Catalase:
Hydrogen-peroxide:hydrogen-peroxide
oxidoreductase
(EC 1.11.1.6)
is a contaminant
present in oxidases and will, therefore,
affect assays based on the Trinder
sequence, where glycerol oxidase or glycerophosphate
oxidase is utilized.
Because
catalase
competes
with peroxidase
(donor:hydrogen-peroxide
oxidoreductase,
EC 1.11.1.7)
for
H2O2, interference
is less when test conditions
are optimal
for peroxidase,
with regard to pH and hydrogen
donor.
Ethylene
glycol:
Propylene
glycol and other glycols react
nonspecifically
with glycerol oxidase, which is used in the
method developed
by Terada
et al. (39), and give falsely
high values. Ethylene
glycol is frequently
used to stabilize
control sera.
Hexokinase:
ATP:D-hexose
6-phosphotransferase
(EC
2.7.1.1)
can be present
in yeast enzymes,
especially
in
glycerol
kinase from Candida
sp. Its presence results in
falsely high values for the ultraviolet
method with pyruvate kinase
(EC 2.7.1.40)
and lactate dehydrogenase,
because hexokinase
will generate
additional
ADP from serum glucose and ATP.
Lactate
dehydrogenase:
(S)-Lactate:NAD
oxidoreductase, a trace contaminant
in most enzymes,
will interfere
with the INT/diaphorase
method if present in glycerol-3phosphate
dehydrogenase,
or with the direct glycerol dehydrogenase
method with NAD,
because it reacts at a slow
rate with lactate
and hydroxybutyrate
in serum (68). The
interference
caused by this reaction
is masked if the rate
techniques
measure
apparent
pseudo-first-order
kinetics.
NADH-oxidase:
“NADH-oxidase”
refers
to nonspecific
activities
in the presence of coenzyme.
NADH,
for instance,
can be oxidized
at a slow rate without
any apparent
substrate.
NADH-oxidase,
which is often listed in manu1608
CLINICAL
CHEMISTRY,
Vol. 36, No. 9, 1990
facturers’
certificates
of analysis, is always associated
with
dehydrogenases
and need not be a separate
protein.
Although
very low rates may not contribute
to a significant
bias,
accumulation
of several
substances
that
oxidize
NADH
should be avoided.
Oxidases:
Oxidases,
namely
glucose oxidase (EC 1.1.3.4),
lactate
oxidase
(BC 1.13.12.4),
and pyruvate
oxidase
(EC
1.2.3.3), must be absent in preparations
of GPO to avoid
interference
with the Trinder
reaction.
If the reaction
is
initiated
with glycerol
kinase or lipase, the normal
preincubation
time of approximately
5 mm with GPO may not
be sufficient to remove endogenous
glucose and lactic acid
that generate
additional
H2O2.
Peroxidase:
Peroxidase
reacts
nonspecifically
with
NADH,
and the rate is increased
by ketoacids,
e.g., ketobutyrate
(unpublished
data, S.G.K.).
In a single-cuvet
sequential
determination
of triglycerides
and cholesterol
(69,
70), a significant
side reaction can be seen in samples from
patients
with ketoacidosis,
because
the NADH-coupled
triglyceride
reaction mixture
contains
the peroxidase
necessary
for the Trinder-type
cholesterol
assay.
Peroxides:
Peroxides
are frequently
found in surfactants
and contribute
to the pink color that forms during
storage
of reagents
for assays based
on the Trinder-type
reaction,
but they do not interfere
if the reagents
are blanked
correctly.
Phospholipase:
Phosphatidylcholine
cholinephosphohydrolase (BC 3.1.4.3) and phosphodiesterase
(sn-glycerol-3phosphorylcholine
glycero-phosphatehydrolase,
EC 3.1.4.2)
in lipase preparations
act on phospholipids
and, in conjunction with phosphatase,
result in falsely high values for
incorrectly
blanked
triglyceride
assay. Mainly
diglycerides
are generated
from phosphatidylcholine;
therefore,
it is
advisable
to test the lipase mixture
for nonspecific
activity
before use.
Pyruvate:
Pyruvate
is a breakdown
product of phosphoenolpyruvate
and can be present in the reaction mixture.
It
contributes
to NADH
consumption
before the start of the
glycerol reaction;
thus the amount
of NADH
present may
not be sufficient to assure the range of linearity.
Quantities
of enzyme:
Quantities
of enzyme used for the
assays are of great importance.
All contaminants
that may
be present in commercial
materials
can be additive.
Use of
too little enzyme, or too much, increases the possibility
for
failure. Enzymes
stored for a long period may lose activity.
If the loss of activity
is compensated
for by the use of
increased amounts of raw material,
the contaminants
may
be correspondingly
increased.
Contaminants
can be more
stable than host enzymes.
interference
from Endogenous
Substances
in Serum
As stated
previously,
the routine
determination
of tri
glycerides without extraction
or deproteinization
may trig
ger endogenous
substances
that cause interference
in th
reaction.
Interference
may not always cause a significan
bias, but this potential
problem should be anticipated
whe
processing
patients’
samples.
Alcohol/alcohol
dehydrogenase,
lactate/lactate
dehydroge
nase, and glycerol/glycerol
dehydrogenase:
These
enzyme
and their substrates
are often increased
in serum or plas
specimens
from patients
with liver diseases
or with my
cardial
infarctionlischemia
(71). They can cause a slow
steady increase
in absorbance
with all methods that util
NAD
and alkaline
conditions,
because the reaction is no
completed
within
the normal pre-incubation
time. Interfer
ence can be negated by analyzing
serum blanks
at the same
time and temperature.
Alkaline
phosphatase:
Alkaline
phosphatase
significantly
interferes
with all methods,
whether
as a contaminant of the reagent
preparations,
as previously
discussed,
or as increased
concentrations
in the specimens.
Specimens
with increased
concentrations
of this enzyme require
special attention
(e.g., pediatric
samples).
Triglyceride
results
may become apparently
increased
owing
to hydrolysis
of
phosphoenolpyruvate
in the ultraviolet
assay involving
lactate dehydrogenase
and pyruvate
kinase,
or to hydrolysis of glycerol
phosphate
or dihydroxyacetone
phosphate
in
other procedures.
The degree of interference
depends
on
individual
assay conditions
and whether
serum
blanks
have been included.
Although
alkaline
phosphatase
activity is optimally
measured
at alkaline
pH, its activity
at pH
7.0 is significant
(67). As mentioned
previously,
phosphate
ions and EDTA inhibit
the activity of alkaline
phosphatase
and are, therefore,
often included
in commercial
formulations.
Ascorbic
acid:
Ascorbic
acid interferes
with
methods
involving
2-(4-iodophenyl)-3-(4-nitrophenyl)-5-phenyltetrazolium
chloride
with diaphorase
(EC 1.6.4.3), by decolorizing the formazan,
and in the Trinder
method, by reacting
nonspecifically
as a hydrogen
donor in the peroxidasecatalyzed
reaction.
Ascorbate
oxidase
(L-ascorbate:oxygen
oxidoreductase,
BC 1.10.3.3) added to the reagents
effectively removes
this interference,
provided
the enzyme
is
pure and does not generate
H202 (72). (Contrary
to most
oxidases,
ascorbate
oxidase
generates
H20, not H202.)
Ascorbate
oxidase
need not be added in routine assays,
because the small amount
of ascorbate
ordinarily
found in
the assay mixture
can be disregarded.
The threshold
limit
of ascorbate excretion
is about 0.1 mmol/L,
the interference
from which
is equivalent
to only 5% of the upper normal
triglyceride
concentration.
Serum-blanked
methods
are not
affected.
Bilirubin: Bilirubin
interference
with colorimetric
methods is well documented
and presents
a potentially
serious
problem
(73). The interference
is probably
both spectral
and chemical
and will be different
for conjugated
and
unconjugated
bilirubin
(74). Bilirubin
is oxidized
in a
kinetic
reaction
with H202, and its decrease
in absorbance
is superimposed
on the main triglyceride
reaction.
A serum
blank
does not compensate
sufficiently
because
the subtrate,
H202, is not formed from free glycerol
in equivalent
ounts.
The various chromogens
used for the peroxidase-coupled
says are affected
differently
by the bilirubin
side-reacSon; some are less susceptible
to the interference
than
there, presumably
because of a higher affinity
of peroxifor the chromogen
(75). The addition
of ferrocyamide
ons has shown various
degrees of success, depending
on
e chromogens,
pH, and spectral
wavelength
used for
easurements
(76). Adding
bilirubin
oxidase
appears
to
ye inherently
better
results and should be considered
as a
retreatment
for icteric
samples (77).
Bilirubin
does not interfere
with ultraviolet
methods
hen measured
with
precision
spectrophotometers
vs
lanks, because NADH
has a much lower oxidation
potenal than does H2O2. Bichromatic
readings
in some instruents, however, do not provide sufficient
spectral
accuracy.
e absorbance
of NADH
at 380 nm lies within
a spectral
houlder
extending
from 340 to 400 nm. This spectral
nsitivity
can result in apparent
interference.
The ab-
sorbance of unbound bilirubin
peaks at around
420 nm and
is still measurable
at the range
of 380-400
nm. The
overlapping
spectra of icteric samples are often not considered in the calculation
of a bichromatic
factor.
Alkaline
and acid phosphatases:
Phosphatases
that originate from erythrocytes
may liberate glycerol from glycerol
esters and cause chemical
interference
during hemolysis.
Also, spectral interference
occurs in some of the colorimetric methods if no serum blank is performed.
Phospholipids:
Phospholipids
from
erythrocyte
membranes can also cause falsely increased
triglyceride
values
in unblanked
assays.
This will occur particularly
when
there is a delay in separation
of the serum from the clot
through
the action of phosphoesterases.
Uric acid: Uric acid has been reported
as an interferent
in the Trinder
reaction
(78). Peroxidase
reacts nonspecifically with many reducing compounds as a hydrogen
donor;
thus increased
uric acid concentrations,
as well as ascorbic
acid, will affect the results of unblanked
techniques.
Problems
in Laboratory
Technique
Plasma:
Plasma
treated
with heparin
or EDTA
can be
used for the triglyceride
assay, provided that most platelets
have been removed.
Platelet
membranes
will rupture
in
the presence of surfactant
and will release
alkaline
phosphatase
and lactate
dehydrogenase
into the assay mixture
(79).
Highly
lipemic
specimens:
Highly
lipemic
specimens
contain enough chylomicrons
to agglomerate
as a layer on top
of the samples.
If sample cups for automated
instruments
are left in the waiting
position for more than 30 mm, the
samples are no longer homogeneous.
Lipemia
also interferes if no “clearing
factor” is used, namely,
if the sample
blank solution
does not contain
agents to solubilize
the
lipid micelles. This effect is not always visible, and considerable light scattering
can be measured
even if the cuvets
appear to be clear. Patents
exist that claim removal
of
turbidity
from lipids and (or) proteins by surfactants
(64,
80-82);
however, the degree to which surfactants
can clear
lipids completely,
with no optical interference,
has been
challenged
(83).
Triglyceride
concentrations
measured
by the GPO-coupled reaction
reportedly
are decreased
in grossly
lipemic
samples
because of rapid oxygen utilization
that, through
producing
a temporarily
anaerobic
environment,
leads ultimately
to decreased
color generation
(84). Similar
results
were obtained
in the laboratory
of one of us (unpublished
data, S.G.K.) with the use of the Cobas-Bio
centrifugal
analyzer
(Roche
Diagnostic
Systems,
Nutley,
NJ) but not
when measurements
were taken in a manual
spectrophotometer. Adding a liquid with high oxygen retention,
such
as a fluorocarbon,
can eliminate
the problem.
Hydrazine
-containing
buffers:
Hydrazine-containing
buffers are sometimes
advocated
for methods
based on the
reduction
of NAD
in alkaline
pH ranges (28). The rationale is to trap the aldehyde
group of the product,
dihydroxyacetone
phosphate
(or dihydroxyacetone),
in order to
achieve
a more
favorable
equilibrium.
However,
NAD
and hydrazine
form an ultraviolet-absorbing
complex
and
generate
a steady
increase
in absorbance
(“creep-reaction”). Tris is a better agent for trapping
aldehyde
groups.
Creep-reactions:
“Creep-reactions”
are those in which the
absorbance
of a reaction mixture
continues
to change
after
the main
reaction
has reached
an endpoint.
These
are
definite
signs of side reactions
and are not obvious
in
CLINICAL
CHEMISTRY,
Vol. 36, No. 9, 1990
1609
automated
instruments.
Test results can be either positively or negatively
affected.
The validation
of new test
reagents
should
include
an experiment
that traces absorbance time on a recording
spectrophotometer,
with use of a
known
serum sample or standard.
Blanks:
Rate measurements
based on pseudo-zero-order
kinetics
have the obvious advantage
of not needing to be
blanked,
but will mask all creep reactions
caused
by
extraneous
or endogenous
sources. Enzyme
inhibitors
may
be added to increase the apparentK
of glycerol kinase (85,
86) and to provide surplus
enzyme
activity,
but contaminants may not be inhibited.
Endpoint
assays determine
the
absorbance
of sample-reagent
mixtures
before the reaction
has taken
place (incubation
with reagent
not containing
glycerol kinase or lipase) and again after the reaction has
been triggered
and has come to completion.
In this case,
contaminants
in the trigger
reagent
are not eliminated.
The most nearly accurate,
but certainly
the most expensive, blanking
technique
constitutes
a separate
serum
blank for each sample (87). The assay is performed
with the
complete
reagent
and then repeated
with
the reagent
lacking
lipase. This glycerol
blank,
however,
introduces
a
negative
error caused by the clearing
effect of lipase.
A
separate
free glycerol
blank
needs
to be performed
as a
serum blank
with glycerol
reagents,
lacking
glycerol
kinase, or with the lipase-containing
reagent,
lacking one of
the chromogenic
compounds.
The latter approach
was patented by Tsuda et al. (88) because of the obvious advantage
of introducing
sequential
analysis
to automated
instruments. The requirement
of a serum blank in addition
to a
free glycerol blank, described
by Artiss
et al. (83), stressed
that surfactants
alone clear turbidity
only partially,
when
the glycerol
blank
is assayed.
The sample
blank
is especially important
when special medications
have been administered
to the patient,
because absorbing
and (or) fluorescent compounds
may be present.
Davies et al. (89) found
that metronidazole
produced
a characteristic
spectrum
in
the ultraviolet
range. Later et al. (90) reported
a fluorescence of unknown
origin.
Hydroxyurea
has also been found
to inhibit glycerol oxidase (91).
The bichromatic
measurement
of triglyceride
assays
may be a good alternative,
but spectral
conditions
greatly
affect
the results.
The spectrum
of hemoglobin,
for instance,
changes
with
sample
handling.
While hemoglobin
has its major peak at 500 nm, the formation
of oxyhemoglobin decreases
the maximum
to 415 nm. Bilirubin,
if
unconjugated,
peaks at 460 nm; but in the presence
of
surfactants
that split the protein bonds, unbound
bilirubin
absorbs at 420 nm. Many
automated
instruments
use a
bichromatic
pair of 340/380 nm for ultraviolet
tests. If the
bandwidth
of the respective
filter is wide, considerable
absorbance
is measured
at 380 nm and thus affects
the
result, owing to the bilirubin
shift. The bichromatic
factor
is an arithmetic
mean of empirical
data from many assays;
it will correct for the majority
of specimens,
but not necessarily for abnormal
samples.
Sample-to-reagent
ratios:
Most laboratory
instruments
are preset by the manufacturer
with regard to sample and
reagent
volume,
wash volume
(if applicable),
and instrument settings. By keeping the sample fraction low, i.e., 0.01
(5 ML), endogenous
interfering
substances
are diluted,
so
that the actual
effect has minor significance.
The instrument readout, however, must include a high multiplication
factor. Errors caused by exogenous sources such as reagent
impurities
are then multiplied,
and the overall low sensi1610
CLINICAL
CHEMISTRY,
Vol. 36, No. 9, 1990
tivity
is reflected
in the imprecision
of the method.
Th
delicate balance between sample volume, sensitivity
of th
method, and instrument-related
optical fluctuation
must lx
taken into account when applying
specific methodology
t*
laboratory
equipment.
Glick and Ryder (92) show the effecl
of common serum indices such as hemolysis
and icterus or
results with various laboratory
instrumentation
when usec
as prescribed
by the manufacturers.
De-ionized water: De-ionized
water, when freshly taker
from a system, does not contain sufficient
oxygen for the
peroxidase-coupled
reactions.
The enzyme will display sub.
optimal
behavior
until all solutions
are oxygenated.
As e
result, calibration
factors
and blank values may change
during
the first day. Reagents
will equilibrate
during the
first 24 h, provided enough “headspace”
is given for absorb
ing oxygen from the air.
Drugs:
The direct
effects of drugs on the triglyceride
methods
have not been studied extensively.
Stored sample
from patients
receiving
intravenous
administration
of he.
parin have shown decreased
stability
of triglycerides,
witI
a corresponding
increase
in the concentration
of free glyc.
erol (19,93).
Other investigators
have claimed high appar.
ent concentrations
of triglycerides
when unblanked
tech.
niques were used, because
of increased
free glycerol
con
centrations
after treatment
with nitroglycerine
(18). A.
stated previously,
others have found interference
problem
under certain
conditions,
such as during
treatment
with
metronidazole
or hydroxyurea
(89-91).
Little research
date
on the effects of special patients’
specimens
are available,
e.g., those from uremic
patients,
pre- and postdialysis,
When
selecting
a triglyceride
method
and its technica]
application
(instrument
setting, blanks,
etc.), special atten
tion should be given to the expected
peculiarities
of the
patients
to be tested.
Calibrators:
A major problem for triglyceride
standardi.
zation is achieving
a consensus
on calibration
materials,
Because the end product of most triglyceride
reactions
i
free glycerol, glycerol itself has been used as a convenieni
calibrator.
Glycerol,
however,
can be considered
only a
primary
standard
for the indicator
reaction;
it is not the
analyte
itself and does not participate
in all steps of the
reaction.
Ideally,
a primary
triglyceride
standard
should
contain, in a pure, well-defined
medium,
triglycerides
rep.
resentative
of the average composition
and complexity
o
those found in adult humans.
Owing to the hydrophobi
nature
of triglycerides
and the complex packaging
of li
protein
particles,
a truly
parallel
primary
standard
probably not possible.
Triolein,
although
not entirely
representative
of hum
triglyceride
fatty acid composition,
has a similar
averag
chain length and is hydrolyzed
in the reaction
process
Because
triglycerides
in serum
contain
many fatty aci
with various
lengths
and numbers
of unsaturated
bonds
the rate and degree of hydrolysis
in any system will depen
on the esters involved
and on the ability
of the specifi
lipases in the reagent
to cleave them. The hydrolysis
o
oleate, although it represents
an average human fatty aci
will not be completely
representative
of the hydrolysis
o
all fatty acids. However,
it is probably
a reasonable
alte
native.
Another
alternative,
that of using
well-characte
secondary
standards,
has also been shown
to be accura
and precise
(94). Chromatographic
methods,
e.g., HP
could be used to validate
the hydrolysis
of serum-ba
secondary
standards
having
complex
fatty acid compo&
Lions. These
standard
materials
could
subsequently
be
analyzed
by methods
based
on the molar absorptivity
of a
reaction product (95). Storage
stability
of secondary
stanlards is of critical
importance,
because matrix
characterisLics may not be changed.
Improving
the accuracy
and precision
for determining
triglyceride
concentrations
is an important
component
in
identifying
individuals
at risk for CAD.
No definitive
method has been devised that can act as the “gold stanlard” by which all methodology,
reagents,
and calibrators
are judged. A protocol involving
a well-defined
reference
method that can be reliably
and reproducibly
performed
and that is resistant
to interfering
substances,
both endogenous and exogenous,
must be developed,
along with procedures to minimize
biological
variation
in sampling.
The
potential
methods,
interferents,
and limitations
discussed
here need to be evaluated
further before consistently
high
atandards
for measuring
triglyceride
concentrations
can be
established.
Ref erences
1. Expert
Program
Panel.
Expert
Report
of the National
Cholesterol
Education
Panel on detection, evaluation, and treatment of
high blood cholesterol
in adults.
Arch Intern Med 1988;148:36.-69.
2. Austin MA. Epidemiologic
associations
between hypertriglycaridemia and coronary
heart disease.
Semin
Thromb
Hemostas
1988;14:137-42.
3. Grundy SM, Vega GL. Hypertriglyceridemia:
causes and relation to coronary
heart
disease.
Semin
Thromb
Hemostas
1988;14:149-64.
Brunzell
JD, Albers JJ, Chait A, Grundy
SM, Groszek E,
vIcDonald GB. Plasma lipoproteins
in familial
combined hyperlipidemia and monogenic familial hypertriglyceridemia.
J Lipid Res
1983;24:147-55.
S. Genest J, Sniderman
A, Cianfeone K, et al. Hyperapobetalipoproteinemia.
Plasma
lipoprotein
responses to oral fat load.
Arteriosclerosis
1986;6:297-304.
S. Friedewald
WT, Levy RI, Fredrickson
DS. Estimation
of the
concentration
of low-density
lipoprotein
cholesterol
in plasma,
without
use of the preparative
ultracentrifuge.
Clin Chem
1972;18:449-502.
7. Warnick GR, Knopp RH, Fitzpatrick
V, Branson L. Estimating
[ow-density lipoprotein
cholesterol by the Friedewald
equation is
adequate for classifying
patients on the basis of nationally
recommended cutpoints. Clin Chem 1990;36:15-9.
S. McNamara
JR, Cohn JS, Wilson PWF, Schaefer EJ. Calculated
values for low-density
lipoprotein
cholesterol in the assessment
of
lipid
abnormalities
and coronary
disease
risk. Clin Chem
990;36:36-42.
McNamara
JR. Campos H, Ordovas JM, Peterson J, Wilson
WF, Schaefer EJ. Effect of gender, age, and lipid status on low
ensity
lipoprotein
subfraction
distribution.
Results
from the
ramingham
Offspring Study. Arteriosclerosis
1987;7:483-90.
0. McNamara JR, Millar JS, Bljjlevens E, Schaefer EJ. LDL 4, 5
nd 6 may be the most atherogenic
LDL species [Abstract].
Clin
hem 1988;34:1226.
1. Weintraub MS, Eisenberg 5, Breslow JL. Different patterns of
stprandial
lipoprotein
metabolism
in normal,
type ha, type ifi,
nd type IV hyperlipoproteinemic
individuals.
Effects of treatment
.
ith cholestyramine
and gemfibrozil.
J Clin
Invest
1987;79:1110-
2. Cohn JS, McNamara
JR, Cohn SD, Ordovas JM, Schaefer EJ.
ostprandial
plasma lipoprotein
changes in human
subjects of
fferent ages. J Lipid Res 1988;29:469-79.
3. Laurell S, Tibbling G. The use of blood glycerol determination
n the diagnosis of hyperthyroidism.
Clin Chim Acta 1968;21:1272.
4. Elm RJ, Ruddel M, McClean
S. The variability
of the glycerol
oncentration
in
human
serum
[Abstract].
Clin
Chem
983;29:1174.
5. Porte D Jr, Bierman
EL. The effect of heparin
infusion on
lasma triglyceride
in vivo and in vitro with a method for calcu-
lating triglyceride
turnover. J Lab Clin Med 1969;73:631-48.
16. Lenz PH, Cargill DI, Fleischman
Al. Propylene glycol interference in determination
of serum and liver triglycerides.
Clin
Chem 1973;19:1071-4.
17. Sevenm G, Buongiorno
A. Serum triglyceride
levels in uremic
patients
receiving
polyacrylonitrilo
dialysis.
Clin
Biochem
1981;14:72-3.
18. Ng RH, Guilmet
R, Altaffer
M, Statland
BE. Falsely high
results for triglycerides
in patients
receiving
intravenous
nitroglycerin [Tech Brief]. Clin Chem 1986;32:2098-9.
19. Hortin GL, Cole TG, Gibson DW, Kessler G. Decreased stability of triglycerides
and increased
free glycerol
in serum from
heparin-treated
patients. Clin Chem 1988;34:1847-9.
20. Chowdhury
FR, Rodman H, Bleicher
SJ. Glycerol-like
contamination
of commercial
blood sampling tubes. Am J Med Tech
1972;38:25-7.
21. Ryder K, Glick M, Bertram 5, Schechter B. Effect of dry-skin
products
on Ektachem triglyceride
results [Abstract].
Clin Chem
1986;32:1411.
22. Cheung CK, Swaminathan
ide assay [Letter]. Clin Chem
R. Effect of detergent
on triglycer1987;33:202.
DB. Micromethod
for the direct deter-
23. Van Handel E, Zilversmit
mination of serum triglycerides.
J Lab Clin Med 1957;50: 152-7.
24. Kessler G, Lederer H. Fluorimetric
measurements
of triglycerides. In: Skeggs LT Jr, ed. Automation
in analytical
chemistry.
New York: Mediad, 1966:341-4.
25. Carlson LA, WadstrOm
LB. Determination
of glycerides
in
blood serum. Clin Chim Acta 1959;4:197-205.
26. Wieland 0. Glycerol. In: Bergmeyer
HU, ed. Methods of enzymatic analysis, 1st ed. New York: Academic Press, 1965;211-4.
27. Eggstein M, Kreutz FH. Eine neue Bestimmung
der Neutralfette in Blutserum
und Gewebe. I. Mitteilung.
Prinzip,
Durchfuhrung
und
Besprechung
der
Methode.
Klin
Wochenschr
1966;44:262-7.
28. Klotzsch 5, Serrichio M, Furedi R. An automated
colorimetric
method for the specific determination
of serum triglycerides.
In:
Advances
in automated
analysis,
Vol. 1. New York: Mediad,
1973;111.
29. Stavropoulos
WS, Crouch RD. Method
for determination
of
triglycerides
and glycerol. US Patent 4 001 089. The Dow Chemical Company. January
4, 1977.
30. Stavropoulos
WS, Crouch RD. Determination
of triglycerides
and glycerol. US Patent 4 142 938. The Dow Chemical
Company.
March 6, 1979.
31. Stavropoulos
WS, Crouch RD. A new colorimetric
procedure
for the determination
of serum triglycerides
[Abstract].
Clin Chem
1974;20:857.
32. Bucolo G, David H. A completely
enzymatic
determination
of
serum triglycerides [Abstract]. Clin Chem 1971;17:664.
33. Bucolo G, David H. Triglyceride
hydrolysis
and assay. US
Patent 3 703 591. Calbiochem
Corp. November 6, 1970; November
21,
1972.
34. Bucolo G, David H. Quantitative
determination
of serum
triglycerides
by the use of enzymes. Clin Chem 1973;19:476-82.
35. Megraw
RE, Dunn DE, Biggs HG. Manual
and continuousflow colorimetry
of triglycerols
by a fully enzymic
method. Clin
Chem 1979;25:273-8.
36. Bowie L, Gochman N. A new spectrophotometric,
enzymatic
determination
of serum
triglycerides
[Abstract].
Clin Chem
1973;19:656.
Rautela
37.
method
GS, Hall RG Jr, Bekiesz
for rapid
biological fluids
38. Winartasaputra
and automatic
[Abstract].
Clin
H, Mallet
CL, Wermus
GR. A kinetic
measurement
of triglycerides
Chem 1974;20:857.
VN, Kaun SS, Guilbault
in
GO. Fluo-
rometric and colorimetric enzymic
determination
of triglycerides
(triacylglycerols)
in serum. Clin Chem 1980;26:613-7.
39. Terada 0, Uwajima
1, Mihara A, Amsaka K. Glycerol oxidase
and process for the production
thereof and method for the quantitative determination
of glycerol by glycerol oxidase. US Patent
4 202 941. Kyowa Hakko Kogyo Co., Ltd. May 13, 1980.
40. Trinder P. Determination
oxidase with an alternative
1969;6:24-7.
41.
Fossati
metrically
Chem
P, Prencipe
of glucose
oxygen
in blood using glucose
Ann Clin Biochem
acceptor.
L. Serum triglycerides determined
colorithat produces hydrogen peroxide.
Clin
with an enzyme
1982;28:2077-80.
CLINICAL
CHEMISTRY,
Vol. 36, No. 9, 1990
1611
42. Schmidt
FH, von Dahl K. Zur Methode der enzymatischen
Neutralfett-Bestimmung
in biologisehen
Material. Z Klin Chem
Klin Biochem 1968;6:156.-9.
43. Chernick
SS. Determination
of glycerol in acyl glycerols. In:
Colowick SP, Kaplan NO, Lowenstein
JM, eds. Methods in enzymology. Vol. 14: Lipids. New York: Academic Press, 1969:627-30.
44.
Winiarski
RJ, Ladden
PJ, Rumbin
SM.
A single
enzymatic
reagent
for serum triglyceride
determination
on clinical chemistry
analyzers
[Abstract].
Clin Chem 1978;24:1019.
45. Hagen JH, Hagen PB. An enzycnic method for the estimation
of glycerol in blood and its use to determine the effect of noradrenaline on the concentration
of glycerol on blood. Can J Biochem
Physiol 1962;40: 1129-39.
46. Grossman
SH, Mollo E, Ertingshausen
G. Simplified,
totally
enzymatic
method for determination
of serum triglycerides
with a
centrifugal
analyzer.
Clin Chem 1976;22:1310-3.
47. Sugiura M, Oikawa T, Hirano K, et al. A simple colorimetric
method
for determination
of serum
triglycerides
with
lipoprotein
lipase and glycerol dehydrogenase.
Clm Chim Acta 1977;81:12530.
48. Van Oers MM, Scholtis RJH, van de Calseyde JF, Kuypers
AMJ. Assay of triglycerides
using the Perkin-Elmer
C-4 Automatic
Analyzer.
Z Klin Chem Klin Biochem 1971;9:516-9.
49. Mourad
N, Zager R, Neveu P. Semiautomated
enzymatic
method for determining
serum triglycerides
by use of the Beckman
“DSA 560.” Clin Chem 1973;19:116-.8.
50. Bucolo G, Yabut J, Chang TY. Mechanized
enzymatic determination of triglycerides
in serum. Clin Chem 1975;21:420-4.
51. Barbour
triglycerides
HM.
with
Enzymatic
the Abbott
determination
Bichromatic
of cholesterol
Analyzer.
Ann
and
Clin
Biochem 1977;14:22-8.
52. Lehnus G, Smith L. Automated
ment
of total
triglycerides
procedure
for kinetic measure(as glycerol) in serum with the Gilford
system 3500. Chin Chem 1978;24:27-31.
53. Naito HK, Gatautis VJ, Galen RS. The measurement
of serum
triacylglycerol
on the Hitachi 705 chemistry analyzer
[Abstracti.
Clin Chem 1985;31:948.
54. Uwajima T, Akita H, Ito K, Mihara A, Aisaka K, Tirada 0.
Formation and purification
of a new enzyme, glycerol oxidase and
stoichiometry
of the enzyme
reaction.
Agric
Biol
Chem
1980;44:399-406.
55. Gauhl H, Seidel H, Lang G, Roder A, Ziegenhorn
J. Method
and reagent
for the determination
of glycerol. US Patent 4 399
218. Boehringer
Mannheim
GmbH. August 16, 1983.
56. McGowan
MW, Artiss JD, Strandbergh
DR, Zak B. A peroxidase-coupled method for the colorinietric
determination
of serum
triglycerides.
Clin
Chem
1983;29:538-42.
57. Sharma A, Artiss JD, Zak B. A method for the sequential
colorimetric
determination
of serum triglycerides
and cholesterol.
Clin Biochem 1987;20:167-72.
58. Werner M, Gabrielson DG, Eastman J. Ultramicro
determination of serum triglycerides
by bioluminescent
assay. Chin Chem
1981;27:268-71.
59. Ambrose RT, Smith JW. The determination
of triglycerides
in
serum by HPLC [Abstract].
Clin Chem 1981;27:1040.
60. Huany C, Roy AV. Lipase composition
for glycerol ester
determination.
US Patent 4 056 442. Dow Chemical Company.
November 1, 1977.
61. Nix PT, Santoro JM, Stephens JE. Enzymatic
glyceride hydrolysis. US Patent 4 394 445. Worthington
Biochemical
Company. July 19, 1983.
62. Battey Y, Fuhrer J, Persen R, Matteo MR. An improved
enzymatic
assay for the determination
of serum triglycerides
on
the CentrifiChem
Analyzer [Abstract].
Clin Chem 1980;26: 1024.
63. Borgstrom B, Erlanson-Albertson
C, Wieloch T. Pancreatic
colipase: chemistry
and physiology
[Review].
J Lipid Res
1979;20:805-16.
64. Wahlefeld AW. Triglycerides
determination
after enzymatic
hydrolysis.
In: Bergmeyer HU, ed. Methods of enzymatic analysis,
2nd ed. Vol. 4. New York: Academic Press, 1974:1831-5.
65. Wahlefeld AW, Mollering
H, Gruber W, Bernt E, Roeschlau
P.
Determination
of triglycerides.
US Patent 3 862 009. Boehringer
Mannheim
GmbH. January
21, 1975.
66. Biochemical
catalogs
and specifications
of Boehringer
Mannheim Corp., Indianapolis,
IN; Genzyme Corp., Boston, MA; Sigma
1612
CLINICAL
CHEMISTRY,
Vol. 36, No. 9, 1990
Chemical
OH.
Corp., St. Louis, MO; US Biochemical
Corp., Clevelanc
67. Fernely
HN. Mammalian
alkaline
phosphatase.
In: Boyer PE
ed. The enzymes, 3rd ed. New York: Academic Press, 197 1:417-4’
68. MacRae AR, Amesbury
LD, Oommen BP. Positive interfei
ence by LDH in the assay of triglycerides
using Bio-Rad kits. Clii
Biochem 1981;14:22C.
69. Zoppi F. Single-cuvet
sequential
determination
of triglycei
ides and cholesterol. Clin Chem 1985;31:2036-9.
70. Sullivan
DR, Kruijswijk
Z, West CE, Kohlmeier
M, Kata
MB. Determination
of serum triglycerides
by an accurate enzy
matic
method
not affected
by free
glycerol. Chin Cher
1985;31:1227-8.
71. McQueen MJ, Garland IWC, Morgan HG. “Glycerate dehydrc
genase”
activity
in myocardial
infarction
and myocardial
ische
mia. Clin Chem 1972;18:275-9.
72. Danniger
J, Deneke U, Lang G, Michal G, Roeschlau F
Method for the determination of substrates
or enzyme activitie
US Patent 4 168 205. Boehringer
Mannheim
GmbH. Septembe
18, 1979.
73. Perlstein MT, Thibert RJ, Zak B. Bilirubin
and hemoglobii
interferences
in direct colorimetric
cholesterol
reactions
usin
enzyme reagents. Microchem
J 1977;22:403-19.
74. Rutman M, Klotzsch
SG. Effect of free and conjugated
biliru
bin on triglycerides
determination
by various methods as applie
to Technicon RA”-Systems
[Abstract].
Clin Chem 1986;32:1187.
75. Siedel J, Staepels J, Ziegenhorn J. Enzymatic
color reagent fo
the assay of serum and urine creatinine
without interference
b:
even grossly elevated sample bilirubin
levels [Abstract].
Clii
Chem 1988;34:1189-90.
76. Spain MA, Wu AHB. Bilirubin interference with determina
tion of uric acid, cholesterol,
and triglycerides
in commercia
peroxidase-coupled
assays, and the effect of ferrocyanide.
Clii
Chem 1986;32:518-21.
77. Feldbruegge
DH, Koch DD, Calkins DM. Use of bilirubii
oxidase as a means of overcoming
bilirubin
interference
with thi
Hitachi
737 cholesterol
method
[Abstract].
Clin Chem 19&
34:1185.
78. Fleming
JK, Gadsden RH Sr, Kabbani I.Definitive character
ization
of uric acid as an interferent
in peroxidase
indicate
reactions
and a proposed mechanism
of action. Clin Biochen
1988;21:27-32.
79. Sanders GTB, Terraneo G, Dois JLS. Artifactual
increase
ii
plasma lactate dehydrogenase
activity
caused by a surfactan
[Letter].
Clin Chem 1987;33:192.
80. Monte AA, Chiang C. Surfactant
containing
reagent formula
tions for assaying biological specimens and methods for preparin
same. US Patent 3 997 470. Mallinckrodt
Inc. December 14, 1976
81. Batz HG, Draeger B, Wahlefeld AW, Weimann G, Gruber W
Eliminating
turbidity
in serum undergoing
photometric
assay. Ul
Patent 4 184 848. Boehringer
Mannheim
GmbH. January
22
1980.
82. Klose 5, Buschek H, Schlumberger
H. Compositions
an
method for reducing turbidity
in samples. US Patent 4 282 00
Boehringer
Mannheim
GmbH. August 4, 1981.
83. Artiss JD, Strandbergh
DR, Zak B. Elimination
of free gly
erol interference
in a colorimetric
enzymic triglyceride
assay. Cli
Chim Acts 1989;182:109-16.
84. Shephard MDS, Whiting
MJ. Falsely low estimation
of
glycerides in lipemic plasma by the enzymatic triglyceride
meth
with Inodifled Trinder’s chromogen. Clin Chem 1990;36:325-39.
85. Muller-Matthesius
R, Gruber W. Enzyme-kinetic
determi
tion of the concentration
of a substrate.
US Patent 3 977 9
Boehringer
Mannheim
GmbH. August 31, 1976.
86. Nagele U, Wahlefeld
AW, Ziegenhorn
J. Triglycerides.
I
Bergmeyer HU, ed. Methods of enzymatic analysis, 3rd ed. Vol.
Weinheim:
Verlag Chemie, 1985:2-18.
87. ter Welle HF, Baartscheer
T, Fiolet JWT. Influence of
glycerol on enzymatic
evaluation
of triglycerides
[Letter].
C
Chem 1984;30:1102-3.
88. Tsuda M, Miike A, Shimizu
Y, Yokote Y, Tatano T. Com
tion and method for decomposing hydrogen peroxide. US Pate
4 416 982. Kyowa Hakko Kogyo Co. November 16, 1981.
89. Davies SN, Campbell JB, Gochman
N. Potential interferon
with the Technicon SMAC triglyceride
measurement,
as illustra
by metronidazole
[Letter]. Clin Chem 1979;28:1979-80.
90. Later
R, Pegon Y, Contreras
P, Quincy
C. A fluorescent
compound that can cause error in enzymic triglycerides
determination
[Letter]. Clin Chem 1985;31:499-500.
91. McPherson PA, Brown KD, Agarwal RP, Threatte GA, Jacobson RJ. Hydroxyurea
interferes
negatively with triglyceride
measurement by a glycerol oxidase method. Clin Chem 1985;31:1355-7.
92 Glick MR, Ryder KW. Interferographs.
Users guide to interferences in clinical chemistry instruments. Indianapolis:
Science
Enterprises
Inc., 1987.
biological
93. Roy AV. Free glycerol interferences
on the enzymatic determination
of serum triglycerides
[Abstract].
Clin Chem 1979;
25:1073.
94. Ham A, Giegel J. Comparison
of “primary and secondary”
calibration
of triglyceride
procedures
[Abstract].
Clin Chem
1975;21:971.
95. Nagele U, Hagele EO, Sauer G, et al. Reagent for the enzymatic determination
of serum total triglycerides
with improved
lipolytic efficiency. J Clin Chem Clin Biochem 1984;22:165-74.
CLINICAL CHEMISTRY, Vol. 36, No. 9, 1990
1613