Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Endomembrane system wikipedia , lookup
Protein moonlighting wikipedia , lookup
Purinergic signalling wikipedia , lookup
Cytokinesis wikipedia , lookup
Phosphorylation wikipedia , lookup
Biochemical switches in the cell cycle wikipedia , lookup
Signal transduction wikipedia , lookup
Magnesium transporter wikipedia , lookup
Protein phosphorylation wikipedia , lookup
Organ-on-a-chip wikipedia , lookup
List of types of proteins wikipedia , lookup
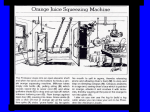
Am J Physiol Renal Physiol 286: F307–F316, 2004. First published October 21, 2003; 10.1152/ajprenal.00275.2003. Protein kinase C-⑀ modulates mitochondrial function and active Na⫹ transport after oxidant injury in renal cells Grażyna Nowak, Diana Bakajsova, and Ginger L. Clifton Department of Pharmaceutical Sciences, College of Pharmacy, University of Arkansas for Medical Sciences, Little Rock, Arkansas 72205 Submitted 1 August 2003; accepted in final form 14 October 2003 a variety of drugs and toxicants results in nephrotoxicity and acute renal failure (ARF). In contrast to the heart or brain, the kidney has the potential for complete recovery from ARF after toxicant- and ischemiareperfusion-induced injury. After the insult, surviving tubular epithelial cells dedifferentiate, proliferate, and eventually replace the irreversibly injured tubular epithelial cells, thus restoring tubular integrity and renal functions (28, 40). A disruption of these processes contributes to prolonged renal dysfunction. Renal proximal tubular cells (RPTC) are the primary target of nephrotoxicants within the kidney, and RPTC dysfunction is primarily responsible for the pathophysiological and clinical presentations of ARF. Therefore, the repair of RPTC functions allows for the return of renal functions after ARF. Growth factors have been implicated in renal regeneration through promoting proliferation, differentiation, and the recovery of mitochondrial function and active Na⫹ transport in renal proximal tubules (10, 18, 19, 28, 29, 34, 36, 43). Recent studies demonstrated that some extracellular matrix proteins also play an important role in the promotion of the repair processes in RPTC. Nony and colleagues (27) demonstrated that collagen IV, but not collagen I, fibronectin, or laminin, promotes the recovery of mitochondrial function and Na⫹/K⫹ activity in toxicant-injured RPTC. However, the exact cellular mechanisms and pathways that mediate the repair of these functions in RPTC remain unknown. Protein kinase C (PKC) consists of a family of 11 phospholipid-dependent serine-threonine kinases classified by the requirement for Ca2⫹ and diacylglycerol for activation (26). PKC is a key mediator of many diverse physiological and pathological processes (11). PKC isozymes play a crucial role in the regulation of major cellular functions, including proliferation, differentiation, motility, ion homeostasis, and transport functions (11). PKC has also been implicated in the regulation of cellular injury, apoptosis, cell survival, and the recovery from injury (11). PKC-⑀ is the diacylglycerol-dependent, Ca2⫹-independent PKC isozyme that plays an important role in cell survival and suppression of apoptosis in some cell types (11, 12). PKC-⑀ is involved in ischemic injury in the heart and is a pivotal signaling element in the cardioprotective mechanisms of ischemic preconditioning (23, 25). Studies in cardiac myocytes have demonstrated that PKC-⑀ activation is required for protection against ischemic injury (8, 9, 14, 16). The inhibition of PKC-⑀ activation and translocation results in the abolition of the protection offered by ischemic preconditioning in the heart (23). Although the exact mechanisms through which PKC-⑀ exerts its protective effects in the heart are not known at present, these effects may be associated with the regulation of ion homeostasis, including modulation of the mitochondrial ATP-dependent K⫹ channel or plasma membrane Na⫹ channels. Furthermore, PKC-⑀ also mediates hydrogen peroxide/ hydroxyl radical-induced opening of mitochondrial ATP-dependent K⫹ channels and an inhibition of mitochondrial GABA receptors in cardiomyocytes (44). Recent studies suggest that PKC-⑀ selectively inhibits the cardiac and neuronal Na⫹ current (11, 42) and plays a role in the modulation of Address for reprint requests and other correspondence: G. Nowak, Univ. of Arkansas for Medical Sciences, Dept. of Pharmaceutical Sciences, 4301 W. Markham St., Little Rock, AR 72205 (E-mail: [email protected]). The costs of publication of this article were defrayed in part by the payment of page charges. The article must therefore be hereby marked “advertisement” in accordance with 18 U.S.C. Section 1734 solely to indicate this fact. renal proximal tubular cells; recovery of physiological functions; respiratory chain; adenosine 5⬘-triphosphate production; sodium-potassium adenosinetriphosphatase EXPOSURE OF THE KIDNEY TO http://www.ajprenal.org 0363-6127/04 $5.00 Copyright © 2004 the American Physiological Society F307 Downloaded from http://ajprenal.physiology.org/ by 10.220.32.246 on June 17, 2017 Nowak, Grażyna, Diana Bakajsova, and Ginger L. Clifton. Protein kinase C-⑀ modulates mitochondrial function and active Na⫹ transport after oxidant injury in renal cells. Am J Physiol Renal Physiol 286: F307–F316, 2004. First published October 21, 2003; 10.1152/ajprenal.00275.2003.—The aim of this study was to determine whether protein kinase C-⑀ (PKC-⑀) is involved in the repair of mitochondrial function and/or active Na⫹ transport after oxidant injury in renal proximal tubular cells (RPTC). Sublethal injury was produced in primary cultures of RPTC using tert-butylhydroperoxide (TBHP), and the recovery of functions was examined. PKC-⑀ was activated three- to fivefold after injury. Active PKC-⑀ translocated to the mitochondria. Basal oxygen consumption (QO2), uncoupled QO2, and ATP production decreased 58, 60, and 41%, respectively, at 4 h and recovered by day 4 after injury. At 4 h, complex I-coupled respiration decreased 50% but complex II- and IV-coupled respirations were unchanged. Inhibition of PKC-⑀ translocation using a peptide selective inhibitor, PKC-⑀V1–2, reduced decreases in basal and uncoupled QO2 values and increased complex I-linked respiration in TBHP-injured RPTC at 4 h of recovery. Furthermore, PKC-⑀V1–2 prevented decreases in ATP production in injured RPTC. Na⫹-K⫹ATPase activity and ouabain-sensitive 86Rb⫹ uptake were decreased by 60 and 53%, respectively, at 4 h of recovery. Inhibition of PKC-⑀ activation prevented a decline in Na⫹-K⫹-ATPase activity and reduced decreases in ouabain-sensitive 86Rb⫹ uptake. We conclude that during early repair after oxidant injury in RPTC 1) PKC-⑀ is activated and translocated to mitochondria; 2) PKC-⑀ activation decreases mitochondrial respiration, electron transport rate, and ATP production by reducing complex I-linked respiration; and 3) PKC-⑀ mediates decreases in active Na⫹ transport and Na⫹-K⫹-ATPase activity. These data show that PKC-⑀ activation after oxidant injury in RPTC is involved in the decreases in mitochondrial function and active Na⫹ transport and that inhibition of PKC-⑀ activation promotes the repair of these functions. F308 PKC-⑀ MODULATES MITOCHONDRIAL FUNCTION AND NA⫹ TRANSPORT MATERIALS AND METHODS Materials. Female New Zealand White rabbits (2.0–2.5 kg) were purchased from Myrtle’s Rabbitry (Thompson Station, TN). The cell culture medium (a 50:50 mixture of DMEM and Ham’s F-12 nutrient mix without phenol red, pyruvate, and glucose) was purchased from MediaTech Cellgro (Herndon, VA). Myristoylated PKC-⑀V1–2 inhibitor (N-Myr-Glu-Ala-Val-Ser-Leu-Lys-Pro-Thr) was supplied by Biomol (Plymouth Meeting, PA). Protease inhibitors and the ATP Bioluminescence Assay Kit HS II were obtained from Roche (Mannheim, Germany), and phosphatase inhibitor cocktails were from Sigma (St. Louis, MO). Tris-glycine gels and nitrocellulose membranes were obtained from BioWhittaker Molecular Applications (Rockland, ME) and Bio-Rad (Hercules, CA), respectively. PhosphoPKC-⑀ and PKC-⑀ antibodies were purchased from Upstate BiotechAJP-Renal Physiol • VOL nology (Lake Placid, NY) and BD Transduction Laboratory (San Diego, CA), respectively. Anti-mouse IgG coupled to horseradish peroxidase was supplied by Kirkegaard & Perry Laboratory (Gaithersburg, MD) and Supersignal Chemiluminescent Substrate by Pierce (Rockford, IL). The sources of the other reagents and cell culture hormones have been described previously (30, 33, 35). Isolation and culture of RPTC. Renal proximal tubules were isolated from rabbit kidneys by the iron-oxide perfusion method and cultured in 35-mm culture dishes in improved conditions, as previously described (35). The culture medium was a 50:50 mixture of DMEM and Ham’s F-12 nutrient mix without phenol red, pyruvate, and glucose, supplemented with 15 mM NaHCO3, 15 mM HEPES, and 6 mM lactate (pH 7.4, 295 mosmol/kgH2O). Human transferrin (5 g/ml), selenium (5 ng/ml), hydrocortisone (50 nM), bovine insulin (10 nM), and L-ascorbic acid-2-phosphate (50 M) were added to the media immediately before daily media change (2 ml/dish). TBHP treatment of the RPTC monolayer. RPTC monolayers reached confluence within 6 days and were treated with TBHP (300 M, 45 min) on day 7 of culture. After TBHP exposure, the monolayer was washed with fresh, warm (37°C) medium and cultured for an additional 4 days. Previously, we have shown that TBHP treatment for this period of time induces ⬃24% cell death and loss from the monolayer and sublethal injury to the remaining cells (32). In experiments using the selective inhibitor of PKC-⑀ translocation (PKC⑀V1– 2), RPTC were treated with 20 M myristoylated PKC⑀V1–2 (NMyr-Glu-Ala-Val-Ser-Leu-Lys-Pro-Thr) for 1 h followed by TBHP treatment. Next, PKC⑀V1–2 was added daily starting with the media change immediately after TBHP exposure. RPTC samples were taken at various time points after TBHP exposure for measurements of mitochondrial functions, active Na⫹ transport, biochemical analyses, and immunoblotting. Oxygen consumption. RPTC monolayers were gently detached from the dishes using a rubber policeman and transferred to the oxygen consumption (QO2) measurement chamber. QO2 was measured polarographically using a Clark-type electrode, as described previously (30, 32, 35). Basal QO2 was used as a marker of overall mitochondrial function in RPTC. Uncoupled QO2 was used as a marker of electron transfer rate and was measured in the presence of carbonyl cyanide p-(trifluoro-methoxy)phenylhydrazone (2 M). Respiration with electron donors linked to the respiratory complex I, II, or IV was measured after aspirating culture media and adding 2 ml warm (37°C) sterile PBS containing 5 mM glutamate ⫹ 5 mM malate (complex I), 10 mM succinate (complex II) ⫹ 0.1 M rotenone, or 1 mM ascorbate ⫹ 1 mM N,N,N⬘,N⬘-tetramethyl-p-phenylenediamine (complex IV). Intracellular ATP content. Intracellular ATP content in RPTC was measured by the luciferase method in freshly prepared cellular lysates using an ATP Bioluminescence Assay Kit HS II (Roche) and following the manufacturer’s protocol. ATP production rate. The assessment of state 3 respiration (the maximum rate of ATP synthesis) was carried out by a modified method of Borkan et al. (4). In brief, the culture media were aspirated and replaced with 1 ml of a buffer solution resembling an intracellular electrolyte milieu (in mM: 120 KCl, 5 KH2PO4, 10 HEPES, 1 MgSO4, and 2 EGTA, adjusted to pH 7.4 with KOH) containing digitonin (0.1 mg/ml) and 5 mM glutamate ⫹ 5 mM malate or 10 mM succinate as the substrates. The reaction was initiated by adding excess ADP (2 mM final concentration) and was carried out for 5 min at 37°C. Initial experiments determined that ATP production in these conditions was linear for 10 min. The reaction was terminated by adding an aliquot of ice-cold perchloric acid (3% final concentration), and the suspension was snap-frozen in liquid nitrogen. After being thawed, the suspension was spun down at 15,000 g for 1 min at 4°C. The supernatant was neutralized to pH 7.5 and centrifuged again at 15,000 g for 10 min at 4°C. The final supernatant was analyzed for ATP content using the ATP Bioluminescence Assay Kit HS II, as described above. The initial pellet was assayed for protein content 286 • FEBRUARY 2004 • www.ajprenal.org Downloaded from http://ajprenal.physiology.org/ by 10.220.32.246 on June 17, 2017 Ca2⫹-independent outward K⫹ channels on the plasma membrane (38). Subcellular redistribution is an essential feature of PKC-⑀ activation. Translocation to specific subcellular compartments is a critical step in the phosphorylation of target proteins and PKC-⑀ signaling. The mitochondrion is thought to be an important target for PKC-⑀ during cardiac ischemia-reperfusion injury. Ischemic preconditioning or phorbol ester induces the translocation of PKC-⑀ to the mitochondria followed by opening of the mitochondrial ATP-sensitive K⫹ channel (37, 45). Active PKC-⑀ also inhibits cytochrome c release from mitochondria, the subsequent activation of caspases, and suppresses apoptosis (12). In cardiac mitochondria, PKC-⑀ forms signaling modules with extracellular signal-regulated kinases (ERKs) and, upon activation, phosphorylates mitochondrial ERKs, which results in the phosphorylation and inactivation of the pro-apoptotic protein Bad (12). Thus the activation of PKC-⑀ in mitochondria is associated with suppression of cell death and enhanced cell survival. Although the evidence supports an important role of PKC-⑀ in the protection against cardiac injury, very little is known about PKC-⑀ involvement in the physiological and pathological processes in the kidney. It is unknown whether toxicantinduced injury has any effect on renal PKC-⑀ and whether renal PKC-⑀, and also the cardiac PKC-⑀, plays a protective role during injury. It has been proposed that oxidative stress accompanying diabetes activates PKC-⑀ in the renal cortical tubules (17). However, the role of PKC-⑀ in the renal dysfunction and repair after oxidant injury is completely unknown. Previously, we have shown that tert-butylhydroperoxide (TBHP) treatment induces ⬃24% cell death and loss from the monolayer and sublethal injury to the remaining cells (32). The sublethal injury induced by TBHP was associated with the decrease in mitochondrial function and the consumption of an oxidative substrate, intracellular ATP content, active Na⫹ transport, and Na⫹-dependent glucose uptake (32). These RPTC functions are repaired over time without addition of any exogenous factors. Our recent studies have shown that the repair of RPTC functions, such as mitochondrial function and active Na⫹ transport, after an oxidant-induced injury is mediated through PKC-dependent mechanisms (31). PKC-⑀ is one of the major PKC isozymes present in RPTC. Therefore, the aim of the present study was to examine whether 1) PKC-⑀ plays a role in mitochondrial dysfunction and decreases in active Na⫹ transport and/or 2) PKC-⑀ mediates the repair of mitochondrial function and active Na⫹ transport after oxidant injury in RPTC. PKC-⑀ MODULATES MITOCHONDRIAL FUNCTION AND NA⫹ TRANSPORT AJP-Renal Physiol • VOL (fatty acid free)] using a Dounce homogenizer and centrifuged at 1,000 g for 5 min at 4°C. The supernatant was collected and centrifuged at 15,000 g for 15 min at 4°C. The pellet containing RPTC mitochondria was washed two times in the washing buffer (395 mM sucrose, 10 mM HEPES, and 0.1 mM EGTA, adjusted to pH 7.4 with KOH) and spun down again at 15,000 g for 15 min at 4°C. The final mitochondrial pellet was resuspended in the Laemmli (21) sample buffer and used for immunoblot analysis. Immunoblotting. Immunoblot analysis was used to determine the total and phosphorylated forms of PKC-⑀ in RPTC homogenates and mitochondria. RPTC homogenates were lysed in the modified radioimmune precipitation assay buffer (50 mM Tris䡠HCl, 150 mM NaCl, 1 mM EGTA, 1% Triton X-100, 1 mM Na3VO4, 1 mM NaF, and the protease and phosphatase inhibitor cocktails; pH 7.4), incubated on ice for 10 min, and spun down at 100,000 g for 15 min at 4°C to pellet the detergent-insoluble fraction; the supernatant was combined with Laemmli sample buffer (21) and boiled as described previously (30). Proteins were separated by SDS-PAGE and transferred electrophoretically to a nitrocellulose membrane. Blots were blocked for 1 h in Tris-buffered saline buffer containing 0.5% casein and 0.1% Tween 20 (blocking buffer) and incubated overnight at 4°C in the presence of anti-phospho-PKC-⑀ or anti-PKC-⑀ antibodies diluted in the blocking buffer. After being washed, the membranes were incubated with secondary IgGs coupled to horseradish peroxidase and washed again. The supersignal chemiluminescent system was used for protein detection. Quantification of the results was performed using scanning densitometry. Protein assay. Protein concentration was determined using the bicinchoninic acid assay with BSA as the standard. Statistical analysis. Data are presented as means ⫾ SE and were analyzed for significance by ANOVA. Multiple means were compared using Fisher’s protected least-significant difference test with a level of significance of P ⬍ 0.05. RPTC isolated from an individual rabbit represented one experiment (n ⫽ 1) consisting of data obtained from 2 to 10 culture plates. RESULTS Activation of PKC-⑀ during RPTC repair after TBHP-induced injury. As shown in Fig. 1, the recovery of RPTC after TBHP-induced injury was associated with the activation of PKC-⑀. The protein levels of phosphorylated (active) PKC-⑀ increased at 1 h of the repair period and remained increased during the 1st day of the recovery (Fig. 1A). The ratio of phosphorylated PKC-⑀ to total PKC-⑀ protein in RPTC homogenates increased 2.5-, 4-, and 3-fold at 1, 2, and 4 h, respectively, after TBHP-induced injury (Fig. 1B). The ratio of phosphorylated PKC-⑀ to total PKC-⑀ remained elevated until 24 h after TBHP injury. Phosphorylation of PKC-⑀ was associated with the translocation from the cytosol to the particulate fraction of RPTC, which confirmed PKC-⑀ activation (Fig 1C). The treatment of RPTC with the PKC-⑀ translocation inhibitor (20 M myristoylated PKC-⑀V1–2) prevented PKC-⑀ translocation to the membranous fraction of TBHP-injured RPTC, which suggested that PKC-⑀V1–2 decreases PKC-⑀ activation (Fig. 1D). Mitochondrial PKC-⑀ during RPTC repair after TBHPinduced injury. Our previous report demonstrated that PKC-␣ is present in RPTC mitochondria (30). This is the first report demonstrating the presence of PKC-⑀ in RPTC mitochondria. The levels of PKC-⑀ and phosphorylated PKC-⑀ in RPTC mitochondria decreased at 1 h after TBHP exposure but increased fourfold and sixfold at 4 and 6 h of the recovery period, respectively (Fig. 2). On days 1, 2, and 4 after injury, the levels of phosphorylated PKC-⑀ were similar in recovering RPTC and 286 • FEBRUARY 2004 • www.ajprenal.org Downloaded from http://ajprenal.physiology.org/ by 10.220.32.246 on June 17, 2017 after solubilization in a buffer containing 100 mM Tris䡠HCl (pH 7.5), 150 mM NaCl, and 0.05% Triton X-100. Mitochondrial membrane potential. Mitochondrial membrane potential (⌬⌿m) was assessed as described previously (30) using JC-1, a cationic dye that exhibits potential-dependent accumulation and formation of red fluorescent J-aggregates in mitochondria, which is indicated by a fluorescence emission shift from green (525 nm) to red (590 nm). At different time points of the recovery period, RPTC monolayers were loaded with 10 M JC-1 for 30 min at 37°C. After being loaded, media were aspirated, and the monolayers were put on ice, washed with ice-cold PBS, scraped off culture dishes, washed again, and resuspended in PBS. Fluorescence was determined by flow cytometry (FACSCalibur; BD Biosciences) using excitation by a 488-nm argon-ion laser. The JC-1 monomer (green) and the Jaggregates (red) were detected separately in FL1 (emission, 525 nm) and FL2 (emission, 590 nm) channels, respectively. ⌬⌿m is presented as the red-to-green fluorescence intensity ratio. Rb⫹ uptake. Ouabain-dependent 86Rb⫹ uptake was used as a cognate for measurement of ouabain-dependent K⫹ transport in RPTC. Monolayers were incubated for 10 min at 37°C in the presence of 10 mM HEPES, 140 mM NaCl, 5 mM KCl, 1 mM MgCl2, 2 mM CaCl2, and 10 M bumetamide (pH 7.4) and in the absence or presence of 1 mM ouabain. This preincubation period allowed the restoration of transmembrane ion gradients as well as bumetamide and ouabain binding. Under these conditions, intracellular Na⫹ concentration is rate limiting for Na⫹-K⫹-ATPase-mediated Rb⫹ uptake. The reaction was initiated by adding 86RbCl (1 Ci; sp act 5.1 mCi/mg) and was carried out for 5 min. In the initial set of experiments, we determined that this reaction time was within the linear 86 Rb⫹ uptake range (data not shown). The uptake was terminated by aspiration of the incubation buffer followed by extensive washing of the monolayers with the ice-cold incubation buffer in which 5 mM KCl was replaced by 5 mM RbCl. The cells were solubilized, and the amount of 86RbCl associated with the monolayers was determined by liquid scintillation spectrometry. Active Rb⫹ uptake was calculated as the difference between total and ouabain-insensitive Rb⫹ uptake. Na⫹-K⫹-ATPase activity. RPTC were scraped from the dishes, resuspended in 5 mM HEPES buffer (pH 7.4), and lysed in 25 mM imidazole buffer (pH 7.0) containing 0.065% SDS, 1% BSA, and phosphatase inhibitor cocktail. After incubation for 10 min at room temperature, 0.6 ml of 0.3% BSA in 25 mM imidazole buffer was added to lower the SDS concentration, and aliquots were used for measurement of Na⫹-K⫹-ATPase activity. Na⫹-K⫹-ATPase activity was determined by measuring the difference between total ATPase activity and ouabain-insensitive ATPase activity, as described previously (33). Isolation of cytosolic and particulate fractions. RPTC samples were harvested at various time points during recovery after TBHP injury. Monolayers were washed with ice-cold PBS to remove all nonviable cells, and the remaining cells were scraped from the dishes, suspended in PBS, pelleted by centrifugation for 15 s in a microfuge, and resuspended in ice-cold isolation buffer (20 mM Tris䡠HCl, pH 7.5, containing 10 mM MgCl2, 2 mM EGTA, 2 mM EDTA, 1 mM NaF, 1 mM Na3VO4, 2 mM dithiothreitol, protease inhibitor cocktail, and phosphatase inhibitor cocktail). After centrifugation at 1,000 g for 5 min to remove cell debris and nuclei, the supernatant was spun down at 100,000 g for 30 min at 4°C. The supernatant resulting from the ultracentrifugation represented the cytosolic fraction. The pellet was resuspended in the isolation buffer containing 1% Triton X-100 and, after 30 min incubation on ice, was centrifuged at 100,000 g for 30 min. The supernatant resulting from this ultracentrifugation represented the original particulate fraction. The cytosolic and particulate fractions were combined with Laemmli sample buffer (21), boiled, and used for immunoblotting. Isolation of RPTC mitochondria. RPTC were homogenized in the ice-cold isolation buffer [225 mM mannitol, 10 mM HEPES (adjusted to pH 7.4 with KOH), 75 mM sucrose, 0.1 mM EGTA, and 0.1% BSA F309 F310 PKC-⑀ MODULATES MITOCHONDRIAL FUNCTION AND NA⫹ TRANSPORT Fig. 1. A: protein levels of phosphorylated (P) protein kinase C (PKC)-⑀ and total PKC-⑀ in renal proximal tubular cell (RPTC) homogenates during the recovery after tert-butylhydroperoxide (TBHP)-induced injury. B: PKC-⑀ activation (the ratio of phosphorylated PKC-⑀ to total PKC-⑀). C: PKC-⑀ levels in cytosolic and particulate fractions in RPTC during the recovery after TBHP-induced injury. D: PKC-⑀ levels in cytosolic and particulate fractions in RPTC grown in the presence of PKC-⑀ inhibitor, PKC-⑀V1–2, during and after TBHP-induced injury. Blots in A are representative of 4 independent experiments. Results (quantified by densitometry) in B are averages ⫾ SE of 4 independent experiments (RPTC isolations). Blots in C and D are representative of 3 independent experiments. *P ⬍ 0.05, significantly different from 0 h (controls). QO2. Basal QO2 was used as a marker of the overall function of RPTC mitochondria. At 4 h after TBHP exposure, basal QO2 in TBHP-injured RPTC was decreased to 42% of control levels (Fig. 3). The inhibition of PKC-⑀ activation by PKC-⑀V1–2 reduced decreases in basal QO2 to 63% of controls (Fig. 3). Basal QO2 in TBHP-injured RPTC recovered on day 4 after the exposure regardless of the presence or absence of PKC-⑀V1–2 (Fig. 3). Uncoupled QO2 was used as a marker of the mitochondrial electron transfer rate and the integrity of respiratory complexes. Uncoupled QO2 in TBHP-treated RPTC decreased to 39% of control levels at 4 h after the injury (Fig. 4). The inhibition of PKC-⑀ activation by PKC-⑀V1–2 reduced TBHPinduced decreases in uncoupled QO2 to 57% of controls at 4 h of the recovery (Fig. 4). The inhibition of PKC-⑀ had no effect on uncoupled QO2 in TBHP-treated RPTC on day 4 (Fig. 4). in controls (Fig. 2, data not shown). These data demonstrate that active (phosphorylated) PKC-⑀ is translocated to RPTC mitochondria during the early recovery after TBHP-induced injury. Fig. 2. Protein levels of phosphorylated PKC-⑀ and total PKC-⑀ in RPTC mitochondria during the recovery after TBHP-induced injury. Blots are representative of 3 independent experiments (RPTC isolations). AJP-Renal Physiol • VOL Fig. 4. Uncoupled oxygen consumption (a marker for electron transfer rate) during RPTC recovery after TBHP-induced injury. Results are averages ⫾ SE of 8 independent experiments (RPTC isolations). Values with dissimilar superscripts on a given day are significantly different (P ⬍ 0.05) from each other. 286 • FEBRUARY 2004 • www.ajprenal.org Downloaded from http://ajprenal.physiology.org/ by 10.220.32.246 on June 17, 2017 Fig. 3. Basal oxygen consumption (QO2, a marker for overall mitochondrial function) during RPTC recovery after TBHP-induced injury. Results are averages ⫾ SE of 8 independent experiments (RPTC isolations). Values with dissimilar superscripts on a given day are significantly different (P ⬍ 0.05) from each other. PKC-⑀ MODULATES MITOCHONDRIAL FUNCTION AND NA⫹ TRANSPORT Because the data suggested that the components of the respiratory chain are the targets of PKC-⑀, we examined whether respiration coupled to complexes I, II, or IV is under the control of PKC-⑀. Complex I-coupled respiration (measured using glutamate and malate as electron donors) decreased to 52% of controls at 4 h after TBHP-induced injury (Fig. 5A). AJP-Renal Physiol • VOL In contrast, TBHP-induced injury had no effect on complex IIand complex IV-coupled respirations (Fig. 5, B and C). PKC⑀V1–2 had no effect on complex I-coupled respiration in controls but diminished TBHP-induced decreases in site I-coupled respiration to 74% of those in control RPTC (Fig. 5A). Furthermore, PKC-⑀V1–2 stimulated complex II-coupled respiration 1.5-fold in TBHP-injured RPTC, whereas it had no effect in controls (Fig. 5B). Complex IV-linked respiration in TBHP-injured RPTC at 4 h of the recovery period was stimulated 1.4-fold by the inhibition of PKC-⑀ activation but was unaffected in controls (Fig. 5C). These results demonstrate that PKC-⑀ activation plays a role in mitochondrial dysfunction in TBHP-injured RPTC and that the inhibition of PKC-⑀ activation protects against decreases in mitochondrial respiration. Furthermore, these data show that the electron transport chain is a target of PKC-⑀ during oxidant injury and that the inhibition of PKC-⑀ activation in recovering RPTC increases respiration through complexes I, II, and IV of the respiratory chain. ATP production. ATP synthesis is the fundamental function of the mitochondria. The rate of ATP synthesis was measured during state III (the maximal capacity of mitochondria to generate ATP) in digitonin-permeabilized RPTC incubated in the presence of ADP, and metabolic substrates linked to the respiratory complex I (glutamate ⫹ malate) and the respiratory complex II (succinate). The rate of ATP production in the presence of electron donors linked to complex I was 43.9 ⫾ 4.1 nmol䡠mg protein⫺1 䡠min⫺1 in control RPTC. The early recovery period after TBHP exposure was associated with the decrease in complex I-mediated ATP production to 59% of the control levels (Fig. 6A). This decrease was prevented by the inhibition of PKC-⑀ activation in TBHP-injured RPTC (Fig. 6A). Complex I-linked ATP synthesis in TBHP-injured RPTC recovered on day 4 regardless of the presence or absence of PKC-⑀V1–2. In contrast, ATP synthesis in the presence of complex II-linked substrate (succinate) was not affected by TBHP-induced injury, and PKC-⑀V1–2 had no effect on ATP synthesis supported by succinate (Fig. 6B). These results demonstrate that PKC-⑀ mediates TBHP-induced decreases in ATP production coupled to the oxidation of electron donors to complex I. Intracellular ATP levels. Intracellular ATP contents were examined during RPTC recovery to determine whether the inhibition of PKC-⑀ activation promotes intracellular ATP levels in recovering RPTC after TBHP injury. ATP content in control RPTC was 10.6 ⫾ 1.7 nmol/mg protein, and PKC⑀V1–2 had no effect on ATP levels in control RPTC (Fig. 7). ATP content was diminished by 54% at 4 h of the recovery after TBHP exposure, and the inhibition of PKC-⑀ activation had no effect on the decreases in the intracellular ATP content in TBHP-injured RPTC (Fig. 7). ATP content recovered on day 4 after TBHP injury regardless of the presence or absence of PKC-⑀V1–2 (Fig. 7). ⌬⌿m. Mitochondrial respiration results in the generation of proton and pH gradients across the inner mitochondrial membrane and produces the ⌬⌿m, which represents most of the energy of the proton gradient. ⌬⌿m in RPTC was assessed by the measurement of changes in the J-aggregate-to-JC-1 monomer ratio. The J-aggregate-to-JC-1 monomer ratio in control RPTC was 1.15 ⫾ 0.31 and was not altered at 4 h or on day 4 after TBHP-induced injury (Fig. 8). Inhibition of PKC-⑀ acti- 286 • FEBRUARY 2004 • www.ajprenal.org Downloaded from http://ajprenal.physiology.org/ by 10.220.32.246 on June 17, 2017 Fig. 5. Oxygen consumption coupled to complex I (A), complex II (B), and complex IV (C) during RPTC recovery after TBHP-induced injury. Results are averages ⫾ SE of 8 independent experiments (RPTC isolations). Values with dissimilar superscripts on a given day are significantly different (P ⬍ 0.05) from each other. F311 F312 PKC-⑀ MODULATES MITOCHONDRIAL FUNCTION AND NA⫹ TRANSPORT Fig. 6. ATP production rate in the presence of electron donors linked to complex I (A) and complex II (B) during RPTC recovery after TBHP-induced injury. Results are averages ⫾ SE of 5 independent experiments (RPTC isolations). Values with dissimilar superscripts on a given day are significantly different (P ⬍ 0.05) from each other. vation had no effect on ⌬⌿m in control or TBHP-injured RPTC (Fig. 8). These data show that PKC-⑀ does not play any role in the maintenance of the ⌬⌿m in RPTC. Active Na⫹ transport. Active Na⫹ transport was used as a marker of the basolateral membrane function and was assessed by the measurement of ouabain-sensitive Rb⫹ uptake and the activity of Na⫹-K⫹-ATPase. Ouabain-sensitive Rb⫹ uptake in control RPTC was 36.3 ⫾ 4.8 nmol RbCl2䡠mg protein⫺1䡠min⫺1 and was unaffected by PKC-⑀V1–2 (Fig. 9). At 4 h of the recovery period after TBHP-induced injury, ouabain-sensitive Rb⫹ uptake was decreased to 47% of levels in control RPTC (Fig. 9). However, in the presence of PKC-⑀V1–2, ouabain-sensitive Rb⫹ uptake in TBHP-treated RPTC was 67% of control levels (Fig. 9). Ouabainsensitive Rb⫹ uptake returned on day 4 after TBHP exposure regardless of the presence or absence of PKC-⑀V1–2 (Fig. 9). Na⫹-K⫹-ATPase activity was 290 ⫾ 25 mU䡠mg protein⫺1 䡠min⫺1 in controls. TBHP-induced injury was associated with a 60% decrease in the Na⫹-K⫹-ATPase activity at 4 h of the recovery period (Fig. 10). On day 4 of the recovery period, the Na⫹-K⫹-ATPase activity in TBHP-injured RPTC was higher than at 4 h but still 29% lower than in controls (Fig. 10). Inhibition of PKC-⑀ translocation by PKC-⑀V1–2 had no AJP-Renal Physiol • VOL effect on the Na⫹-K⫹-ATPase activity in control RPTC but prevented TBHP-induced decreases in the Na⫹-K⫹-ATPase activity at 4 h after the injury and maintained the pump activity throughout the 4-day recovery period (Fig. 10; data not shown). These data show that inhibition of PKC-⑀ activation in TBHP-treated RPTC protects against the decreases in the activity of Na⫹-K⫹-ATPase and active Na⫹ transport and maintains this function during the recovery period. DISCUSSION PKC isozymes have been implicated in a variety of cellular functions and physiological and pathophysiological responses in different tissues. These responses include proliferation, mi- Fig. 8. Mitochondrial membrane potential in RPTC during the recovery after TBHP-induced injury. Results are expressed as the ratio of the aggregate-tomonomeric form of JC-1. Results are averages ⫾ SE of 5 independent experiments (RPTC isolations). Values with dissimilar superscripts on a given day are significantly different (P ⬍ 0.05) from each other. 286 • FEBRUARY 2004 • www.ajprenal.org Downloaded from http://ajprenal.physiology.org/ by 10.220.32.246 on June 17, 2017 Fig. 7. Intracellular content of ATP in RPTC during the recovery after TBHP-induced injury. Results are averages ⫾ SE of 4 independent experiments (RPTC isolations). Values with dissimilar superscripts on a given day are significantly different (P ⬍ 0.05) from each other. PKC-⑀ MODULATES MITOCHONDRIAL FUNCTION AND NA⫹ TRANSPORT gration, permeability, contraction, secretion, injury, and apoptosis (11). It has been shown that PKC-⑀ plays an important role in ischemic damage in the heart and that PKC-⑀ activation is required for the protection of cardiac tissue from ischemiainduced cell death (16). The involvement of PKC-⑀ in cell survival has been also demonstrated in cancer cells (12). The protective effects of PKC-⑀ in cancer cells are the result of dysregulation of one or more of the mitochondrial apoptotic pathways responsible for caspase activation (12). PKC isozymes have been also implicated in the renal recovery after the ARF (1, 22) and in wound healing after mechanically induced injury in renal tubular epithelial cells (39). The activation of PKC-␦, PKC-⑀, and PKC-, but not PKC-␣ or PKC-, occurs during compensatory renal hypertrophy induced by unilateral nephrectomy (13). Our previous study has shown that PKC plays an important role in the recovery of mitochondrial and transport functions in RPTC after toxicantinduced injury (31). These data suggested that PKC-␣ and/or PKC-⑀ are involved in the repair of RPTC functions after sublethal injury induced by the oxidant, TBHP (31). Our present results demonstrate that PKC-⑀ is activated during the early recovery after oxidant injury as shown by both the increases in phosphorylation and translocation of PKC-⑀ from the cytosolic to the particulate fraction of RPTC. These data are consistent with recent reports showing that PKC-⑀ is activated by oxidative stress induced by hyperglycemia in the diabetic kidney (17). The activation of PKC-⑀ was most pronounced within a few hours after TBHP-induced injury, which suggested that PKC-⑀ plays a role in the early repair process in RPTC. PKC-⑀ activation subsided at 24 h after the injury and was followed by the recovery of RPTC functions on day 4. Elucidating the function of a specific PKC isozyme in the presence of other PKCs requires selective tools to inhibit the isozyme under study. Many current approaches include the use of isozyme nonselective pharmacological inhibitors, preventing a meaningful interpretation of the results. Several years ago, it was demonstrated that a translocation inhibitor peptide (corresponding to the PKC-⑀-binding site for the specific reAJP-Renal Physiol • VOL ceptor for activated C kinase, RACK) acts as a selective competitor of PKC-⑀ translocation, binding, and function (14, 16). This inhibitor peptide (PKC-⑀V1–2) has been used to demonstrate that the activation of PKC-⑀ mediates the protective effects of ischemic preconditioning in cardiac myocytes (16). In the present study, we used PKC-⑀V1–2 to block PKC-⑀ translocation during TBHP exposure and the recovery period and to decrease PKC-⑀ function in regenerating RPTC. The use of PKC-⑀V1–2 allowed us to show that PKC-⑀ mediates the decreases in mitochondrial respiration and ATP production after sublethal injury produced by the oxidant TBHP. Specifically, the inhibition of PKC-⑀ activation with PKC-⑀V1–2 diminished TBHP-induced decreases in basal and uncoupled QO2 values. These data suggested that the respiratory chain is the target for PKC-⑀. To look further into the mechanism of these changes, we tested whether the complexes of the mitochondrial respiratory chain are the target(s) of PKC-⑀. Different oxidative substrates were used as electron donors to differentiate between respiration linked to the generation of NADH and complex I, FADH2 production and complex II, or complex IV. Electrons (reducing equivalents) from glutamate and malate enter the electron transport chain mainly as NADH at complex I. Electrons from succinate enter the electron transport chain as FADH2 at complex II. Electrons from both complexes I and II then feed into the Q cycle portion of complex III. Interestingly, TBHP exposure decreased only respiration linked to respiratory complex I but had no effect on respiration linked to complexes II and IV. Because respiration linked to complex II was not affected during TBHP exposure and RPTC recovery, we conclude that the respiratory complex III was not affected by sublethal injury induced by TBHP. These data also suggest that the availability of ubiquinone, which carries the electrons between complexes I or II and complex III, was adequate to support the electron transport. Therefore, we conclude that sublethal concentrations of TBHP target components of the respiratory complex I or NADHproducing dehydrogenases upstream of complex I but have no apparent effects on complex II and FADH2 production. The Fig. 10. Na⫹-K⫹-ATPase activity in RPTC lysates during the recovery after TBHP-induced injury. Results are averages ⫾ SE of 4 independent experiments (RPTC isolations). Values with dissimilar superscripts on a given day are significantly different (P ⬍ 0.05) from each other. 286 • FEBRUARY 2004 • www.ajprenal.org Downloaded from http://ajprenal.physiology.org/ by 10.220.32.246 on June 17, 2017 Fig. 9. Ouabain-sensitive 86Rb⫹ uptake (a marker of active Na⫹ transport) in RPTC during the recovery after TBHP-induced injury. Results are averages ⫾ SE of 4 independent experiments (RPTC isolations). Values with dissimilar superscripts on a given day are significantly different (P ⬍ 0.05) from each other. F313 F314 PKC-⑀ MODULATES MITOCHONDRIAL FUNCTION AND NA⫹ TRANSPORT AJP-Renal Physiol • VOL Na⫹-K⫹-ATPase activity can be primarily controlled by PKC through phosphorylation of the catalytic ␣-subunit of the pump on serine and threonine residues (20, 24). In contrast to other cell types, Na⫹-K⫹-ATPase activity in renal proximal tubules is inhibited through phosphorylation by PKC (3, 20). Furthermore, the levels of intracellular Na⫹ modulate the effects of PKC-mediated phosphorylation on Na⫹-K⫹-ATPase activity. Increased intracellular Na⫹ concentrations are associated with the inhibition of Na⫹-K⫹-ATPase activity in response to phosphorylation (15). We assessed the function of Na⫹-K⫹-ATPase in the cell by measuring the ouabain-sensitive 86Rb⫹ uptake and showed that pump function is decreased early after TBHP exposure and recovers on day 4 of the repair. Inhibition of PKC-⑀ activation by PKC⑀V1–2 in TBHP-injured RPTC significantly reduced the decreases in ouabain-sensitive 86Rb⫹ uptake during the early recovery period. This suggested that the decrease in active Na⫹ transport in RPTC after TBHP injury is dependent on PKC-⑀ activation and that PKC-⑀ activation decreases Na⫹-K⫹-ATPase function. The decrease in the pump function of Na⫹-K⫹-ATPase could be the result of the decrease of Na⫹-K⫹-ATPase catalytic activity or the reduced number of pump molecules on the basolateral membrane. Our study determined that the catalytic activity of Na⫹-K⫹-ATPase in cell lysates is decreased in TBHP-injured RPTC but is maintained by treatment with PKC⑀V1–2. These results suggest that the phosphorylation of Na⫹-K⫹-ATPase by PKC-⑀ decreases the pump activity and show that the inhibition of PKC-⑀ activation during the early repair process maintains the catalytic activity of Na⫹-K⫹-ATPase. Therefore, our results suggest that Na⫹-K⫹-ATPase is an effector protein for PKC-⑀ in TBHP-injured RPTC. Our data are in agreement with the study by Buhagiar et al. (7), who demonstrated that PKC-⑀ regulates the sarcolemmal Na⫹-K⫹ pump in cardiac myocytes. However, it is unknown, yet, whether PKC-⑀ phosphorylates Na⫹K⫹-ATPase directly or through activation of a downstream kinase. Thus our data show that oxidant-induced injury activates PKC-⑀ in RPTC and that this activation mediates decreases in mitochondrial function, specifically in complex I-mediated respiration, active Na⫹ transport, and Na⫹-K⫹-ATPase activity. Therefore, the activation of PKC-⑀ in renal cells appears to play a role distinct from the protective effects in the cardiac tissue. In the heart, the activation of PKC-⑀ has been shown to protect against injury, and it is thought that this protection is through mitochondrial and/or transport mechanisms (2, 8, 9, 14, 37, 38, 42–45). In contrast, oxidant-induced activation of PKC-⑀ in renal cells is detrimental to the respiratory and transport functions, and the inhibition of PKC-⑀ activation offers protection against the decrease in these functions. We speculate that this apparent difference between cardiac and renal responses to activation of PKC-⑀ may be the result of different downstream targets of PKC-⑀ in cardiomyocytes and RPTC, and phosphorylation of different mitochondrial enzymes that regulate oxidative metabolism or other proteins essential for mitochondrial function. Furthermore, the effects of PKC-⑀-mediated regulation of Na⫹-K⫹-ATPase, ion channels, and/or transporter proteins may be different in cardiomyocytes and RPTC, thus affecting ion homeostasis and cell survival. 286 • FEBRUARY 2004 • www.ajprenal.org Downloaded from http://ajprenal.physiology.org/ by 10.220.32.246 on June 17, 2017 lack of effects of TBHP on the ⌬⌿m at 4 h after the exposure suggests that the integrity of the inner mitochondrial membrane was not compromised and that mitochondrial NADH was not lost because of leakage from the mitochondria. Inhibition of PKC-⑀ activation with PKC⑀V1–2 reduced decreases in the respiration linked to complex I at 4 h of the recovery of TBHP-injured RPTC. This protective effect could be the result of preserving the activities of NADH-producing dehydrogenases in the tricarboxylic acid cycle or maintaining the activity of complex I. The choice of respiratory substrates used in this study precluded the involvement of dehydrogenases upstream of the tricarboxylic acid cycle. At the present time, it is not clear whether complex I or the dehydrogenases of the tricarboxylic acid cycle are the targets for PKC-⑀. It has been shown, however, that the activities of aconitase and the ␣-ketoglutarate dehydrogenase complex are decreased by oxidative stress induced by H2O2 (41). The ␣-ketoglutarate dehydrogenase complex has been the most extensively studied component of the tricarboxylic acid cycle, since it is a key regulatory component of oxidative metabolism. It has been shown that the ␣-ketoglutarate dehydrogenase complex is sensitive to some nephrotoxicants and heavy metals, including zinc (5, 6, 41). Therefore, we speculate that, as a key regulatory enzymatic complex of the oxidative metabolism, the ␣-ketoglutarate dehydrogenase is a very likely target of TBHP and PKC-⑀ in our model. However, because the inhibition of PKC-⑀ activation restored the respiration only partially, we conclude that mechanisms other than PKC-⑀ contribute to the decreases in complex I-linked respiration. Alternatively, the TBHP-induced decline in complex I respiration is the result of the decrease in activities of multiple enzymes of the tricarboxylic acid cycle and complex I, but PKC-⑀ targets only one of them. The decrease in QO2 in TBHP-injured RPTC was accompanied by a decline in glutamate- and malate-linked ATP production, whereas succinate-coupled ATP production remained unaffected throughout the repair period. These results further support the conclusion that the flow of electrons through complex I but not complex II, III, or IV is decreased during the early recovery of TBHP-injured RPTC. Furthermore, consistent with the promotion of respiration, blocking PKC-⑀ activation restored the glutamate- and malate-supported ATP production rate at 4 h of the recovery. Thus our results suggest that the respiratory function and ATP synthesis in TBHP-injured RPTC are, in part, under the control of PKC-⑀. However, despite the increased ATP production rate at 4 h of the recovery, the intracellular ATP content in TBHP-injured RPTC was not restored in the presence of a PKC-⑀ inhibitor, which suggested an increase in the ATP-consuming processes. Active ion transport consumes a large portion of energy (ATP) generated by renal proximal tubules. The proximal tubule is the principal site of renal Na⫹ reabsorption, which involves Na⫹-K⫹-ATPase, the ion pump using metabolic energy derived from ATP hydrolysis and generating the electrochemical gradient of Na⫹ and K⫹ across the plasma membrane. Na⫹-K⫹-ATPase is the main determinant of low cytosolic levels of Na⫹ and therefore plays a central role in the regulation of cell volume, intracellular electrolyte content, secondary active transmembrane transport of other ions, and cellular uptake of organic compounds cotransported with sodium. It has been shown that, in proximal convoluted tubules, PKC-⑀ MODULATES MITOCHONDRIAL FUNCTION AND NA⫹ TRANSPORT In conclusion, PKC-⑀ plays a role in the early phase of the recovery of mitochondrial function and active Na⫹ transport after oxidant injury in RPTC. PKC-⑀ activation decreases mitochondrial respiration, electron transport rate, and ATP production by decreasing the electron flow through complex I. The data also suggest that Na⫹-K⫹-ATPase is an effector protein for active PKC-⑀, thereby establishing a molecular link between oxidant injury and the decrease in active Na⫹ transport in RPTC. Thus the inhibition of PKC-⑀ activation early after oxidant injury in renal proximal tubules represents a means to promote the repair of mitochondrial function and active Na⫹ transport. ACKNOWLEDGMENTS 15. 16. 17. 18. 19. 20. GRANTS This work was supported by National Institute of Diabetes and Digestive and Kidney Diseases Grant R01DK-59558. 21. 22. REFERENCES 1. Alberti P, Bardella L, and Comolli R. Ribosomal protein S6 kinase and protein kinase C activation by epidermal growth factor after temporary renal ischemia. Nephron 64: 296–302, 1993. 2. Baines CP, Zhang J, Wang G, Zheng Y, Xiu JX, Cardwell EM, Bolli R, and Ping P. Mitochondrial PKC⑀ and MAPK form signaling modules in the murine heart: enhanced mitochondrial PKC⑀-MAPK interactions and differential MAPK activation in PKC⑀-induced cardioprotection. Circ Res 90: 390–397, 2002. 3. Bertorello A and Aperia A. Na⫹-K⫹-ATPase is an effector protein for protein kinase C in renal proximal tubule cells. Am J Physiol Renal Fluid Electrolyte Physiol 256: F370–F373, 1989. 4. Borkan SC, Emami A, and Schwartz JH. Heat stress protein-associated cytoprotection of inner medullary collecting duct cells from rat kidney. Am J Physiol Renal Fluid Electrolyte Physiol 265: F333–F341, 1993. 5. Brown AM, Bruce SK, Effron MS, Shestopalov AI, Ullucci PA, Sheu KFR, Blass JP, and Cooper AJL. Zn2⫹ inhibits ␣-ketoglutarate-stimulated mitochondrial respiration and the isolated ␣-ketoglutarate dehydrogenase complex. J Biol Chem 275: 13441–13447, 2000. 6. Bruschi SA, Lindsay JG, and Crabb JW. Mitochondrial stress protein recognition of inactivated dehydrogenases during mammalian cell death. Proc Natl Acad Sci USA 95: 13413–13418, 1998. 7. Buhagiar KA, Hansen PS, Bewick NL, and Rasmussen HH. Protein kinase C⑀ contributes to regulation of the sarcolemmal Na⫹-K⫹ pump. Am J Physiol Cell Physiol 282: C1059–C1063, 2002. 8. Chen C, Gray MO, and Mochly-Rosen D. Cardioprotection from ischemia by a brief exposure to physiological levels of ethanol: role of epsilon and protein kinase C. Proc Natl Acad Sci USA 96: 12784–12789, 1999. 9. Chen L, Hahn H, Wu G, Chen C, Liron T, Schechtman D, Cavallaro G, Banci L, Guo Y, Bolli R, Dorn GW II, and Mochly-Rosen D. Opposing cardioprotective actions and parallel hypertrophic effects of ␦PKC and ⑀PKC. Proc Natl Acad Sci USA 98: 11114–11119, 2001. 10. Counts RS, Nowak G, Wyatt RD, and Schnellman RG. Nephrotoxin inhibition of renal proximal tubule cell regeneration. Am J Physiol Renal Fluid Electrolyte Physiol 269: F274–F281, 1995. 11. Dempsey EC, Newton, AC, Mochly-Rosen D, Fields AP, Reyland ME, Insel PA, and Messing RO. Protein kinase C isozymes and the regulation of diverse cell responses. Am J Physiol Lung Cell Mol Physiol 279: L429–L438, 2000. 12. Ding L, Wang H, Lang W, and Xiao L. Protein kinase C-⑀ promotes survival of lung cancer cells by suppressing apoptosis through dysregulation of the mitochondrial caspase pathway. J Biol Chem 277: 35305– 35313, 2002. 13. Dong L, Stevens JL, Fabbro D, and Jaken S. Regulation of protein kinase C isozymes in kidney regeneration. Cancer Res 53: 542–4549, 1993. 14. Dorn GW II, Souroujon MC, Liron T, Chen C, Gray MO, Zhou HZ, Csukai M, Wu G, Lorenz JN, and Mochly-Rosen D. Sustained in vivo AJP-Renal Physiol • VOL 23. 24. 25. 26. 27. 28. 29. 30. 31. 32. 33. 34. 35. 36. 37. cardiac protection by a rationally designed peptide that causes ⑀ protein kinase C translocation. Proc Natl Acad Sci USA 96: 12798–12803, 1999. Efendiev R, Bertorello AM, Zandomeni R, Cinelli AR, and Pedemonte CH. Agonist-dependent regulation of renal Na⫹, K⫹-ATPase activity is modulated by intracellular sodium concentration. J Biol Chem 277: 11489–11496, 2002. Gray MO, Karliner JS, and Mochly-Rosen D. A selective ⑀-protein kinase C antagonist inhibits protection of cardiac myocytes from hypoxiainduced cell death. J Biol Chem 272: 30945–30951, 1997. Ha H, Yu MR, Choi YJ, and Lee HB. Activation of protein kinase c-␦ and c-⑀ by oxidative stress in early diabetic rat kidney. Am J Kidney Dis 38: S204–S207, 2001. Humes HD, Cieslinski DA, Coimbra TM, Messana JM, and Galvao C. Epidermal growth factor enhances renal tubule cell regeneration and repair and accelerates the recovery of renal function in postischemic acute renal failure. J Clin Invest 84: 1757–1761, 1989. Kays SE and Schnellmann RG. Regeneration of renal proximal tubule cells in primary culture following toxicant injury: response to growth factors. Toxicol Appl Pharmacol 132: 273–280, 1995. Kazanietz MG, Caloca MJ, Aizman O, and Nowicki S. Phosphorylation of the catalytic subunit of rat renal Na⫹,K⫹-ATPase by classical PKC isoforms. Arch Biochem Biophys 338: 74–80, 2001. Laemmli UK. Cleavage of structural proteins during the assembly of the head bacteriophage T4. Nature 227: 680–685, 1970. La Porta CA and Comolli R. Biochemical and immunological characterization of calcium-dependent and -independent PKC isoenzymes in renal ischemia. Biochem Biophys Res Commun 191: 1124–1130, 1993. Mackay K and Mochly-Rosen D. Localization, anchoring, and functions of protein kinase C isozymes in the heart. J Mol Cell Cardiol 33: 1301–1307, 2001. Mahmmoud YA and Cornelius F. Protein kinase C phosphorylation of purified Na,K-ATPase: C-terminal phosphorylation sites at the ␣- and ␥-subunits close to the inner face of the plasma membrane. Biophys J 82: 1907–1909, 2002. Naruse K and King GL. Protein kinase C and myocardial biology and function. Circ Res 86: 1104–1106, 2000. Nishizuka, Y. Intracellular signaling by hydrolysis of phospholipids and activation of protein kinase C. Science 258: 607–614, 1992. Nony PA, Nowak G, and Schnellmann RG. Collagen IV promotes repair of renal cell physiological functions after toxicant injury. Am J Physiol Renal Physiol 281: F443–F453, 2001. Nony PA and Schnellmann RG. Mechanisms of renal cell repair and regeneration after acute renal failure. J Pharmacol Exp Ther 304: 905– 912, 2003. Norman J, Tsau K, Backay A, and Fine LG. Epidermal growth factor accelerates functional recovery from ischaemic acute tubular necrosis in the rat: role of the epidermal growth factor receptor. Clin Sci (Colch) 78: 445–450, 1990. Nowak G. Protein kinase C-␣ and ERK1/2 mediate mitochondrial dysfunction, decreases in active Na⫹ transport, and cisplatin-induced apotosis in renal cells. J Biol Chem 277: 43377–43388, 2002. Nowak G. Protein kinase C mediates repair of mitochondrial and transport functions following toxicant-induced injury in renal cells. J Pharmacol Exp Ther 306: 157–165, 2003. Nowak G and Schnellmann RG. L-Ascorbic acid regulates growth and metabolism of renal cells: improvements in cell culture. Am J Physiol Cell Physiol 271: C2072–C2080, 1996. Nowak G and Schnellmann RG. Renal cell regeneration following oxidant exposure: inhibition by TGF-1 and stimulation by ascorbic acid. Toxicol Appl Pharmacol 145: 175–183, 1997. Nowak G, Aleo MD, Morgan JA, and Schnellmann RG. Recovery of cellular functions following oxidant injury. Am J Physiol Renal Physiol 274: F509–F515, 1998. Nowak G, Keasler KB, McKeller DE, and Schnellmann RG. Differential effects of EGF on repair of cellular functions after dichlorovinylL-cysteine-induced injury. Am J Physiol Renal Physiol 276: F228–F236, 1999. Nowak G, Carter CA, and Schnellmann RG. Ascorbic acid promotes recovery of cellular functions following toxicant-induced injury. Toxicol Appl Pharmacol 167: 37–45, 2000. Ohnuma Y, Miura T, Miki T, Tanno M, Kuno A, Tsuchida A, and Shimamoto K. Opening of mitochondrial KATP channel occurs downstream of PKC-⑀ activation in the mechanism of preconditioning. Am J Physiol Heart Circ Physiol 283: H440–H447, 2002. 286 • FEBRUARY 2004 • www.ajprenal.org Downloaded from http://ajprenal.physiology.org/ by 10.220.32.246 on June 17, 2017 We thank Malinda L. Godwin for assistance in the isolation and primary culture of RPTC. F315 F316 PKC-⑀ MODULATES MITOCHONDRIAL FUNCTION AND NA⫹ TRANSPORT 38. Shimoni Y. Protein kinase C regulation of K⫹ currents in rat ventricular myocytes and its modification by hormonal status. J Physiol 520: 439– 449, 1999. 39. Sponsel HT, Breckon R, and Anderson RJ. Adenine nucleotide and protein kinase C regulation of renal tubular epithelial cell wound healing. Kidney Int 48: 85–92, 1995. 40. Toback FG. Regeneration after acute tubular necrosis. Kidney Int 41: 226–246, 1992. 41. Tretter L and Adam-Vizi V. Inhibition of krebs cycle enzymes by hydrogen peroxide: a key role of ␣-ketoglutarate dehydrogenase in limiting NADH production under oxidative stress. J Neurosci 20: 8972–8979, 2000. 42. Xiao G, Qu Y, Sun Z, Mochly-Rosen, and Boutjdir M. Evidence for functional role of ⑀PKC isozyme in the regulation of cardiac Na⫹ channels. Am J Physiol Cell Physiol 281: C1477–C1486, 2001. 43. Zhang G, Ichimura T, Maier JA, Maciag T, and Stevens JL. A role for fibroblast growth factor type-1 in nephrogenic repair. Autocrine expression in rat kidney proximal tubule epithelial cells in vitro and in the regenerating epithelium following nephrotoxic damage by S-(1,1,2,2-tetrafluoroethyl)-L-cysteine in vivo. J Biol Chem 268: 11542–11547, 1993. 44. Zhang HY, McPherson BC, Liu H, Baman TS, Rock P, and Yao Z. H2O2 opens mitochondrial KATP channels and inhibits GABA receptors via protein kinase C-⑀ in cardiomyocytes. Am J Physiol Heart Circ Physiol 282: H1395–H1403, 2002. 45. Zhang J, Bolli R, Lalli J, Tang X-L, LI RCX, Zheng Y, Pass J, and Ping P. Ischemic preconditioning and phorbol ester redistribute protein kinase C ⑀ to the nucleus, sarcolemmal membranes, and mitochondria in rabbit myocardium (Abstract). Circulation 100: I-325, 1999. Downloaded from http://ajprenal.physiology.org/ by 10.220.32.246 on June 17, 2017 AJP-Renal Physiol • VOL 286 • FEBRUARY 2004 • www.ajprenal.org