Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
NADH:ubiquinone oxidoreductase (H+-translocating) wikipedia , lookup
Amino acid synthesis wikipedia , lookup
Nicotinamide adenine dinucleotide wikipedia , lookup
Mitochondrion wikipedia , lookup
Biosynthesis wikipedia , lookup
Adenosine triphosphate wikipedia , lookup
Oxidative phosphorylation wikipedia , lookup
Specialized pro-resolving mediators wikipedia , lookup
Metalloprotein wikipedia , lookup
Microbial metabolism wikipedia , lookup
Lactate dehydrogenase wikipedia , lookup
Butyric acid wikipedia , lookup
Basal metabolic rate wikipedia , lookup
Glyceroneogenesis wikipedia , lookup
Evolution of metal ions in biological systems wikipedia , lookup
Citric acid cycle wikipedia , lookup
Biochemistry wikipedia , lookup
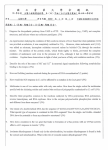
European Heart Journal Supplements (2001) 3 (Supplement O), O2–O7 Changes in cardiac metabolism: a critical step from stable angina to ischaemic cardiomyopathy W. C. Stanley Department of Physiology and Biophysics, School of Medicine, Case Western Reserve University, Cleveland, Ohio, U.S.A. Cardiac work requires a high rate of adenosine triphosphate (ATP) breakdown. ATP is resynthesized in the mitochondria with energy from the combustion of fatty acids, glucose and lactate. Fatty acids are the main fuel for the heart, supplying 60–90% of the energy, with the balance (10–40%) from pyruvate oxidation (formed from glycolysis and lactate). Fatty acid oxidation inhibits pyruvate oxidation in the mitochondria. During myocardial ischaemia, oxygen consumption and ATP production is reduced, causing accelerated glycolysis and lactate production; the pH falls and cell function is impaired. Paradoxically, with a partial reduction in coronary flow, the myocardium continues to derive most of its energy from the oxidation of fatty acids despite a high rate of lactate production; this fatty acid oxidation during ischaemia inhibits pyruvate oxidation, and drives pyruvate conversion to lactate. Partial inhibition of fatty acid oxidation in ischaemic myocardium, such as with the long-chain 3-ketoacyl thiolase inhibitor trimetazidine, reduces lactate production and H+ accumulation during ischaemia, and results in clinical benefit in patients with angina pectoris. (Eur Heart J Supplements 2001; 3 (Suppl O): O2–O7) © 2001 The European Society of Cardiology Introduction theless, many patients with coronary artery disease continue to have severe angina despite maximally tolerated traditional therapy or following revascularization procedures. Such patients would benefit from additional pharmacotherapy that would reduce the symptoms of ischaemia without further suppressing cardiac contractility, heart rate, or arterial blood pressure. An alternative or adjunctive treatment for myocardial ischaemia is to reduce the production and release of anginaproducing stimuli, and lessen the ischaemic burden of the patient by optimizing energy metabolism in the ischaemic myocardium[2]. This approach differs from traditional therapies (e.g. beta-adrenergic receptor antagonists, calcium channel blockers, or long-acting nitrates) in that there are no direct effects on coronary blood flow, heart rate, or afterload. Rather, these agents alter the metabolism of the ischaemic tissue so that there is less accumulation of lactate, and a lesser fall in intracellular pH and ATP. The present brief review presents the biochemical and physiological rationale for this pharmacological approach to treatment of chronic stable angina. The pump function of cardiac muscle is supported by high rates of myocardial blood flow, oxygen consumption, and combustion of fat and carbohydrates (glucose and lactate). Myocardial ischaemia occurs when there is a deficit between the normal rate of oxygen delivery to the myocardium required for a given heart rate, afterload and inotropic state, and the actual rate of oxygen delivery to the myocardium. The primary effect of ischaemia is mitochondrial metabolic dysfunction caused by reduced aerobic formation of adenosine triphosphate (ATP); this triggers accelerated anaerobic glycolysis and disruption of normal cardiac cell function[1,2]. Traditional therapies for ischaemia are aimed at restoring the balance between oxygen delivery and ATP formation, and the myocardial demand for ATP. This is achieved either by increasing blood flow to the myocardium via coronary vasodilatation, or by reducing the oxygen requirement of the ischaemic tissue through decreasing heart rate, arterial blood pressure and cardiac contractility. These haemodynamic approaches to the treatment of ischaemic heart disease have proven relatively effective at reducing the symptoms of angina and improving exercise time. NeverCorrespondence: William C. Stanley, PhD, Department of Physiology and Biophysics, School of Medicine, Case Western Reserve University, 10900 Euclid Avenue, Cleveland, OH 441064970, U.S.A. 1520-765X/01/0O0002 + 06 $35.00/0 Key Words: Angina pectoris, cardiac, coronary artery disease, fatty acids, glucose, heart, lactate, metabolism, mitochondria. Metabolism in healthy myocardium Before considering myocardial metabolism during ischaemia, it is important to have an understanding of metabolism in the normal healthy heart. © 2001 The European Society of Cardiology Myocardial metabolism in chronic stable angina O3 Cardiac function is maintained by the synthesis and breakdown of adenosine triphosphate Under conditions of normal coronary blood flow, ATP is broken down by myosin ATPase, releasing energy that fuels tension development and systolic work (Fig. 1). ATP breakdown is also employed by the sarcoplasmic reticulum Ca2+-ATPase to remove Ca2+ from the cytosol at the end of systole and allow for diastolic relaxation. Approximately two-thirds of the ATP used by the heart goes to contractile shortening, and the remaining one-third is used for the sarcoplasmic reticulum Ca2+-ATPase and other ion pumps[1,2]. ATP is constantly resynthesized from adenosine diphosphate and inorganic phosphate in the mitochondria by oxidative phosphorylation. In the healthy heart the processes of ATP synthesis and breakdown are exquisitely matched such that there is never a significant fall in ATP concentration, even with large increases in cardiac power output[3]. Fatty acids are the predominant fuel for the heart Fatty acids supply approximately 60–90% of the energy used to synthesize ATP in the healthy human heart (Fig. 1)[1–7]. The rate of fatty acid uptake by the heart is primarily determined by the concentration of fatty acids in the plasma[6], which varies widely between 0·1 and approximately 1·5 mmol . l – 1. Plasma fatty acids come from the breakdown of triglyceride in fat cells, and the broad range in plasma concentration is due to the hormonal control of hormone-sensitive lipase by insulin and noradrenaline (norepinephrine) in this tissue. Insulin suppresses fatty acid levels, and thus fatty acid levels are low when insulin levels are high after a meal. On the other hand, noradrenaline increases fatty acid release from fat cells so that fatty acid levels are elevated under times of stress, such as physical exercise, fasting, or myocardial ischaemia. Diabetic patients (both types 1 and 2) have high fatty acid levels because of low insulin levels and/or resistance to the normal insulin-induced suppression of fatty acid release from fat cells. Thus, during times of stress, when catecholamines are high and insulin is low, the heart is faced with a high plasma free fatty acid concentration, and fatty acid oxidation by the heart is high. Fatty acids are oxidized in the mitochondria, where they release energy in the form of reduced nicotinamide adenine dinucleotide (NADH) and reduced flavin adenine dinucleotide (FADH2) for the electron transport chain and the subsequent formation of ATP by oxidative phosphorylation (Fig. 2)[8]. On entering the cell, fatty acids are esterified to fatty acyl-coenzyme A (CoA), which makes the fatty acid more water-soluble. In order to cross the inner mitochondrial membrane, the fatty acid must be converted to fatty acylcarnitine by the enzyme carnitine palmitoyl transferase[8]. Once in the mitochondrion the fatty acid undergoes beta-oxidation, a process that repeatedly cleaves off two carbon acetyl-CoA units, generating NADH and Figure 1 Cardiac energy metabolism under normal aerobic conditions. Fatty acids are the primary source of energy for the heart, supplying 60–90% of the energy for adenosine triphosphate (ATP) synthesis. The balance (10–40%) comes from the oxidation of pyruvate formed from glycolysis and lactate oxidation. Almost all of the ATP formation comes from oxidative phosphorylation in the mitochondria; only a trivial amount of ATP (<2% of the total) is synthesized by glycolysis. ADP=adenosine diphosphate; SR=sarcoplasmic reticulum. FADH2 in the process. The acetyl-CoA is further oxidized to CO2 in the citric acid cycle. The rate of fatty acid betaoxidation is primarily regulated by the concentration of free fatty acids in the plasma, the activity of the carnitine transferase/translocase system on the mitochondrial membranes, and the activity of a series of enzymes that catalyze the multiple steps of fatty acid beta-oxidation (Fig. 2)[8]. Glucose and lactate metabolism Glucose and lactate supply between approximately 10% and 40% of the energy requirement of the heart (Fig. 1)[1,2,4,5,7]. Glucose is taken up by the myocardium and is either stored as glycogen, or broken down by glycolysis to pyruvate in the cytosol of the cell (Fig. 2). Lactate is extracted from the blood, converted to pyruvate in the cytosol, and further oxidized to acetyl-CoA in the mitochondrial matrix. In the normal healthy human heart, pyruvate is derived in approximately equal proportions from glycolysis and lactate uptake[4,5,7]. Pyruvate is oxidized to acetyl-CoA in the mitochondria by the enzyme pyruvate dehydrogenase (PDH; Fig. 3). The rate of flux of pyruvate to acetyl-CoA is determined by the amount of active enzyme present in the tissue and the concentration of the substrates (CoA, nicotinamide adenine dinucleotide [NAD+] and pyruvate), and the products (acetyl-CoA and NADH)[2,9]. Fatty acid oxidation inhibits glucose and lactate oxidation Oxidation of glucose and lactate is strongly inhibited by high rates of fatty acid oxidation in the heart[1,2,5,7,10,11]. Lowering plasma fatty acid concentration by pharmacological means (e.g. with niacin[12,13]), or directly inhibiting fatty acid Eur Heart J Supplements, Vol. 3 (Suppl O) November 2001 O4 W. C. Stanley Figure 2 Mitochondrial energy metabolism. Reduced nicotinamide adenine dinucleotide (NADH) and reduced flavin adenine dinucleotide (not shown) transfer electrons from fatty acids, glucose and lactate to the electron transport chain. The process of oxidative phosphorylation is driven by the electron transport chain, which takes the energy from the oxidation of fatty acids, glucose and lactate, primarily via NADH. ADP=adenosine diphosphate; ATP=adenosine triphosphate; CoA=coenzyme A; NAD+= nicotinamide adenine dinucleotide. oxidation in the mitochondria (e.g. with a carnitine palmitoyltransferase I inhibitor[14,15] or with the 3-ketoacyl thiolase [3-KAT] inhibitor trimetazidine[16]) will result in an increase in the rates of glucose and/or lactate uptake and oxidation. The molecular site of fatty acid inhibition of pyruvate oxidation (and thus glucose and lactate oxidation) is at the level of PDH. PDH and beta-oxidation of fatty acids yield the common products acetyl-CoA and NADH. Flux of pyruvate to acetyl-CoA is inhibited by acetyl-CoA and NADH, and thus high rates of fatty acid oxidation result in elevated NADH : NAD+ and acetyl-CoA : free CoA ratios, which strongly inhibit flux through PDH (Fig. 3)[2,9]. The amount of active enzyme is also under acute allosteric control by PDH kinase, which phosphorylates and inhibits PDH[2,9–11]. The activity of PDH kinase is stimulated by increases in the NADH : NAD+ and acetyl-CoA : free CoA ratios, and thus high rates of fatty acid oxidation stimulate PDH kinase and inhibit the rate of glucose and lactate oxidation by the heart. Studies conducted in humans and large animals have demonstrated that pharmacological inhibition of the rate of fatty acid oxidation by the heart accelerates the flux of pyruvate through PDH, and the uptake and oxidation of glucose and lactate by the heart[2,12,13,15]. Energy metabolism during ischaemia Accelerated glycolysis, lactate production and a fall in pH The primary result of ischaemia is mitochondrial metabolic dysfunction caused by reduced oxygen delivery to the Eur Heart J Supplements, Vol. 3 (Suppl O) November 2001 Figure 3 Regulation of pyruvate oxidation under normal aerobic conditions. Pyruvate is formed in the cytosol from glycolysis and lactate oxidation, and is converted to acetyl-coenzyme A (CoA) in the mitochondria by pyruvate dehydrogenase (PDH). The acetyl-CoA and reduced nicotinamide adenine dinucleotide (NADH) generated by fatty acid oxidation inhibit flux through PDH. Pharmacological inhibition of the rate of fatty acid oxidation removes inhibition of flux through PDH by NADH and acetyl-CoA, and results in more pyruvate oxidation and thus more glucose and lactate uptake. tissue, resulting in a decrease in ATP formation by oxidative phosphorylation (Fig. 4)[1,2,17]. The reduction in aerobic ATP formation stimulates glycolysis, and an increase in myocardial glucose uptake and glycogen breakdown occurs[1,2]. Unlike under conditions of normal blood flow, however, during ischaemia pyruvate produced by glycolysis is not so readily oxidized in the mitochondria, and there is a high rate of conversion of pyruvate to lactate in the cytosol, and a rise in tissue lactate content. Instead of the normal uptake of lactate from the blood, the ischaemic myocardium switches to production of lactate. Cell homeostatis is dramatically disrupted; there is accumulation of lactate and H+, a fall in intracellular pH, and a reduction in contractile work (Fig. 4). Thus, during ischaemia there is accelerated glycolysis and pyruvate formation concurrent with impaired pyruvate oxidation in the mitochondria, which results in lactate accumulation in the tissue. The ischaemia-induced fall in intracellular pH has several negative effects on the ability of cardiac muscle to maintain Ca2+ homeostatis and use the energy released from the breakdown of ATP to perform contractile work. First, the amount of ATP required by the sarcoplasmic Ca2+ pump is greater when pH is decreased[18]. Second, the Ca2+ concentration for a given amount of force generation is greater at a lower pH, and thus a higher cytosolic Ca2+ concentration is required during systole to produce a given amount of mechanical power[18]. Thus, at low pH, for a given rate of ATP synthesis, more of the energy released from ATP breakdown contributes to the ‘chemical work’ of regulating Ca2+ content in the cytosol, and less to contractile work. In addition, the efflux of H+ from the cardiomyocyte Myocardial metabolism in chronic stable angina O5 High rates of fatty acid oxidation inhibit pyruvate oxidation during ischaemia Figure 4 Cardiac energy metabolism during ischaemia of moderate severity (approximately 40% of normal blood flow). The up and down arrows indicate the changes compared with normal aerobic conditions. Relative to aerobic conditions, ischaemia results in an increase in glycolysis without an increase in the rate of pyruvate oxidation, thus causing lactate to accumulate in the cell. Despite accelerated glycolysis and lactate production, the relatively high rate of residual oxygen consumption is fuelled primarily by the oxidation of fatty acids. ADP=adenosine diphosphate; ATP= adenosine triphosphate; Pi=inorganic phosphate. that occurs in exchange for Na+ leads to a greater Na+–Ca2+ exchange across the cell membrane, and further wasting of ATP in order to maintain Ca2+ homeostasis[19]. Fatty acids are the main fuel for the mitochondria during partial ischaemia During moderate myocardial ischaemia, the residual oxygen consumption is largely supported by the oxidation of fatty acids (Fig. 4)[2,8,17,20]. In fact, the relative contribution of fatty acids to the energy requirement of the myocardium is not significantly affected by ischaemia of moderate severity[2,17,20]. Studies conducted in large animal models show that reductions in coronary blood flow of 30–60% do not affect the relative contribution of fatty acids to mitochondrial oxygen consumption, despite a dramatic switch to lactate production. In studies conducted in swine and dogs using isotopically labelled glucose and fatty acid tracers, there was a continued high rate of fatty acid oxidation with an increase in the relative contribution of glucose to mitochondrial oxidative metabolism when coronary blood flow was reduced by 30–60%[2,17,20]. Even though there was a switch from lactate uptake to lactate production and a decrease in myocardial ATP content during ischaemia, fatty acid continued to be the predominant fuel for the heart. It is important to note that patients undergoing myocardial ischaemia have very high plasma free fatty acid concentrations (>1·0 mmol . l – 1) because of activation of the peripheral sympathetic nervous system[21], which would fuel a high relative contribution of fatty acid to myocardial substrate oxidation. The impaired pyruvate oxidation during ischaemia of moderate severity is due to the rise in mitochondrial NADH secondary to the fall in oxygen consumption and to the high rates of fatty acid oxidation. During moderate ischaemia, there is a build-up of NADH and a rise in the NADH : NAD+ ratio in the mitochondria, which feedback and inhibit flux through PDH via product inhibition (Fig. 5). The build-up of NADH during ischaemia is the result of the decrease in oxygen consumption and electron transport chain flux, resulting in a back-up of NADH oxidation and a fall in NAD+ content. Studies conducted in pigs and dogs showed that ischaemia does not decrease the degree of direct PDH inhibition by phosphorylation[2,22,23], suggesting that the impairment in the in vivo rate of pyruvate oxidation during ischaemia is not due to deactivation of the enzyme, but rather to product inhibition by an increase in the NADH : NAD+ ratio. Optimization of energy metabolism during ischaemia Myocardial ischaemia is treated with drugs that are aimed at restoring normal metabolism by the following mechanisms: delivering more oxygen to the tissue via coronary vasodilatation; decreasing the demand for mitochondrial oxygen consumption by reducing arterial blood pressure, contractility and heart rate; or optimizing myocardial metabolism by decreasing fatty acid oxidation and stimulating pyruvate oxidation in the mitochondria (e.g. by the use of glucose–insulin–potassium therapy for acute myocardial infarction, or trimetazidine for stable angina)[1,2]. Metabolic agents that suppress fatty acid oxidation and increase the oxidation of pyruvate by PDH in the mitochondria will reduce the ischaemia-induced disruption in cardiac metabolism[2]. In other words, inhibiting cardiac fatty acid oxidation and increasing the oxidation of pyruvate results in less lactate production and less of a fall in cell pH, with clinical benefit to the ischaemic patient[2,24–27]. This direct metabolic approach is optimally suited to conditions in which there is sufficient residual oxygen delivery to the myocardium to support pyruvate oxidation in the mitochondria. In other words, it is important that there be a sufficient rate of acetyl-CoA oxidation and oxygen consumption so that increasing the rate of pyruvate oxidation has a meaningful effect on the rate of lactate production. Metabolic interventions clearly work well with demand-induced ischaemia (e.g. exercise-induced angina), as has been observed in several positive trials with the 3KAT inhibitors trimetazidine and ranolazine, which partly reduce fatty acid oxidation[25–27]. Those agents show clear clinical benefit, as reflected in improved exercise duration, without eliciting any direct effects on heart rate or blood pressure. Eur Heart J Supplements, Vol. 3 (Suppl O) November 2001 O6 W. C. Stanley Figure 5 Pyruvate oxidation during ischaemia. There is accelerated glycolysis and lactate production in the cytosol. In the mitochondria there is a rise in the ratio of reduced nicotinamide adenine dinucleotide (NADH) to oxidized nicotinamide adenine dinucleotide (NAD+) due to a decrease in oxygen consumption and continued fatty acid oxidation. Pharmacologically inhibiting fatty acid oxidation (e.g. with the 3-ketoacyl thiolase inhibitor trimetazidine) during ischaemia removes inhibition of pyruvate dehydrogenase (PDH) by NADH and acetylcoenzyme A (CoA), and results in more pyruvate oxidation and reduced symptoms of angina. Conclusion Myocardial ischaemia of moderate severity dramatically alters fuel metabolism, reducing the rate of oxygen consumption and ATP production. This leads to a fall in ATP content, high rates of glycolysis, pyruvate formation and lactate accumulation, and a fall in intracellular pH. The myocardium continues to derive most of its energy (50–70%) from the oxidation of fatty acids. Despite the high rate of lactate production during ischaemia, pyruvate oxidation is inhibited by fatty acid oxidation, which contributes to the accelerated lactate production, intracellular acidosis and general disruption to cell homeostatis. Ischaemia-induced dysfunction can be minimized by metabolic agents that partly inhibit fatty acid oxidation, and increase the combustion of glucose and lactate. References [1] Opie L. The Heart: Physiology, from Cell to Circulation. Philadelphia, Lippincott-Raven, 1998. [2] Stanley WC, Lopaschuk GD, Hall JL, McCormack JG. Regulation of myocardial carbohydrate metabolism under normal and ischaemic conditions: potential for pharmacological interventions. Cardiovasc Res 1997; 33: 243–57. [3] Balaban RS, Kantor HL, Katz LA, Briggs RW. Relation between work and phosphate metabolite in the in vivo paced mammalian heart. Science 1986; 232: 1121–3. [4] Gertz EW, Wisneski JA, Stanley WC, Neese RA. Myocardial substrate utilization during exercise in humans: dual carbon-labeled carbohydrate isotope experiments. J Clin Invest 1988; 82: 2017–25. Eur Heart J Supplements, Vol. 3 (Suppl O) November 2001 [5] Wisneski JA, Gertz EW, Neese RA, Gruenke LD, Morris DL, Craig JC. Metabolic fate of extracted glucose in normal human myocardium. J Clin Invest 1985; 76: 1819–27. [6] Wisneski JA, Gertz EW, Neese RA, Mayr M. Myocardial metabolism of free fatty acids: studies with 14C-labeled substrates in humans. J Clin Invest 1987; 79: 359–66. [7] Wisneski JA, Stanley WC, Gertz EW, Neese RA. Effects of hyperglycemia on myocardial glycolytic activity in normal humans. J Clin Invest 1990; 85: 1648–56. [8] Lopaschuk GD, Belke DD, Gamble J, Itoi T, Schonekess BO. Regulation of fatty acid oxidation in the mammalian heart in health and disease. Biochim Biophys Acta 1994; 1213: 263–76. [9] Hansford RG, Cohen L. Relative importance of pyruvate dehydrogenase interconversion and feed-back inhibition in the effect of fatty acids on pyruvate oxidation by rat heart mitochondria. Arch Biochem Biophys 1978; 191: 65–81. [10] Randle PJ, Hales CN, Garland PB, Newsholme EA. The glucose fatty-acid cycle. Its role in insulin sensitivity and the metabolic disturbances of diabetes mellitus. Lancet 1963; ii: 785–9. [11] Randle PJ, Newsholme EA, Garland PB. Regulation of glucose uptake by muscle. Effects of fatty acids, ketone bodies and pyruvate, and of alloxan diabetes and starvation, on the uptake and metabolic fate of glucose in rat heart and diaphragm muscles. Biochem J 1964; 93: 652–65. [12] Lassers BW, Wahlqvist ML, Kaijser L, Carlson LA. Effect of nicotinic acid on myocardial metabolism in man at rest and during exercise. J Appl Physiol 1972; 33: 72–80. [13] Stone CK, Holden J, Stanley WC, Perlman SB. Effect of substrate availability upon cardiac glucose uptake. J Nucl Med 1995; 36: 996–1002. [14] Lopaschuk GD, Spafford M, Davies NJ, Wall SR. Glucose and palmitate oxidation in isolated working rat hearts reperfused following a period of transient global ischemia. Circ Res 1990; 66: 546–53. [15] Schwartz GG, Greyson C, Wisneski JA, Garcia J. Inhibition of fatty acid metabolism alters myocardial high-energy phosphates in vivo. Am J Physiol 1994; 267: H224–31. [16] Kantor PF, Lucien A, Kozak R, Lopaschuk GD. The antianginal drug trimetazidine shifts cardiac energy metabolism from fatty acid oxidation to glucose oxidation by inhibiting mitochondrial long-chain 3-ketoacyl coenzyme A thiolase. Circ Res 2000; 86: 580–8. [17] Liedtke AJ. Alterations in carbohydrate and lipid metabolism in the acutely ischemic heart. Prog Cardiovasc Dis 1981; 23: 321–6. [18] Fabiato A, Fabiato F. Effects of pH on the myofilaments and the sarcoplasmic reticulum of skinned cells from cardiac and skeletal muscles. J Physiol (Lond) 1978; 276: 233–55. [19] Murphy E, Perlman M, London RE, Steenbergen C. Amiloride delays the ischemia-induced rise in cytosolic free calcium. Circ Res 1991; 68: 1250–8. [20] McNulty PH, Sinusas AJ, Shi CQ et al. Glucose metabolism distal to a critical coronary stenosis in a canine model of low-flow myocardial ischemia. J Clin Invest 1996; 98: 62–9. [21] Lopaschuk GD, Collins-Nakai R, Olley PM et al. Plasma fatty acid levels in infants and adults after myocardial ischemia. Am Heart J 1994; 128: 61–7. [22] Stanley WC, Hernandez LA, Spires DA, Bringas J, Wallace S, McCormack JG. Pyruvate dehydrogenase activity and malonyl CoA levels in normal and ischemic swine myocardium: effects of dichloroacetate. J Mol Cell Cardiol 1996; 29: 905–14. [23] Schoder H, Knight RJ, Kofoed KF, Schelbert HR, Buxton DB. Regulation of pyruvate dehydrogenase activity and glucose metabolism in post-ischaemic myocardium. Biochim Biophys Acta 1998; 1406: 62–72. [24] Bergman G, Atkinson L, Metcalfe J, Jackson J, Jewitt DE. Beneficial effect of enhanced myocardial carbohydrate utilisation after oxfenicine (L-hydroxyphenylglycine) in angina pectoris. Eur Heart J 1980; 1: 247–53. [25] Dalla-Volta S, Maraglino G, Della-Valentina P, Viena P, Desideri A. Comparison of trimetazidine with nifedipine in effort angina: a double-blind, crossover study. Cardiovasc Drugs Ther 1990; 4: 853–60. Myocardial metabolism in chronic stable angina [26] McCormack JG, Stanley WC, Wolff AA. Pharmacology of ranolazine: a novel metabolic modulator for the treatment of angina. Gen Pharmacol 1998; 30: 639–45. O7 [27] Detry JM, Sellier P, Pennaforte S, Cokkinos D, Dargie H, Mathes P. Trimetazidine: a new concept in the treatment of angina. Comparison with propanolol in patients with stable angina. Br J Clin Pharmacol 1994; 37: 279–88. Eur Heart J Supplements, Vol. 3 (Suppl O) November 2001