Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Rheumatic fever wikipedia , lookup
DNA vaccination wikipedia , lookup
Complement system wikipedia , lookup
Lymphopoiesis wikipedia , lookup
Sjögren syndrome wikipedia , lookup
Immune system wikipedia , lookup
Psychoneuroimmunology wikipedia , lookup
Adaptive immune system wikipedia , lookup
Molecular mimicry wikipedia , lookup
Innate immune system wikipedia , lookup
Monoclonal antibody wikipedia , lookup
Adoptive cell transfer wikipedia , lookup
Cancer immunotherapy wikipedia , lookup
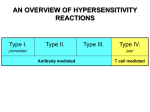
Lecture 11 Immune System & its Diseases II Dr. Yasmine Lashine MD, PhD 1 ILOs • • • • • • • • • • • • • Distinguish between innate and adaptive immunity. Recall the cells involved in the immune response and define their roles. Compare and contrast the origin, maturation process, and general function of B and T lymphocytes. Name several antigen-presenting cells and describe their roles in adaptive defenses. Understand the mechanisms and key players of humoral immunity. Define cellular immunity and describe the process of activation. Describe the roles of different types of T cells and their functions in the body. Discuss the possible mechanisms of graft rejection and the role of MHC molecules. Compare and contrast the types and subtypes of hypersensitivity disorders in terms of examples, pathogenesis, clinical features, key players, antigens… Define self-tolerance, and describe its development in B and T lymphocytes. Give examples of immune deficiency diseases and differentiate between primary and secondary immune deficiencies. Understand the pathogenesis of HIV infection and rheumatoid arthritis. Cite examples of autoimmune diseases and understand their mechanisms. 2 Outline 1. Types of Hypersensitivity Reactions • Type I Hypersensitivity Reactions • Type II Hypersensitivity Reactions - Complement-dependent Reactions - Antibody-mediated Cellular Cytotoxicity - Cellular Dysfunction • Type III Hypersensitivity Reactions • Type IV Hypersensitivity Reactions - Delayed-Type Hypersensitivity - T cell-Mediated Cytotoxicity 2. Transplant Rejection 3 Type I Hypersensitivity Reactions http://steamcleaning-austin.com/services/allergy-relief/ http://thetreatmentherbs.com/pollen-allergy-and-herbs/ 4 http://www.healthspablog.org/allergy/allergy-to-dust-invented-new-vaccine Type I Hypersensitivity Reactions Inhalation Ingestion Environmental antigens (allergens) Injection Activation of Th2 cells Cytokine release Activation of TH2 cells and production of IgE antibody Production of IgE antibodies from B cells Attachment of IgE to mast cells Re-exposure to the allergen Sensitization of mast cells by IgE antibody Activation of mast cells and Mediators release Clinical manifestation Inhalation, ingestion, or injection TH2 subset of CD4+ helper T cells 6 Leukocyte activation Amplification of Th2-initiated reaction Stimulation of cell mucus secretion 5-30 min to 1 hour 2-8 hours to several days The dominant inflammatory cells in the latephase reaction are neutrophils, eosinophils, and lymphocytes, especially TH2 cells 7 Type I Hypersensitivity Reactions Mediators of immediate hypersensitivity reaction Vasoactive amines released from granule stores: • Histamine causes vasodilation, increased vascular permeability, smooth muscle contraction, and increased secretion of mucus. • Adenosine causes bronchoconstriction and inhibits platelet aggregation. • Chemotactic factors for neutrophils and eosinophils. Newly synthesized lipid mediators: • Prostaglandin D2 (PGD2) Causes intense bronchospasm and increased mucus secretion • Leukotrienes C4 and D4 (LTC4, LTD4) are the most potent vasoactive and spasmogenic agents . LTB4 is highly chemotactic for neutrophils, eosinophils, and monocytes • Platelet-activating factor (PAF): platelet aggregation, bronchospasm, chemotaxis Cytokines: • TNF and chemokines recruit and activate leukocytes. • IL-4 and IL-5 amplify the Th2-initiated immune reaction. • IL-13 stimulates epithelial cell mucus secretion. 8 Type I Hypersensitivity Reactions Local manifestation Skin contact : urticaria Ingestion : GIT manifestation as vomiting and diarrhea Inhalation Seosonal allergy Runny and stuffy nose Sneezing Sore throat Redness in the eyes Asthma Coughing Wheezing Shortness of breath 9 Type I Hypersensitivity Reactions systemic manifestation Drugs as penicillin Parenteral administration of Antigens as snake venom or bee sting Itching , urticarial , skin erythema Profound respiratory difficulty ( bronchoconstriction and increased mucous secretion) Laryngeal edema Upper airway obstruction Vomiting , abdominal pain and diarrhea Systemic vasodilatation Anaphylactic shock Circulatory collapse Within minutes Death 10 Type I Hypersensitivity Reactions Clinical and pathologic manifestation 2014 Health Care & Alternative Medicine Epinephrine! 11 http://www.firstaidanywhere.com/bee-sting-first-aid.html Type I Hypersensitivity Reactions Type I HS in Parasitic Infections 12 Case • Every springtime, a young healthy man is bothered by episodes of nasal congestion accompanied by sneezing and watery eyes. He has no cough. On physical examination he is afebrile. There is swelling of his nasal passageways, but no other findings. His condition improves with use of loratadine. His problems are most likely produced by release of chemical mediators from which of the following cell types? • Neutrophil • Mast cell • CD4+ cell • NK cell 13 Type II Hypersensitivity Reactions Antibody-Mediated Diseases This reaction is mediated through Antibodies that are directed against target antigens on the surface of cells or other tissue components Cell-mediated cytotoxicity Complementdependent ADCC reactions Antibody mediated cellular dysfunction Type II hypersensitivity reaction 14 Type II Hypersensitivity Reactions Complement-dependent reactions Opsonization and phagocytosis 15 Type II Hypersensitivity Reactions Complement-dependent reactions Examples: Transfusion reactions Erythroblastosis fetalis (hemolytic disease of the newborn) Autoimmune hemolytic anemia 16 Type II Hypersensitivity Reactions Complement-dependent reactions Transfusion reactions 17 Type II Hypersensitivity Reactions Complement-dependent reactions Erythroblastosis fetalis 18 Type II Hypersensitivity Reactions Antibody-Dependent Cellular Cytotoxicity (ADCC): 19 Cell-mediated killing of parasites Type II Hypersensitivity Reactions Antibody mediated cellular dysfunction Graves Disease Myasthenia Gravis Antibodies against the thyroid-stimulating hormone receptor stimulate thyroid epithelial cells to secrete thyroid hormones, resulting in hyperthyroidism Antibodies against acetylcholine receptors in the motor end plates of skeletal muscles inhibit neuromuscular transmission, with resultant muscle weakness 20 Type II Hypersensitivity Reactions Antibody mediated cellular dysfunction Graves Disease 21 Type II Hypersensitivity Reactions Disease Target Antigen Mechanisms of Disease Autoimmune hemolytic anemia Erythrocyte membrane proteins Opsonization and Hemolysis, anemia phagocytosis of erythrocytes Acute rheumatic fever Streptococcal cell wall Inflammation, macrophage antigen; antibody crossactivation reacts with myocardial antigen (Molecular mimicry) Myasthenia gravis Acetylcholine receptor Antibody inhibits Muscle weakness, acetylcholine binding, down- paralysis modulates receptors Graves disease (hyperthyroidism) TSH receptor Antibody-mediated Hyperthyroidism stimulation of TSH receptors Examples of Antibody-Mediated Diseases (Type II Hypersensitivity) Clinico pathologic Manifestations Myocarditis, arthritis 22 Immune Complex Diseases (Type III Hypersensitivity) Endogenous Antigen DNA Antigenantibody Deposition in blood vessels Immune Exogenous Complex Microbial Antigen Complement activation Vasculitis Arthritis Glomerulonephritis Antigen-antibody complex deposition Can cause Local injury when affecting particular organs as kidney or joints , and can also cause Systemic injury by affecting multiple organs 23 Systemic Immune-Complex Disease: Serum sickness The use of horse anti-thymocyte globulins for the treatment of severe aplastic anemia 5 days after injection • • Production of specific antibodies Formation of antigen-antibody complex Deposition of immune complex Inflammatory reaction and clinical manifestation occurs -10 days Fever – Urticaria-Arthralgias Lymph node enlargement-Proteinuria 24 Type III Hypersensitivity Disease Antigen Involved Clinicopathologic Manifestations Systemic lupus erythematosus Nuclear antigens Nephritis, skin lesions, arthritis, others Poststreptococcal glomerulonephritis Streptococcal cell wall Nephritis antigen(s); may be "planted" in glomerular basement membrane Serum sickness Various proteins, such as Arthritis, vasculitis, nephritis foreign serum protein (horse anti-thymocyte globulin) Arthus reaction (experimental) Various foreign proteins Cutaneous vasculitis 25 Case • A 9-year-old boy has a sore throat. A throat culture grows group A hemolytic streptococcus. He receives antibiotic therapy. However, 17 days later he develops dark-coloured urine. Laboratory studies show 3+ blood on urinalysis. A renal biopsy is performed. On immunofluorescence staining the biopsy shows granular deposition of IgG and complement around glomerular capillary loops. Which of the following immune hypersensitivity mechanisms is most likely responsible for this pattern of findings? • Type I • Type II • Type III • Type IV 26 Type IV Hypersensitivity (Cell-Mediated) 27 Tuberculin reaction Antigen challenge test in an individual already sensitized to the tubercle bacillus by a previous infection 8-12 hours after injection Intracutaneous injection of tuberculin local area of erythema and induration appears, reaching a peak (typically 1-2 cm in diameter) in 24 to 72 hours HIV ? 28 Type IV Hypersensitivity Delayed – Type hypersensitivity Granulomatous Inflammation The initial CD4+ T-cell infiltrate is progressively replaced by macrophages over a period of 2 to 3 weeks. These macrophages become large, and flat (epithelioid cells). The epithelioid cells occasionally fuse under the influence of cytokines (e.g., IFN-γ) to form multinucleated giant cells. 29 Type IV Hypersensitivity (Cell-Mediated) T –cell mediated cytotoxicity CD8+ CTLs is the main key player in this reaction kill antigen-bearing target cells. Class I MHC molecules bind to intracellular peptide antigens and present the peptides to CD8+ T lymphocytes, stimulating the differentiation of these T cells into effector cells called CTLs. CTLs play a critical role in resistance to virus infections and some tumors. 30 Transplant Rejection Immunologic rejection of transplanted tissue is considered the major barrier to transplantation of organs between individuals of the same species (allografts ). Cell mediated hypersensitivity Directed against donor’s MHC molecules Antibody mediated hypersensitivity Tissue rejection Classic acute rejection in a non-immunosuppressed host occurs within 10 to 14 days and includes both DTH and CTL 31 Transplant Rejection Direct recognition Host T cells directly recognize the allogeneic (foreign) MHC molecules that are expressed on graft cells. Indirect recognition Host CD4+ T cells recognize donor MHC molecules after these molecules are picked up, processed and presented by the host's own 32 APCs. Transplant Rejection T –cell mediated rejection CTLs kill cells in the grafted tissue, causing parenchymal and, perhaps more importantly, endothelial cell death (resulting in thrombosis and graft ischemia). Cytokine-secreting CD4+ T cells trigger DTH reactions, with increased vascular permeability and local accumulation of mononuclear cells (lymphocytes and macrophages). Antibody mediated rejection Antibodies directed against graft MHC molecules bind to the graft endothelium and cause injury (and secondary thrombosis) via complement activation and recruitment of leukocytes. 33 Transplant Rejection T –cell mediated rejection CTLs kill cells in the grafted tissue, causing parenchymal and, perhaps more importantly, endothelial cell death (resulting in thrombosis and graft ischemia). Cytokine-secreting CD4+ T cells trigger DTH reactions, with increased vascular permeability and local accumulation of mononuclear cells (lymphocytes and macrophages). Antibody mediated rejection Antibodies directed against graft MHC molecules bind to the graft endothelium and cause injury (and secondary thrombosis) via complement activation and recruitment of leukocytes. 34 35 Transplant Rejection Hyperacute rejection A special form of rejection occurring in the setting where preformed antidonor antibodies are present in the circulation of the host before transplant. Transplantation in this setting results in immediate rejection (within minutes to hours) because the circulating antibodies rapidly bind to the endothelium of the grafted organ, with subsequent complement activation and vascular thrombosis. 36 References • • Basic Pathology 8th and 9th Edition, by Kumar, Cotran and Robbins Previous lectures by Dr. Nabila Hamdi 37 38