Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
From www.bloodjournal.org by guest on June 14, 2017. For personal use only.
Impaired
Responsiveness
to B Cell
Variable
Common
variable
syndrome
Robert
hypogammaglobulinemia
that
heterogeneous
ation
defects
and
capable
terminal
study,
This
report
intrinsic
patient’s
hemolytic
B
with
cells
respectively).
showed
2 v 93
cells
(5
their
responsiveness
±
tioned
media
impaired
this
8.
±
nemia
in
this
bymphoid
disorder
cell
antibody
humoral
syndrome
In some
to the process
cells capable
per
B cells
When
culture.
examined
cell
B cells
with
ty,”
specific
the
presence
from a variety
abnormality
the
The
differentiation
and secretion
differentiation
of serum
using
1985
in vitro
antigen’4
of circuin tissue
to
of
been
more
at stimulation
usually
have
in vitro stimumay now allow
Minneapolis.
a
proliferative
separate
these
state.
signals
signals
by T cells.
generation
by the
and
interleukin
Vol
66.
and
B cells
for proliferation
appear
recent
and
to be provided
have
capable
to and
appear
demonstration
to
Both
by lymphokines
secreted
of decreased
1985:
pp 345-349
with
and
an
first,
impaired
and.
patient’s
second,
T cells.
Inc.
of
to have
an
by disordered
2 production
and
2 have
been
immunodeficiency
of a patient
with
function
appears
manifested
BCGF.
identified
disease.22
CVH
whose
to be the
result
by an impaired
In addition,
this
impairment
in BCGF
production.
T cell suppressive
AND
effect
of
responpatient
No
was
noted
METHODS
the Department
School
and the
in part
of Medicine,
University
Veterans
Administration
by the
lnstitutes
Veterans
of Health
Associate
Administration
grant
at the
Veterans
10, 1984;
accepted
of Minnesota
Medical
Center,
No.
Merit
Al
18160.
Administration
Review
R. T.P.
Medical
is a
Cen-
Minneapolis.
Submitted
Section
©
Sept
reprint
(1 1 IE),
Minneapolis.
I
lupus
ter,
Address
in the
strength-
interleukin
systemic
to interleukin
in immune
National
Research
require
differentiation.
in patients
no
decreased
involve.
by
disease
characterized
Defective
interleukin
responsiveness
Supported
of delivmaintain
importance
of lymphokines
immune
response
has been
2 production
No 2 (August).
differentiation
is a lymphokine
B cells to commit
Human
The potential
of a normal
ened
Blood,
proliferation
or
signal
by the
and
showed
One 29-year-old
female with CVH and multiple healthy, age- and
sex-matched
volunteer
donors were studied.
Informed
consent was
obtained
from both the patient and the volunteers.
The patient,
previously
healthy,
presented
at age 26 with three
years of recurrent
respiratory
tract infections.
Severe hypogammaglobulinemia
was found. No serologic or biopsy evidence of autoimmune or lymphoproliferative
disease was identified.
Her peripheral
blood
counts (including
B and T lymphocyte
numbers)
and bone
marrow cellular
morphology
were normal.
Her clinical course has
been complicated
by several bouts of Hemophilus
influenzae
pneumonia and bacterial
meningitis.
Peripheral
blood mononuclear
cells were isolated
from venous
blood by Ficoll-Hypaque.
Monocyte
depletion
was done by adherence in tissue culture flasks for 45 minutes at 37 #{176}C
in 5% CO2 and
the nonadherent
cells were harvested.
Nonadherent
cells were then
regulation
B cell
defects
proliferation
for
1.4.
±
proliferation
immune
MATERIALS
differentiation
to
cells. The creation
using
CVH
v 26
cells
characterized
& Stratton.
evidence
for an enhanced
in this patient.
in individual
have
T
effect
of BCGF
by Grune
of B cell
with
support
0.21
±
suppressive
to BCGF’s
production
appeared
From
Medical
of
defect
an intrinsic
B cell defect
siveness
to the lymphokine
of enhanced
T cell activi-
or mitogen’5
B cell hybnidomas
from patients
with
identified.’72#{176} BCGF
a signal to activated
patient’s
abnormality
for further
dissection
of this disease
at the B cell level.’6
Recently,
T cell-derived
lymphokines
such
as B cell
growth
factor
(BCGF)
with
specific
effects
on immune
been
ering
This
B cell
in
be secondary
inhibitors’2”3
to induce
their
proliferation
or
i mmunogbobulin-secreting
plasma
of human-human
bated lymphocytes
effect.
intrinsic
enhanced
compared
less
patient’s
in
and
into plasma
of immuno-
may
attempts
In vivo and
B cells
of an
PHA-TCM
when
1 .27
studies
synthesis,
20%
by the
concentrations
showed
(SI
In coculture
with
Additionally.
consistently
in some patients
with primary
We report
here the study
of immunologic
appears
limited
in CVH
failed
mature
an
increasing
T cells
proliferation
respectively).
S
the steps required
for the normal
CVH is not a single disorder
but
difficult
of these
B cell
impaired
abnormalities
patients
with CVH.
Intrinsic
defects
in B cell function
to assess.
control
patient’s
1 .4
±
proliferation
B cells
interaction,
have
included
the demonstration
T cell activity,8’#{176} defective
helper
and
PHA-TCM
responsiveness
displayed
to an intrinsic
B cell defect6’7 or to extrinsic
factors
known
be capable
of modulating
B cell development.8
Examples
the latter
suppressor
the
defective
in cell-cell
B cell
(BCGF).
all immunogbobulin
classes.’
to the severe
hypogammagbobuli-
resulting
patients
arrested
for
condi-
control
with
factor
control
helper
B
Impaired
persisted
erythematosus,
a
immune
regulation.2’
include
Common
v 26
0.20
±
growth
from
evidence
control
1 .3
B cells
B cell
immunoglobulin
displayed
with
patient’s
of terminal
B cell
of normal
synthesis
This
in
com-
globulin.
These
patients
may have normal
numbers
bating
B cells but develop
few or no plasma
cells
sites.5
CVH.
[SI]
[vol/vol]).
BLE
hypogammagbobulinemia
characterized
by severe hypogam-
differentiation,
biosynthesis-all
immune
response.
a clinical
defects.2
HePFCs
compared
involving
leading
of
prepared
impairment
compared
the
OM MON
VA RIA
(CVH)
is a disorder
magbobulinemia
described
defects
with
index
PHA-TCM
patient’s
cells
secretion.
phytohemagglutinin-T
proliferation
prolifer-
formation
respectively).
to
(PHA-TCM).
B cell
marked
patient’s
formation
With
J. Weisdorf
control
of a previously
(HePFC)
(1 5 v 80
B cells
colony
and
in a patient
a
cell
in a Patient
(stimulation
with
plasma
synthesis
defect
In addition,
B cell
B cell
mature
identification
B cell
control
decreased
into
is a clini-
of patients
in impaired
our
plaque-forming
pared
group
immunoglobulin
we
undescribed
resulting
T. Perri and Daniel
(CVH)
a diverse
differentiation
of normal
In this
C
includes
Factor
Hypogammaglobulinemia
By
cal
Growth
/985
MN
by Grune
requests
VA
Medical
to
Dr
Feb
1 1. /985.
Robert
Center,
T.
54th
Perri,
St
&
Hematology
48th
Ave
S.
55417.
& Stratton,
Inc.
0006-497l/85/6602-0020$03.00/0
345
From www.bloodjournal.org by guest on June 14, 2017. For personal use only.
346
PEARl
allowed
to rosette
with
2-aminoethylisothiouronium
bromide
(AET)-sensitized
sheep erythrocytes
(SRBC)
at 4 #{176}C
for two hours.
Rosetted cells (96%
T cells) were separated
from the nonrosetted
B
and null cells (90%
slg+)
by two successive
Ficoll gradients.
SRBCs
were removed
by hypotonic
lysis with distilled
water. The
population
of double nonrosetted
cells was used as B cells in the
following
procedures.
T cell contamination
in this nonrosetted
B
cell-enriched
population
was < 1% as determined
by OKT3 reactivity.
Phytohemagglutinin
(PHA)-T
cell conditioned
medium
(PHA1CM)
was prepared
by incubating
T cells with 1% PHA
in growth
media at 37 #{176}C
with 5% CO2 for three days. Supernatants
were then
collected,
filtered, and stored at 4 #{176}C.
B cell colony
assay.
The B cell colony assay was performed
as
described
previously.23’24
In brief, the initiating
B cells were suspended to 2 x 105/mL in the presence
of 3 x l05/mL
irradiated
T
cells in a-MEM
with 10% fetal calf serum (FCS; GIBCO,
Grand
Island,
NY), 20% PHA-TCM,
and 0.8% methylcellulose.
After
vortexing,
0.I-mL
aliquots
were placed into 6-mm flat-bottomed
microtiter
wells (Linbro,
Hamden,
Conn).
Plates
were secured
tightly and incubated
at 37 #{176}C
with 5% CO2 for five to seven days,
and colonies
were enumerated
microscopically.
All experiments
were done in triplicate.
B cell proliferation
assay.
B cell proliferation
was studied using
5 x l0 B cells in 0.2 mL a-MEM
with 10% FCS plus 1% (vol/vol)
staphylococcal
protein A (SPA; Sigma Chemical
Co. St Louis) in
the presence
of varying concentrations
of human
BCGF (Cellular
Products,
Buffalo,
NY) or PHA-TCM
in 6-mm
flat-bottomed
microtiter
wells. BCG F was prepared
as previously
described.227
The purification
scheme yielded a product
free of immune
interferon, interleukin
1, and interleukin
2. This BCGF supports
both the
short-term
proliferation
of activated
human B cells25’26 as well as the
proliferation
of human B cells in long-term
culture.27 Cultures
were
incubated
for three days at 37 #{176}C
with 5% CO2 and pulsed with
[3H]-thymidine
(New England
Nuclear,
Boston) (I MCi per well)
over the last 16 to 20 hours. Cells were harvested
using a MASH
II
cell harvester
(MA Bioproducts,
Walkersville,
Md) in H2O and
counted
in a Packard
Scintillation
Spectrometer
(Packard
Instrument Co. Downers
Grove, Ill). Stimulation
index (SI) was determined by dividing the cpm incorporated
by cells stimulated
by SPA
plus BCGF or PHA-TCM
by the cpm incorporated
by cells stimulated by SPA alone.
Surface
membrane
analysis.
Pooled cells were washed
three
times in PBS with 2% bovine serum albumin
(BSA)
and 0.2%
sodium azide. Cells were suspended
in a-MEM
(2 x 106mL), and
0.05 mL of this cell suspension
was mixed with 0.05 mL of a 1:100
dilution
of munine monoclonal
antibody.
Antibodies
used included
OKT3,
OKT4,
and OKT8
(Orthoclone,
Ortho
Pharmaceutical
Corp, Raritan,
NI). The cell suspension
and monoclonal
antibody
were incubated
for 45 minutes in an ice bath. Cells were then washed
three times in cold a-MEM
and resuspended
in 0.1 mL cr-MEM.
To
this cell suspension
was added 0.025 mL of fluorescein
isothiocyanate (FITC)-labeled
goat antimouse
globulin (Cappel
Labs, Cochranville, Pa). This suspension
was incubated
for 45 minutes in an ice
bath. Cells were then washed three times in cold a-MEM,
resuspended in a minimal volume, and observed immediately
for immuno-
a,
fluorescence.
(HePFC)
Reverse
hemolytic
plaque
assay.
For the generation
of hemolytic plaque-forming
cells, 1 x 106 T cells and I x 106 B cells were
placed in 5 mL of a-MEM
and 10% FCS in 25-cm2 tissue culture
flasks (Costar,
Cambridge,
Mass) in 37 #{176}C
with 5% CO2 for four to
five days. Pokeweed
mitogen
(PWM)
(Sigma)
10 sg/mL
was
included during this culture period. A 0.025-mL
mixture of packed
SRBCs that had been complexed
to SPA was mixed with 0.8 mL of
0.5% agarose, 0.025 mL antisera
to human immunoglobulins
with i,
individuals
AND
WEISDORF
or “y heavy chain specificity
(Cappel
Labs), and 0.025
mL rabbit
complement
(Pelfreeze,
Rogers,
Ark) previously
absorbed
with
SRBCs.
To this, 0.1 mL of the four- to five-day-PWM-stimulated
cell suspension
was added, and 0.2 mL of the mixture was placed in a
Petni dish and covered. The dishes were incubated
for four hours at
37 #{176}C,
and the number
of cells secreting
specific immunoglobulins
was identified
by viewing the plates under an Olympus
(New Hyde
Park, NY) inverted
microscope
and identifying
a zone of lysis
around a single lymphocyte.
RESULTS
The
possibility
ulinemia
was
T cells was
white
blood
were normal.
decreased
5%,
with
ofOKT8
in Fig
patient’s
severe
presence
of increased
cells
suppressor
cells
(46%).
(24%)
Normal
and
values
for OKT4
by the patient’s
effect
T cells
of patient’s
was demonstrable.
T cells
and
B cell immunogbobulin
plaque
assay. Compared
cells ability
to form
T cells were mixed
production
with control,
plaques
in vitro (Fig
with control
B cells,
enhanced
T cell-mediated
suppressive
ID). These
findings
suggest
that this
gammagbobulinemia
does
not result
suppressive
effect
mediated
by her
intrinsic
B cell defect.
Assays
of B cell colony
dence against
the presence
Shown
on autobogous
B cells showed
a marked
impairment
in plaque
(Fig IA and B) (P < .01). The addition
ofcontrol
patient
B cells did not significantly
improve
the
and
in a reverse
the patient’s
formation
T cells to
patient’s
B
IC). When
no evidence
patient
of an
effect was noted (Fig
patient’s
severe
hypofrom
any increased
T cells,
but from
an
formation
provided
further
eviof an increased
T-cell
mediated
100
so
so
10
4#{176}
H
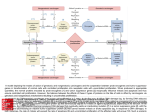
Fig
1.
In vitro
when
and
a
an increased
in our laboratory
are 51% ± 7% and 26% ±
Despite
the increased
number
of T cells
cell phenotype,
no evidence
of enhanced
I is the
albogeneic
hemolytic
hypogammagbob-
Both the patient’s
peripheral
and T cell (l,271/tL)
counts
peripheral
blood T cells showed
of OKT4
reactivity
respectively.
suppressor
suppression
this
to the
first examined.
cell (4,200/L)
The patient’s
number
number
OKT8
that
related
generation
autologous
the
D
patient
of
hemolytic
and allogeneic
with
CVH
plaque-forming
cells
T and B cells from
were
cultured
with
normal
poke-
weed mitogen
as described
in Materials
and Methods.
The following T cell and B cell combinations
were cultured:
(A) 1 x 10 T cells
and 1 x iO B cells from normal individuals;
(B) 1 x iO’ T cells and
I x iO B cells from the CVH patient;
(C) 1 x 10 T cells from
normal
individuals
and 1 x 1 0’ B cells from the CVH patient;
(D) 1 x 10’ T cells from the CVH patient
and 1 x 10 B cells from
normal
individuals.
Data represent
the mean ± SEM of triplicate
experiments.
From www.bloodjournal.org by guest on June 14, 2017. For personal use only.
IMPAIRED
RESPONSIVENESS
suppressive
this
was
effect
patient
markedly
formation
2A and
cells
did
and
BCGF
confirmed
± SEM,
5
.01). When
<
±
in the patient’s
2C). The addition
not
significantly
defect
present
this patient’s
in this
B cells
proliferation
was
assay.
347
an inherent
B cell defect
to
control
screening
B cell
the
nature
exposure
the
this patient’s
examined
next
concentrations,
impairment
to control
remained
lots ofcontrol
PHA-TCM,
capacity
B cells (SI
[vol/vol]
patient’s
B
consistent
PHA-TCM.
this patient’s
responsiveness
in
This
intrinsic
to BCGF.
B cells
to respond
(Fig 3). Over a wide
As
patient
a control
PHA-TCM
presence
alone
reagent
was
of SPA
(data
in the
prepared.
1% (vol/vol)
[P
<
.0 1 ] ). These
by this
so
or
compared
showed
suggest
impaired
a
B cell
[vol/
respecBCGF
T cells.
1
U
. so
so
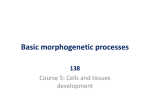
In vitro
B cells
from
generation
C
of B cell
0
colonies
when
normal
individuals;
(B)
T cells
and
CVH patient;
(C) T cells from normal
individuals
the CVH patient;
(D) T cells from the CVH patient
normal
individuals.
experiments.
evident
patient’s
guirre23
patients
presence
Data
represent
the
mean
±
char-
of stem
cells
into
synthesizing
and secreting
plasma
of their defective
immunogbobuof abnormalities
in B cell function,
study,
we
describe
another
by the lack
defect
disorder.
Our
in responsiveness
there appears
of formation
in B cell
patient’s
B cells
to the T cell
to be impaired
in B cell
proliferation
of B cell colonies
by this
B cells.
This
assay
originally
described
by Izaand adapted
by Penn
and Kay24 for the study
of
with
chronic
lymphocytic
leukemia
requires
the
of both irradiated
T cells and PHA-TCM
to support
B cell colony
that
not the
B cell
process,28
20
autologous
and allogeneic
T and B cells from normal
individuals
and the CVH
patient
were cultured
as described
in Materials
and Methods.
The
following
T cell and B cell combinations
were cultured:
(A) T cells
and
was
was
10
2.
in differentiation
production
of BCGF
in this patient.
The presence
of an intrinsic
defect
implied
40
Fig
In this
T cells suggested
were
hyporesponsive
B
of disorders
that results
from vanThese
patients
differ
T cell-B
cell interaction
and soluble
mediators
of B cell
function
have been implicated
as the cause of the impaired
B
cell differentiation
in various
subgroups
of patients
with
patient’s
70
A
group
normal
B cell colony formation.
The defect
in this patient’s
B
cell colony
formation
was not improved
by the addition
of
normal
albogeneic
T cells. The lack of improvement
of this
ao
.
block
function
in a patient
with this
display
a marked
impairment
lymphokine
BCGF.
In addition,
11
100
of the
CVH.
results
patient’s
site
mature
immunoglobulin
cells and in the pathogenesis
bin synthesis.
A diversity
B cell proliferation
assay,
Surprisingly,
on multiple
marked
impairment
in their ability
to support
control
proliferation
(SI 1.27 ± 0.21, 20% patient
PHA-TCM
vob] v 26 ± 1.4, 20% control
PHA-TCM
[vol/vol],
production
a heterogeneous
not shown).
occasions,
patient
PHA-TCM
preparations,
when
with control
PHA-TCM
preparations,
consistently
tively
represents
acterized
by hypogammaglobulinemia
ous defects
in cell immune
function.’
in the
a significant
with control
in the
10% (vol/vol)
20
(v/a)
DISCUSSION
to purified
BCGF
was
range of purified
BCGF
cant
15
OF SCGF
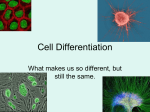
Fig 3.
SPA-stimulated
B cell proliferation
in the presence
of
varying concentrations
of BCGF. Cultures
(5 x 1 O B cells per well)
were incubated
for three days with the addition
of [3H]-thymidine
for the last 1 6 hours. Data represent
the mean ± SEM of triplicate
experiments.
Control
B cells.
-;
CVH patient
B cells, O---D.
CVH
with the same
concentrations
of BCGF
control
nor patient
B cells showed
signifi-
proliferation
S
10
S CONCENTRATION
suggested
B cells incubated
P < .01 ). Neither
BCGF
--
.3..
3
our
B cell defect
The ability
of
this patient’s
B cells showed
in proliferative
capacity
compared
(
.3- - - -
10
s
B cell
ability
of
in a B cell
in the proliferation
PHA-TCM
multiple
a
M
colony
of the
patient.
We first studied
to respond
to PHA-TCM
the possibility
that
included
an impaired
15
b
3,
define
impairment
control
25
20
2, v 93 ± 8, respectively)
(Fig
control
T cells were added,
no
of this patient’s
B cells compared
with control
I .3 ± 0.2 v 26 ± I .4, with 20% control
PHA-TCM
I P < .01 ]). The decreased
responsiveness
of this
cells
30
in
B cell colony
formation
with control
B cell colony
suppress
After
a marked
CVH
B cell colony
formation
was
of patient’s
T cells to control
B
formation
(Fig 2D).
We next sought
to further
there
IN
(Fig 2). The patient’s
impaired
compared
(mean
B) (P
enhancement
noted (Fig
TO
B cells
from
the
and B cells from
and B cells from
SEM of triplicate
formation
the
defective
T cell
apparent
evidently
receptors
for
help
has been
by activation
is required
the
by the patient’s
for the
T cell-derived
own
increased
T cells
expression
lymphokine
B cells
expressing
such
receptors,
second
signal,
BCGF,
can then
enter
when
and
BCGF.
exposed
maintain
of
Actito the
a prolifer-
state.
The inability
of control
PHA-TCM
tion in this patient’s
activated
B cells
this
of normal
shown
to be a multiple
step
of B cells. This activation
vated
ative
the addition
that this patient’s
B cells
proliferative
signal
and
defect.
proliferation
initiated
process
after
possibility
to BCGF’s
patient’s
B cells
are
BCGF.
This was confirmed
The results
described
here
intrinsically
to stimulate
proliferafurther
suggested
that
unable
to respond
by the use of purified
BCGF.
do not distinguish
BCGF
resis-
to
From www.bloodjournal.org by guest on June 14, 2017. For personal use only.
348
PERRI
tance due to diminished
receptors
or a postreceptor
It is now
known
state of activation
Tonsillar
B cells
simply
on the
cells
differ
and
the
Larger
BCGF
signal.
that
or absent
surface
membrane
proliferative
abnormality.
human
and thus
have been
basis
tonsillar
These
two
sensitivity
to the
proliferative
signal
B cells
differ
in vivo
their responsiveness
divided
into two
of size.
in their
second
B cells
could
directly
BCGF.
stimulated
by
to proliferate
without
requiring
an in vitro activation
The small tonsillar
B cells required
an initial
activa-
identified
that
activation
have
and
selective
effects
proliferation
that
on the processes
may
prove
as tools
for further
dissection
stages
of human
B cell activation,
of
useful
in the
in
and
differentiation.3#{176}
The
BCGF
decreased
responsiveness
of this
might be expected
to impair
clonal
subpopulations
patient’s
when
immune
challenged
defect
appears
with
patient’s
expansion
foreign
complicated
B cells to
of B cell
antigens.
by
another
clinically
involve,
by
described
recently
the
the
their
patient
in children
described
responsiveness
T
cell
to the
lymphokine
of BCGF
an enhanced
patient.
CVH
diverse
noted
in patients
with
group
impaired
differentiation
immunoglobulin
T cell
a clinical
of patients
capacity
who
have
for B cell
into mature
synthesis
with
Nezebors
in this
study
proliferation
BCGF
by the patient’s
suppressor
remains
WEISDORF
and
primary
immunodefiin defective
T cell function
of or responsiveness
to
disorder
in immune
regulation
and function
manifested
as CVH.
This patient’s
immune
first, an intrinsic
B cell defect
characterized
production
signal
and,
second,
T cells.
T cell
represents
that is
defects
by an
delivered
impaired
No evidence
of
effect
was noted
in this
syndrome
that includes
a
heterogeneous
proliferation
plasma
cells
and secretion.
causes
and
capable
for
terminal
of normal
This
ACKNOWLEDGMENT
impaired
BCGF
production
by her T cells as well. Abnormalities
production
of other
T cell lymphokines
(ie, interleukin
been
2 has been
deficiency.22
In summary,
impaired
from
to be
of B cell
abnormalities
proliferation,
2) have
systemic
lupus
erythematosus
ciency diseases.2”22
Heterogeneity
resulting
in decreased
production
interleukin
signal
by
tion signal
before
responding
to the proliferation
signal
BCGF.
Pharmacologic
agents
are now beginning
future
various
F.29
of B
activation
delivered
interleukin
in their
to BCG
subpopubations
subpopulations
initial
be
BCGF
AND
in
1,
We especially
thank Marti Dobson
assistance
throughout
this study.
for her excellent
technical
REFERENCES
Fudenberg
HH, Good RA, Goodman
HC, Hitzig W, Kunkel
HG, Roitt IM, Rosen FS, Rowe DS, Seligmann
M, Soothill
IR:
Primary
immunodeficiencies.
Bull WHO 45: 125, 1971
2. Siegal
FP, Siegal M, Good RA: Role of helper, suppressor
and
B-cell defects in the pathogenesis
of the hypogammaglobulinemias.
N EngI I Med 299:172,
1978
3. Morito
T, Bankhurst
AD, Williams
RC: Studies
of T- and
B-cell interactions
in adult patients with combined
immunodeficiency. I Clin Invest 65:422, 1980
4. Rosen ES, Cooper MD, Wedgwood
RIP: The primary
immunodeficiencies.
N EngI I Med 3 1 1 :300, 1984
5. Siegal
FP, Good
RA: Human
lymphocyte
differentiation
markers
and their application
to immune
deficiency
and lymphoproliferative
diseases. Clin Haematol
6:355, 1977
6. Wu LYF, Lawton AR, Greaves
MF, Cooper MD: Evaluation
of human
B lymphocyte
differentiation
using pokeweed
mitogen
(PWM)
stimulation:
In vitro studies in various antibody
deficiency
syndromes,
in F Daguillard
(ed): Proceedings
of the Seventh Leukocyte Culture
Conference.
Orlando,
Fla, Academic
Press, 1973, p
485
7. Mitsuya
H, Osaki K, Tomino
S. Katsuki
T, Kishimoto
5:
Pathophysiologic
analysis
of peripheral
blood lymphocytes
from
patients
with primary
immunodeficiency.
I. Ig synthesis
by peripheral blood lymphocytes
stimulated
with either pokeweed
mitogen or
Epstein-Barr
virus in vitro. I Immunol
127:31 1, 1981
8. Waldmann
TA, Broder 5, Blaese RM, Durm M, Blackman
M,
Strober
W: Role of suppressor
T cells in pathogenesis
of common
variable hypogammagbobulinaemia.
Lancet 2:609, 1974
9. Siegal FP, Siegal M, Good RA: Suppression
of B cell differentiation by leukocytes
from hypogammaglobulinemic
patients.
J Clin
Invest 58:109, 1976
10. Broom BC, de Ia Concha
EG, Webster
ADB, ianossy
GI,
Asherson
GL: Intracellular
immunoglobulin
production
in vitro by
lymphocytes
from patients with hypogammaglobulinemia
and their
effect on normal lymphocytes.
Clin Exp Immunol
23:73, 1976
1 1 . Pyke KW, Dosch
H-M, lpp MM, Gelfand GW: DemonstraI.
tion of an intrathymic
defect in a case of severe combined
immunodeficiency
disease. N EngI I Med 293:424,
1975
12. Waldmann
TA, Broder 5, Krakauer
R, MacDermott
RP,
Durm M, Goldman
C, Meade B: The role of suppressor
cells in the
pathogenesis
of common
variable
hypogammaglobulinemia
and the
immunodeficiency
associated
with myeboma.
Fed Proc 35:2067,
I 976
I 3. Geha
RS, Schneeberger
EE, Rosen FS, Merler E: Heterogeneity of “acquired”
or common
variable
hypogammaglobulinemia. N EnglI Med 291:1,
1974
14. Stevens
RH, Tamaroff
M, Saxon A: Inability of patients with
common variable hypogammaglobulinemia
to generate
lymphoblastoid B-cells following
booster immunization.
Clin Immunol
Immunopathol
16:336, 1980
I 5. de Ia Concha
EG, Oldham
G, Webster
DB, Asherson
GL,
Platts-Mills
TAE: Quantitative
measures
of T and B cell function in
variable
primary
hypogammaglobulinemia:
Evidence
for a consistent B-cell defect. Clin Exp Immunol
27:208, 1976
16. Denis KA, Wall R, Saxon A: Human-human
B cell hybridomas from in vitro stimulated
lymphocytes
of patients
with common
variable immunodeficiency.
I Immunol
131:2273,
1983
17.
Howard
M, Paul WE: Regulation
of B-cell growth
and
differentiation
by soluble factors, in Metzger
H, Fathman
CG, Paul
WE (eds): Annual Review of Immunology.
Palo Alto, Calif. Annual
Reviews Inc, 1983, p 307
18. Yoshizaki
K, Nakagawa
T, Fukunaga
K, Kaieda
T,
Maruyama
5, Kishimoto
5, Yamamura
Y, Kishimoto
T: Characterization of human B cell growth factor (BCGF)
from cloned T cells or
mitogen-stimulated
Tcells. I Immunol
130:1241,
1983
I 9. Butler I, Muraguchi
A, Lane C, Fauci AS: Development
of a
human T-T cell hybridoma
secreting
B cell growth factor. I Exp
Med 157:60,
1983
20.
Elkins K, Cambier
IC: Constitutive
production
of a factor
supporting
B lymphocyte
differentiation
by a T cell hybridoma.
I
Immunol
130:1247,
1983
21.
Linker-Israeli
M, Bakke AC, Kitridou
RC, Gendler 5, Gillis
From www.bloodjournal.org by guest on June 14, 2017. For personal use only.
IMPAIRED
RESPONSIVENESS
TO
BCGF
IN
CVH
5, Horwitz
DA: Defective
production
of interleukin
1 and interleukin 2 in patients
with systemic
lupus erythematosus
(SLE).
I
Immunol
130:2651,
1983
22.
Flomenberg
N, Welte K, Mertelsmann
R, Kernan
N, Ciobanu N, Venuta S, Feldman
5, Kruger 5, Kirkpatrick
D, Dupont B,
O’Reilly
R: Immunologic
effects of interleukin
2 in primary
immunodeficiency
diseases. I Immunol
130:2644,
1983
23.
Izaguirre
CA, Minden MD, Howatson
AF, McCulIoch
EA:
Colony formation
by normal and malignant
human B lymphocytes.
Br I Cancer 42:430, I 980
24.
Perri RT, Kay NE: Monoclonal
CLL B-cells may be induced
to grow in an in vitro B-cell colony assay system.
Blood 59:247,
I 982
25.
Ford RS, Mehto SR. Franzini
D, Montagna
RA, Lachman
LB. Maizel AL: Soluble factor activation
of human B lymphocytes.
Nature 294:261,
1981
26.
Maizel
AL, Sahasrabuddhe
CG, Mehta
SR. Morgan
I,
349
Lachman
LB, Ford RI: Biochemical
separation
of a human B cell
mitogenic
factor. Proc NatI Acad Sci USA 79:5998,
1982
27.
Maizel
AL, Morgan
I, Mehta
SR, Kouttab
N, Bator I,
Sahasrabudde
CG: Long-term
growth of human B cells and their use
in a microassay
for B-cell growth factor. Proc NatI Acad Sci USA
80:5047,
1983
28. Falkoff RIM, Zhu LP, Fauci AS: Separate
signals for human
B cell proliferation
and differentiation
in response to Staphylococcus aureus:
Evidence
for a two-signal
model of B cell activation.
I
Immunol
129:97, 1982
29. Muraguchi
A, Butler IL, Kehrl IH, Fauci AS: Differential
sensitivity
of human B cell subsets to activation
signals delivered
by
anti-si antibody and proliferative
signals delivered
by a monoclonal
B
cell growth factor. I Exp Med 157:530,
1983
30. Muraguchi
A, Butler JL, Kehrl IH, Falkoff RIM, Fauci AS:
Selective
suppression
of an early step in human B cell activation
by
cycbosporin
A. I Exp Med 158:690, 1983
From www.bloodjournal.org by guest on June 14, 2017. For personal use only.
1985 66: 345-349
Impaired responsiveness to B cell growth factor in a patient with common
variable hypogammaglobulinemia
RT Perri and DJ Weisdorf
Updated information and services can be found at:
http://www.bloodjournal.org/content/66/2/345.full.html
Articles on similar topics can be found in the following Blood collections
Information about reproducing this article in parts or in its entirety may be found online at:
http://www.bloodjournal.org/site/misc/rights.xhtml#repub_requests
Information about ordering reprints may be found online at:
http://www.bloodjournal.org/site/misc/rights.xhtml#reprints
Information about subscriptions and ASH membership may be found online at:
http://www.bloodjournal.org/site/subscriptions/index.xhtml
Blood (print ISSN 0006-4971, online ISSN 1528-0020), is published weekly by the American Society of
Hematology, 2021 L St, NW, Suite 900, Washington DC 20036.
Copyright 2011 by The American Society of Hematology; all rights reserved.