Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Adherence (medicine) wikipedia , lookup
Discovery and development of angiotensin receptor blockers wikipedia , lookup
Clinical trial wikipedia , lookup
Discovery and development of antiandrogens wikipedia , lookup
5-HT3 antagonist wikipedia , lookup
Discovery and development of beta-blockers wikipedia , lookup
Environmental impact of pharmaceuticals and personal care products wikipedia , lookup
Psychedelic therapy wikipedia , lookup
Polysubstance dependence wikipedia , lookup
Cannabinoid receptor antagonist wikipedia , lookup
Prescription costs wikipedia , lookup
Drug discovery wikipedia , lookup
Pharmaceutical industry wikipedia , lookup
Pharmacokinetics wikipedia , lookup
Neuropharmacology wikipedia , lookup
Psychopharmacology wikipedia , lookup
Pharmacognosy wikipedia , lookup
Neuropsychopharmacology wikipedia , lookup
NK1 receptor antagonist wikipedia , lookup
Drug interaction wikipedia , lookup
Pharmacogenomics wikipedia , lookup
Theralizumab wikipedia , lookup
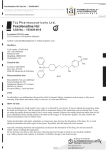
PROCEEDINGS THE CONCEPT OF THE THERAPEUTIC WINDOW IN THE CHOICE OF H1-RECEPTOR ANTAGONIST* — Peter H. Howarth, DM, FRCP† ABSTRACT Antihistamines have existed for more than 60 years. The first-generation antihistamines provided symptom relief from allergic rhinitis but were also associated with undesired side effects due to lack of receptor selectivity and central nervous system penetration. Since then, newer-generation antihistamines have been specifically developed to reduce the occurrence of side effects while still providing efficacy. Differences of cardiotoxicity and sedation still exist, however, among available antihistamines. The choice of available antihistamines, therefore, is best informed through evaluation of the therapeutic window of each medication—ie, the dose range over which a drug is efficacious while being free from side effects. A broad therapeutic window conveys the most ideal characteristics. The therapeutic window provides considerably more information for clinical considerations than standard individual terms, such as potency, efficacy, or safety, combining these characteristics into an easily attainable understanding of the agent. This paper describes the importance of conscientious choices of antihistamines through the use of a therapeutic window based on recent research. Understanding the therapeutic windows of these agents will enable physicians to make informed treatment decisions based on the requirements of the patient and characteristics of the antihistamine. (Adv Stud Med. 2004;4(7A):S508-S512) *Based on a presentation given by Prof Howarth at the 2003 World Allergy Organization Congress. †Reader in Medicine and Honorary Consultant Physician, Respiratory Cell and Molecular Biology, Southampton General Hospital, Southampton, United Kingdom. Address correspondence to: Peter H. Howarth, DM, FRCP, Respiratory Cell and Molecular Biology, Mail point 810, Southampton General Hospital, Tremona Road, Southampton, UK SO16 6YD. E-mail: [email protected]. S508 ore than 6 decades have passed since the first antihistamines were developed and used to treat allergic disease. These initial H1-receptor antagonists, although effective in the treatment of urticaria and rhinitis, were shown to cause undesired side effects, such as sedation, due to central nervous system (CNS) penetration. They also were shown to cause a range of other effects due to lack of receptor specificity. In the late 1970s and early 1980s, second-generation antihistamines, such as terfenadine, cetirizine, and loratadine, were developed to improve receptor specificity and reduce the sedative properties. Additional antihistamines, such as fexofenadine, intranasal levocabastine, and intranasal azelastine, were also developed to further improve the safety profile. Other H1 antihistamines have also been developed, including mizolastine, desloratadine, and levocetirizine. Despite the range of antihistamines available, sedation and cardiotoxicity remain as potential undesirable side effects of some presently prescribed drugs. Given the wide range of H1 antihistamines, physicians must assess these deleterious effects as well as the efficacy of the specific therapy to make an educated choice regarding medication. This choice is best informed through evaluation of the therapeutic window for each medication. M THERAPEUTIC WINDOW The therapeutic window of an H1-receptor antagonist is the dose range over which it is efficacious and also free from unwanted side effects (Figure 1). The positioning of the clinically recommended dose (range) within this window provides an easy understanding of the impact of the interactions that decrease or increase therapeutic bioavailability as well as the impact of dose adjustments on both safety and efficacy. The lower limit of the therapeutic window is set by the lowest clinically effective dose for the disease condition under considera- Vol. 4 (7A) ■ July 2004 PROCEEDINGS tion. By contrast, the upper limit is set by the highest dose tolerated without adverse pharmacologic effect. The therapeutic window will differ between intranasal (topical) and oral (systemic) drug administration. The issues discussed in this paper will focus on those pertaining to oral H1-antihistamine administration. Within any given therapeutic window for H1 antihistamines, a range of factors may influence the positioning of any dose, such as coadministration of food, concomitant drug therapy (eg, macrolide antibiotics), concurrent illness (eg, hepatic/renal disease), and pharmacologic interactions (eg, alcohol). For example, fexofenadine, which is licensed for the treatment of allergic rhinitis and urticaria, is an H1 antihistamine with a very broad therapeutic window. It is clinically effective in a total daily dose as low as 40 mg,1,2 which is one third of the clinically recommended dose. Moreover, it is free from adverse CNS effects when assessed objectively at 3 times the standard therapeutic dose (360 mg daily),3 and it is free from subjective reporting of sedation at 690 mg twice daily, a dose almost 12 times the recommended daily dose.1 By contrast, the H1 antihistamine loratadine has a very narrow therapeutic window, with the clinically recommended dose of 10 mg appearing to be both the minimally effective dose and the maximum tolerated dose.4,5 Whereas interactions or dose adjustments are highly unlikely to influence the efficacy or safety of fexofenadine, they are likely to have an effect with respect to loratadine. H1-ANTIHISTAMINE ACTIVITY The standard H1-antihistamine doses selected for clinical evaluation are assessed both in the acute challenge situation to provide information on time to onset of action, maximum inhibitory effect, and duration of action and in naturally occurring clinical disease, which has greater intrinsic variability and is less rigorously controlled than the challenge studies. These challenge and “wild-disease” studies identify the H1-receptor antagonistic activity of all currently available H1 antihistamines compared with placebo.6 This antagonistic activity, however, is least evident with loratadine,7 as one might anticipate when understanding the positioning of the clinically recommended dose within the therapeutic window. The receptor antagonistic activity of different H1-receptor antagonists can be assessed by their suppression of histamine-induced wheal and flare, a commonly used biologic assay for demonstrating the onset and duration of peripheral H1-receptor blockade.8,9 This Advanced Studies in Medicine ■ pharmacodynamic evaluation model is easily reproduced, allows objective assessments to be made in both healthy volunteers and patients, and is useful as an addition to clinical studies. WHEAL AND FLARE Wheal and flare studies have been widely used to indicate in vivo differences in the potential efficacy of secondgeneration antihistamines.8-11 Frossard et al recently compared the inhibition of histamine-induced wheal and flare by fexofenadine HCl 180 mg, loratadine 10 mg, and desloratadine 5 mg in a single-dose, randomized, parallelgroup, double-blind, placebo-controlled study of healthy individuals.11 This study found that total inhibition of wheal, as defined by the time required to achieve 95% inhibition of wheal area, occurred between 3 and 3.5 hours following administration of fexofenadine. In contrast, total inhibition of wheal was not observed following treatment with either loratadine or desloratadine at the standard doses. These results are further corroborated in the study by Kaliner et al.12 In this randomized, doubleblind, single-dose, placebo-controlled, cross- over study, it was observed that fexofenadine HCl 180 mg was significantly more effective than loratadine 10 mg (P < .001) or placebo (P < .05) at suppressing the flare response. Fexofenadine wheal suppression was also significant relative to that of loratadine (P < .05) or placebo (P < .05). In a similar study, Purohit et al compared the inhibition of histamine-induced wheal and flare by single therapeutic doses of fexofenadine HCl 180 mg and cetirizine 10 mg in a single-center, double-blind, randomized, 2-way crossover study.13 The findings showed that fexofenadine Figure 1.Therapeutic Window *The dose range over which a treatment is both effective and free from unwanted side effects. S509 PROCEEDINGS and cetirizine are comparable in their time to occurrence of 95% inhibition of the wheal and flare reaction to histamine. CLINICAL STUDIES Although the histamine-induced wheal and flare reaction is a useful clinical pharmacologic test to assess dose-response relations for an antihistamine, thereby providing an indication of its efficacy, data from clinical studies are necessary to properly evaluate new agents. All H1 antihistamines have been shown in placebo-controlled studies to be clinically efficacious.6 Studies comparing different H1 antihistamines allow evaluation of both clinical efficacy and safety, and permit investigation of the comparability of their profiles. The efficacy and safety of once-daily fexofenadine 120 mg and 180 mg and cetirizine 10 mg in the treatment of seasonal allergic rhinitis (SAR) were compared in a multicenter, doubleblind, randomized, parallel-group, placebo-controlled, 14-day trial.14 A total symptom score (TSS) was generated as the sum of scores for the following symptoms: sneezing, rhinorrhea, itchy nose/palate/throat, and itchy/watery/red eyes. The findings revealed no significant differences in treatment efficacy between fexofenadine at either dose or cetirizine; however, cetirizine was found to substantially induce fatigue and drowsiness, in contrast to the results obtained with fexofenadine. In a similar study, fexofenadine 180 mg and cetirizine 10 mg demonstrated statistically and clinically equivalent efficacy throughout the dosing period, based on TSS in patients with moderate-to-severe SAR. This study also assessed drowsiness using a visual analog scale (VAS) by which scores were calculated based on a range from 0 (wide awake) to 100 (extremely sleepy). Differences in VAS change from baseline between treatments were observed; patients receiving fexofenadine consistently reported less drowsiness than those receiving cetirizine.15 In a multicenter, multinational, double-blind, parallel-group, randomized, placebo-controlled 2-week study, van Cauwenberge et al assessed the efficacy, safety, and impact on quality of life (QOL) of once-daily fexofenadine HCl 120 mg, loratadine 10 mg, or placebo in the treatment of SAR.16 Fexofenadine and loratadine were significantly superior to placebo in reducing instantaneous TSS (P ≤ .0001 and P ≤ .005, respectively) and individual 24-hour reflective symptom scores for sneezing, rhinorrhea, itchy nose/palate/throat, and itchy/ watery/red eyes (P ≤ .005 and P < .05, respectively; Figure 2). In addition, fexofenadine was significantly S510 superior to loratadine at improving nasal congestion and itchy/watery/red eyes (P ≤ .05). All treatment groups had significantly improved overall QOL from baseline (P < .0001); however, the improvement in the fexofenadine group was significantly greater compared with the loratadine (P ≤ .03) and placebo groups (P ≤ .005). This difference between fexofenadine and loratadine may be explained by their antagonist profile. Receptor antagonists may be neutral antagonists or inverse agonists. Neutral antagonists inhibit the action of the relevant agonist but have no other intrinsic activity. Inverse agonists, while inhibiting the action of the agonist, also have additional activity independent of this property through receptor binding. This binding alters the agonist-independent G-protein coupling of the receptor, which contributes to the basal level of cell activation. Inverse agonists will thus have a broader profile of effect than pure neutral antagonists.17 Studies that we have undertaken with fexofenadine in vitro indicate that it acts as an inverse agonist in that it not only inhibits tumor necrosis factor alpha–induced interleukin (IL)-8 release from epithelial cells, but also reduces the level of IL-8 in the supernatant to below the unstimulated value. The additional activity of fexofenadine over loratadine on QOL and in relieving nasal obstruction in the study by van Cauwenberge et al could be explained by its ability to act as an inverse agonist.16 DRUG-DRUG INTERACTIONS The coadministration of other drugs or pharmacologically active agents may potentially modify the positioning of an H1 antihistamine within the therapeutic window by, for example, interfering with absorption or metabolism. Such changes may either reduce clinical efficacy or increase the risk of side effects. These possible consequences became most apparent when drug interactions led to the appreciation that astemizole and terfenadine had potentially serious cardiac effects due to their inhibitory actions on the potassium rectifier currents within the myocardium.18 Both astemizole and terfenadine undergo hepatic metabolism involving the cytochrome P450 isoenzymes. The coadministration of macrolide antibiotics, such as erythromycin, or antifungal agents, such as ketoconazole, which share the same P450 isozymes, led to the inhibition of their metabolism and a rise in their plasma levels. This interaction took these drugs out of their therapeutic window, with the potentially fatal, although very rare, consequence of the Vol. 4 (7A) ■ July 2004 PROCEEDINGS Figure 2. Placebo-Controlled Comparison of Fexofenadine and Loratadine in Seasonal Allergic Rhinitis Adapted with permission from van Cauwenberge et al. Comparison of the efficacy, safety, and quality of life provided by fexofenadine hydrochloride 120 mg, loratadine 10 mg, and placebo administered once daily for the treatment of seasonal allergic rhinitis. Clin Exp Allergy. 2000;30(6):891899.16 Blackwell Publishing. ventricular arrhythmia, torsade de pointes. H1 antihistamines that do not undergo hepatic metabolism, such as fexofenadine and cetirizine, are thus free from these cytochrome P450 interactions. Interest has more recently focused on the relevance of pharmacologic interactions involving the superfamily of adenosine triphosphate-binding cassette proteins, such as P-glycoprotein (Pgp) and other carrier protein families, including the organic anion transporting peptide (OATP) family.19 Pgp is an important transport protein regulating clearance of molecules that penetrate the blood-brain barrier. Substrates for this carrier protein are rapidly cleared from the CNS and thus are not available to act on central receptors. Fexofenadine is an excellent Pgp substrate; this property makes it a safe H1 antihistamine regarding CNS sedative effects (see review by Prof Hindmarch for details of CNS effects of H1 antihistamines).20 Pgp is also involved in eliminating drugs across the gastrointestinal mucosa. At this site, ketoconazole and macrolide antibiotics are known to inhibit Pgp, reducing the gastrointestinal elimination of H1 antihistamines that use this transport mechanism. For example, ketoconazole increases the plasma levels of desloratadine, and azithromycin increases the plasma levels of both desloratadine and fexofenadine.21,22 By contrast, the OATP family helps facilitate the gastrointestinal absorption of certain H1 antihistamines. This transport process is susceptible to inhibition by grapefruit juice.23,24 Studies in a small number of healthy volunteers have reported a Advanced Studies in Medicine ■ decrease in the plasma levels of fexofenadine when taken with large quantities (1.2 L) of double-strength grapefruit juice.24 This reduction is, however, only about 30% and, due to the minimally effective dose being substantially lower than the effects of this reduction, there is no clinical consequence. Individuals would be unlikely to consume quantities of grapefruit juice large enough to effect this level of reduction. Consistent with the lack of clinical significance of this interaction, data from White et al demonstrated that fexofenadine significantly inhibits the histamine wheal and flare response within the skin when oral fexofenadine is coadministered with either grapefruit juice or orange juice.25,26 Changes in the positioning of H1 antihistamines within a narrow therapeutic window will, however, lead to clinical consequences. The significance of the 40% increase in plasma levels of desloratadine when coadministered with ketoconazole is undetermined, as much less is known about the therapeutic window of this antihistamine. It is appreciated, however, that increasing the dose of drugs that have a therapeutic dose at the top end of their therapeutic window, such as cetirizine and loratadine, can lead to central effects, such as sedation and cognitive impairment.5 These effects could become an issue in situations in which patients overmedicate beyond the prescribed dose due to inadequate symptom control of either rhinitis or urticaria. GENETIC INFLUENCES Variations in the population and among different racial populations, in terms of the metabolism of antihistamines, may theoretically alter the position of a certain drug within its known therapeutic window. Little is known about how this variable influences either the efficacy or the side-effect profile of the currently available H1-receptor antagonists. Any impact of metabolic alterations will, as for the other considerations, be more relevant to those drugs with a narrow therapeutic window, those that are administered either at the lower or upper end of this range, and those for which small alterations can take them outside their therapeutic window. The product insert for desloratadine indicates that certain populations of patients are thought to be slow metabolizers of this agent. Approximately 7% of the general population and 20% of the black population have difficulty in converting desloratadine to its active metabolite, 3-hydroxydesloratadine, and may be more susceptible to dose-related adverse events.27 Additional investigation of S511 PROCEEDINGS this issue is warranted to understand differences in individual susceptibility within the population and to better inform physicians regarding choice of antihistamine. CONCLUSION The appreciation of the therapeutic window for any antihistamine and the positioning of the medication within this window allow an easy evaluation of the likely impact of any dose changes or interactions that will either decrease or increase the bioavailability of that medication. Ideally, an antihistamine should be positioned centrally within a broad therapeutic window. Under such circumstances, those influences that alter bioavailability are unlikely to have any clinical consequence, and the drug can be prescribed without concern. REFERENCES 1. Russell T, Stoltz M, Weir S. Pharmacokinetics, pharmacodynamics, and tolerance of single- and multiple-dose fexofenadine hydrochloride in healthy male volunteers. Clin Pharmacol Ther. 1998;64(6):612-621. 2. Bronsky EA, Falliers CJ, Kaiser HB, Ahlbrandt R, Mason JM. Effectiveness and safety of fexofenadine, a new nonsedating H1-receptor antagonist, in the treatment of fall allergies. Allergy Asthma Proc. 1998;19(3):135-141. 3. Hindmarch I, Shamsi Z, Kimber S. An evaluation of the effects of high-dose fexofenadine on the central nervous system: a double-blind, placebo-controlled study in healthy volunteers. Clin Exp Allergy. 2002;32(1):133-139. 4. Hansen GR. Loratadine in the high performance aerospace environment. Aviat Space Environ Med. 1999;70(9):919-924. 5. Hindmarch I, Shamsi Z. Antihistamines: models to assess sedative properties, assessment of sedation, safety and other sideeffects. Clin Exp Allergy. 1999;29(suppl 3):133-142. 6. Howarth PH. H1-receptor antagonists in the rhinoconjunctivitis. In: Simons FER, ed. Histamine and H1-Receptor Antagonists in the Treatment of Allergic Disease. New York: Marcel Deker Inc; 2002:215-250. 7. Meltzer EO, Malmstrom K, Lu S, et al. Concomitant montelukast and loratadine as treatment for seasonal allergic rhinitis: a randomized, placebo-controlled clinical trial. J Allergy Clin Immunol. 2000;105(5):917-922. 8. Simons FE, McMillan JL, Simons KJ. A double-blind, singledose, crossover comparison of cetirizine, terfenadine, loratadine, astemizole, and chlorpheniramine versus placebo: suppressive effects on histamine-induced wheals and flares during 24 hours in normal subjects. J Allergy Clin Immunol. 1990;86(4, pt 1):540-547. 9. Rivest J, Despontin K, Ghys L, Rihoux JP, Lachapelle JM. Pharmacological modulation by cetirizine and ebastine of the cutaneous reactivity to histamine. Dermatologica. 1991;183(3):208-211. 10. Grant JA, Riethuisen JM, Moulaert B, DeVos C. A doubleblind, randomized, single-dose, crossover comparison of levocetirizine with ebastine, fexofenadine, loratadine, mizolastine, and placebo: suppression of histamine-induced whealand-flare response during 24 hours in healthy male subjects. Ann Allergy Asthma Immunol. 2002;88(2):190-197. S512 11. Frossard N, Purohit A, Kovacs S, Vitow C, Georges G, Pauli G. Fexofenadine is superior to loratadine and desloratadine in onset of action of histamine-induced wheal and flare inhibition. Ann Allergy Asthma Immunol. 2003;90:124. 12. Kaliner MA, White MV, Economides A, et al. Relative potency of fexofenadine HCl 180 mg, loratadine 10 mg, and placebo using a skin test model of wheal-and-flare suppression. Ann Allergy Asthma Immunol. 2003;90(6):629-634. 13. Purohit A, Deslandes B, Pauli G, Frossard N. Fexofenadine and cetirizine have similar rapid onset of action and magnitude of effect as assessed by inhibition of histamine-induced wheal and flare. Ann Allergy Asthma Immunol. 2003; 90:123. 14. Howarth PH, Stern MA, Roi L, Reynolds R, Bousquet J. Double-blind, placebo-controlled study comparing the efficacy and safety of fexofenadine hydrochloride (120 mg and 180 mg once daily) and cetirizine in seasonal allergic rhinitis. J Allergy Clin Immunol. 1999;104(5):927-933. 15. Hampel F, Ratner P, Mansfield L, Meeves S, Liao Y, Georges G. Fexofenadine HCl 180 mg exhibits equivalent efficacy to cetirizine, 10 mg, with less drowsiness in patients with moderate-to-severe seasonal allergic rhinitis. Ann Allergy Asthma Immunol. 2003;91(4):354-361. 16. van Cauwenberge P, Juniper E. Comparison of the efficacy, safety and quality of life provided by fexofenadine hydrochloride 120mg, loratadine 10mg and placebo administered once daily for the treatment of seasonal allergic rhinitis. Clin Exp Allergy. 2000;30(6):891-899. 17. Leurs R, Church MK, Taglialatela M. H1-antihistamines: inverse agonism, anti-inflammatory actions and cardiac effects. Clin Exp Allergy. 2002;32(4):489-498. 18. Hibbert J, Howarth PH. Antihistamines and cardiac arrhythmias. Prescribers J. 1994;34:31-35. 19. Hansten PD, Levy RH. Role of P-glycoprotein and organic anion transporting polypeptides in drug absorption and distribution: focus on H1-receptor antagonists. Clin Drug Invest. 2001;21:587-596. 20. Cvetkovic M, Leake B, Fromm MF, Wilkinson GR, Kim RB. OATP and P-glycoprotein transporters mediate the cellular uptake and excretion of fexofenadine. Drug Metab Dispos. 1999;27(8):866-871. 21. Hwang KK, Correll M, Offord SJ. Evaluation of desloratadine for absorption drug-drug interactions with ketoconazole. J Allergy Clin Immunol. 2001;107:153. 22. Gupta S, Banfield C, Kantesaria B, et al. Pharmacokinetic and safety profile of desloratadine and fexofenadine when coadministered with azithromycin: a randomized, placebo-controlled, parallel-group study. Clin Ther. 2001;23(3):451-466. 23. Dresser GK, Bailey DG, Leake BF, et al. Fruit juices inhibit organic anion transporting polypeptide-mediated drug uptake to decrease the oral availability of fexofenadine. Clin Pharmacol Ther. 2002;71(1):11-20. 24. Banfield C, Gupta S, Marino M, Affrime M. Grapefruit juice reduces the oral bioavailability of fexofenadine but not desloratadine. Clin Pharmacokinet. 2002;41(4):311-318. 25. White MV, Kaliner MA, Rothrock S, et al. Effect of grapefruit juice on fexofenadine vs placebo in a skin wheal-andflare challenge model. Presented at: the 22nd European Academy of Allergology and Immunology Congress; June 7-10, 2003; Paris, France. 26. White MV, Kaliner MA, Rothrock S, et al. Effect of orange juice on fexofenadine vs placebo in a skin wheal-and-flare challenge model. Presented at: the 22nd European Academy of Allergology and Immunology Congress; June 7-10, 2003; Paris, France. 27. Clarinex [package insert]. Kenilworth, NJ: Schering Corporation; 2000. Available at: http://www.spfiles. com/piclarinex.pdf. Accessed November 10, 2003. Vol. 4 (7A) ■ July 2004