Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Inflammation wikipedia , lookup
Atherosclerosis wikipedia , lookup
Molecular mimicry wikipedia , lookup
Adoptive cell transfer wikipedia , lookup
Pathophysiology of multiple sclerosis wikipedia , lookup
Adaptive immune system wikipedia , lookup
Monoclonal antibody wikipedia , lookup
Immune system wikipedia , lookup
Complement system wikipedia , lookup
Hygiene hypothesis wikipedia , lookup
Polyclonal B cell response wikipedia , lookup
Cancer immunotherapy wikipedia , lookup
Immunosuppressive drug wikipedia , lookup
Psychoneuroimmunology wikipedia , lookup
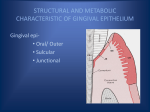
Pre-clinical Periodontics Defense mechanisms of the periodontium Dr Jamal Naim PhD in Orthodontics Initiation of periodontal disease Microorganisms which form the dental biofilm contain or release components which induce gingivitis. The inflammatory changes may remain confined to the gingival area for several years but at some sites gingivitis eventually shifts to destructive periodontal disease. Why lesions remain localized to the marginal portion of the gingival tissues, while in others they progress to involve the loss of connective tissue attachment and supporting alveolar bone? Imbalance of the host-microbial relationship is occurring in the destructive lesions! Normal gingiva vs. clinical healthy gingiva Pink color, firm consistency and scalloped outline for gingival margin. The interdental papillae are firm, do not bleed on gentle probing and fill the space below the contact areas. Can only be established experimentally after supervised meticulous daily plaque control for several weeks. Normal gingiva vs. clinical healthy gingiva the gingivae we would routinely classify as "clinically healthy gingivae" are not as histological perfect as the "normal gingivae“ Clinically healthy gingivae would be typically that level of health which could be attained by patients regularly practicing a good standard of plaque control. The oral surface of clinically healthy gingiva consists of keratinized oral epithelium continuous with the JE. Below the JE is a vascular network which supplies the epithelium with nutrients and defense cells. Neutrophils and macrophages can be seen in the junctional epithelium of the clinically healthy gingiva Defence mechanisms of the periodontium Clinically the gingival tissue is able to deal with external challenges without progressing to a diseased state, probably due to several defensive factors: Host defense processes Host-parasite reactions can be divided into: Innate (non-specific) response include the inflammatory response Adaptive (specific) response include immunological responses Innate (non-specific) response Innate immune mechanisms operate without any previous contact with the disease-causing microorganism. These mechanisms include: the physical barriers of the oral mucosal epithelial surfaces and vascular and cellular aspects of the inflammatory responses. Innate (non-specific) response Regular shedding of epithelial cells into the oral cavity Positive fluid flow of the gingival crevice (GCF) which may remove non-attached microorganisms and noxious products Antimicrobial effect of antibodies Phagocytic function of neutrophils and macrophages Detrimental effect of complements on microbes Innate (non-specific) response 1. Gingival epithelial cells may form the first barriers of defense against oral bacteria in periodontal tissues. (KE) 2. Prevention of attachment and colonization: 1. 2. the washing effect of the saliva and gingival crevicular fluid (GCF), the constituents of these fluids (antibodies, proteases, complement and lactoferrin) can be bactericidal. 3 types of gingival epithelium 1. Turnover time of JE JE has a high turnover (5 days) compared to oral gingival epithelium (8-10 days) The shedding rate is very high for JE 50-100 > than OGE. JE-cells that are degenerating and covered by bacteria and or their products are expelled at a fast rate This also may explain why gingivitis can be a reversible condition, which is considered a defensive mechanism of this tissue` Tooth surface JE has a rapid turnover rate JE cells at the base of the Sulcus are covered by microbes and constantly shed into the Sulcus. Replacement rate of the JE is 5 days (vs 8-10 days for oral gingival epithelium) JE has impressive antimicrobial systems Enzyme-rich lysosomes (packages of enzymes in the JE cytoplasm) e. g. Defensins Tooth surface 3. JE behaves like a semipermeable membrane Small molecules injected intravenously can be detected in sulcus after 1-5 minutes. Large molecules (eg immunoglobins) take 30-120 minutes to get into sulcus. blood vessels in gingiva 3. JE behaves like a semipermeable membrane Bacteria in the sulcus release large quantities of metabolites which diffuse through the JE: Butyric & propionic acids (toxic to tissues) Peptides Lipopolysaccharides (LPS) Bacteria 4. JE is part of the immune system JE has a sensory function detecting chemical excreted from the bacteria HELP!!!!! we’re under attack Bacteria 4. JE is part of the immune system JE produces cytokines (IL8) which recruit PMN from underlying blood vessels in connective tissue, through JE and out into sulcus blood vessels in gingiva Bacteria 4. JE is part of the immune system JE produces other cytokines which switch on the inflammatory response in the gingiva. blood vessels in gingiva 5. Neutrophils (PMN) Different names for the same cell • Polymorphonuclear leucocytes • Polymorphs • PMN • Neutrophils PMN = primary periodontal defensive cell Produced in the bone marrow from stem cells; live for about 4-5 days. PMN have a rapid turnover rate. Engulf microbes in sulcus (phagocytosis). Digest microbes by powerful enzymes contained in cytoplasm. PMN = primary periodontal defensive cell May blow up in the gingival tissues, releasing destructive enzymes and pro-inflammatory mediators which exacerbates the inflammatory response. Biofilm Tooth surface PMN form a dense layer (pallisade) over plaque & engulf bacteria in sulcus Bacterial product stimulates JE cells to produce concentration gradient of chemoattractant (IL-8) for PMN. blood vessels in gingiva Transendothelial migration Defects of the PMN function can reduce host defense capability. PMN function may be blocked at various sites: Chemotactic defects Inadequate adherence Defective phagocytosis Impaired ability to digest Transendothelial migration Systemic diseases characterized by granulocyte defects are usually accompanied by severe periodontal disease (diabetes mellitus, crohn's disease, down syndrome) Granulocytes in most patients with LJP or RPP exhibit more or less comprised functions 6. Gingival crevicular fluid Gingival Crevicular Fluid transports PMN, antibodies, Tooth surface host enzymes and helps flush out the sulcus Positive pressure from gingival blood vessels, through JE into sulcus. blood vessels will be discussed later 7. Non specific antibodies Non-specific: from circulation Specific: against bacteria localized in the gingival tissues This topic will be discussed in more details later 8. Immune system interactions PMN Complement Antibody interaction 8. Immune system interactions The complement system is a series of 25 proteins manufactured in the liver and are are activated by, and work with, (i.e. complement) antibodies Function of complement: lysing (bursting) of cells and signal to phagocytes that a cell have to be removed. Complement coated bacterial cells are easier for PMN to phagocytose binding to bacteria, and when activated, can directly kill them. Defensive factors All of these factors may operate at the same time to reduce the bacterial load and thus prevent an overresponse of the tissue defense systems which could result in the formation of a lesion. Summary of primary periodontal defenses Physical barrier High turnover rate Large inter-cellular spaces permit PMN progress to sulcus JE produces cytokines which call to PMN Crevicular fluid, flushing carries cells + antibodies Immune system interactions