Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
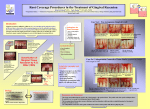
Gingival Fibromatosis & Myltiple Hyaline Fibromas Sheena Stegmann 11/08/2010 Name of Syndrome: Patient: Calvin Smith Age: 9 Gender: Male Height: 4’ 6” Weight: 70 lbs. Vital Signs: Pulse: 80 BPM Respiratory rate: 25 RPM Blood Pressure: 100/60 mmHG Temperature: 97.9 degrees Chief complaint Medical Alert Dense gingival tissue that was preventing tooth eruption Teeth were totally entrapped in a gingival mass of tissue, thus, impairing their eruption. Gingival Fibromatosis & Myltiple Hyaline Fibromas Cause of Syndrome - Medical History (if applicable) Gingival fibromatosis can be caused by number of factors, including: • Herdity/Genetics •Inflammation •Leukemic infiltration and •Use of medications such as phenytoin, cyclosporine or nifedipine and vigabatrin. Age/race/sex predilections and Systemic Clinical Features: •Occurs in children •Race and age are no concerning factor •Genetics is the leading cause •The clinical presentation is generalized firm nodular enlargements with pink to red and inflamed, smooth to stippled surfaces, with little tendency to bleed. •In some cases the gingivae can become so firm and dense as to feel like bone on palpation. •The enlargement is painless and may extend up to the mucogingival junction but does not affect the alveolar mucosa. Orofacial Clinical Features •The histological appearance shows hyperplasia of fibrous tissue of the corneum. •The tissues are composed mainly of dense connective tissue, which is rich in collagen fibrils. •The overlying epithelium is normal, but is slightly hyperplastic in some areas. •Gingival enlargement may occur during the eruption of primary teeth and affect both dentitions, but does not occur once the patient grows into adulthood. Radiographic Features of this Syndrome The radiographic findings indicated a gross delay in tooth eruption. The permanent maxillary central incisors and first permanent molars were still unerupted. Special considerations in Treatment of this patient? How is it Diagnosed? How common is it? Is it a horse or zebra? •Under general anesthesia, using CO2 laser, surgical removal of dense fibrous tissue was performed exposing the teeth crowns. •Conservative restorative treatment was performed as well. •The patient tolerated the procedure well with no postoperative complications. •After recovery, oral hygiene instructions were reinforced and complete tissue recovery was evident after 3 weeks. •Partial recurrence of the gingival overgrowth was noted after 3 months. At this stage, professional prophylaxis was performed by a dental hygienist. •At the six months evaluation, further eruption of all first permanent molars to the level of the second primary molars was noted. •Needs a second surgery •Definitely a ZEBRA case Intraoral pictures Upper anterior region—severe inflammation around the entrapped Teeth. Lower anterior region—teeth are embedded in coarse gingival tissue. Radiographs Before any treatment After 6 months List Sources and References •http://www.dent.ucla.edu/pic/members/gingTumors/part1/pyogenic.html •http://www.aapd.org/upload/articles/Katz3-02.pdf •www.fccjdentalhygiene.netfirms.com/pathologyquizch6key.htm •Oral Pathology Textbook p.210-211