Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Periodontal disease wikipedia , lookup
Acute pancreatitis wikipedia , lookup
Lymphopoiesis wikipedia , lookup
Polyclonal B cell response wikipedia , lookup
Molecular mimicry wikipedia , lookup
Rheumatic fever wikipedia , lookup
Immune system wikipedia , lookup
Adaptive immune system wikipedia , lookup
Atherosclerosis wikipedia , lookup
Cancer immunotherapy wikipedia , lookup
Adoptive cell transfer wikipedia , lookup
Rheumatoid arthritis wikipedia , lookup
Hygiene hypothesis wikipedia , lookup
Sjögren syndrome wikipedia , lookup
Immunosuppressive drug wikipedia , lookup
Psychoneuroimmunology wikipedia , lookup
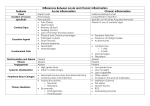
Dr Shoaib Raza • Acute inflammation is morphologically characterized by – Dilatation of small blood vessels – Slowing of blood flow – Leukocyte infiltration – Fluid accumulation in interstitial space • Special morphologic patterns are seen – Severity of reaction – Specific cause of reaction – Particular tissue/site involved Marked by • Outpouring of thin fluid derived from Plasma Secretions of mesothelial cells • Accumulation of fluid in these cavities is called as EFFUSION • Skin blister represent accumulation of serous fluid • • Characterized by deposition of fibrin in the extracellular spaces Fibrinous exudate develops when – Vascular leaks are large, or – Local procoagulant stimulus • Fibrinous exudate is characteristic of: – Inflammation in the lining of body cavities • Conversion to fibrous tissue (organization) within pericardial sac leads to fibrous thickening (Fibrinous pericarditis) • Characterized by production of large amounts of pus (purulent exudate), consist of – PMN, liquefactive necrosis, edema fluid • • Pyogenic bacteria produce this Abscess are localized collection of purulent inflammatory exudate – Suppuration buried in an organ, tissue or confined space • Central necrotic area • Preserved PMN around this necrotic focus • Vascular dilatation, parenchymal and fibroblastic proliferation occurs peripherally • • • A local defect or excavation, of the surface of an organ or tissue, produced by the sloughing (shedding) of inflamed necrotic tissue Occur when tissue necrosis and inflammation exist on or near a surface Encountered in – Mouth, stomach, intestine, genital or urinary tract – Skin & subcutaneous tissues Complete resolution Healing by connective tissue replacement • Fibrosis, organization, scar formation Progression to chronic inflammation Inflammation of the prolonged duration (weeks or months) in which inflammation, tissue injury and attempts at repair coexist It may • Follow acute inflammation • Begin insidiously as low grade smoldering response without any manifestation of the acute reaction Chronic inflammation arises in following settings: • Persistent infection by microorganism Mycobacteria, fungi, viruses, parasites etc • Immune mediated inflammatory diseases Autoimmune diseases (Allergic disorders) • Prolonged exposure to potentially toxic agents Exogenous Silica, carbon Endogenous Atherosclerosis Chronic inflammation is characterized by: • Infiltration with mononuclear cells Macrophages, lymphocytes, plasma cells • Tissue destruction Induced by persistence of offending agent • Attempts at healing by connective tissue replacement of damaged tissue Proliferation of small blood vessels (Angiogenesis) Fibrosis Macrophages are the predominant cells of chronic inflammation • Component of mononuclear phagocyte system Liver Spleen & Lymph nodes Lung CNS Bone Kupffer cells Sinus histiocytes Alveolar macrophages Microglia Osteocytes • Arise from common precursor in bone marrow • Monocytes enter tissue & differentiate into macrophages Migration begins early in acute inflammation Predominant cells after 48 hours Macrophages activation occur via: • Microbial products via TLRs • IFN-γ secreted by sensitized T Cells, NK cells, Activation results in: • Increased level of lysozyme • ROS & NO production • Production of cytokines, growth factors, etc Activation of macrophages result • Toxicity to microbes & host cells • Release of protease etc • Influx of other cell types via cytokines • Fibroblast proliferation • Angiogenesis Arsenal of mediators make them in: powerful allies in the defense, but the same weaponry can induce tissue destruction In acute inflammation: • If irritant is eliminated, macrophages disappear Either dying off Drain to regional lymph nodes via lymphatics In chronic inflammation: • Accumulation of macrophages persists As a result of continuous recruitment from the circulation and local proliferation at the site of inflammation Lymphocytes: • Cell mediated or antibody mediated reactions • Selectins, integrins and chemokines help in their recruitment • TNF, IL-1, etc promote leukocyte recruitment, Persisting the inflammatory response • Macrophages present antigens to T Cells Plasma cells • May transform the inflammatory site into tertiary lymphoid organ Eosinophils: • Abundant in immune reaction mediated by IgE and parasitic infestations (infections) • Eotaxin is a potent chemotactic agent for eosinophil • Eosinophil produce: Major Basic Proteins Mast Cells: • Widely distributed in connective tissue • Participate in both acute & chronic inflammation • Express FcεRI • Release histamine, prostaglandins, serotonin • Cytokines production Distinctive (Specific) pattern of chronic inflammation Immune reactions are usually involved in granuloma formation Granuloma is an attempt to contain an offending agent Granuloma composed of: • Modified macrophages (epitheliod cells) • Collar of lymphocytes • Giant cells (multinucleated cells) • + Necrosis (caseous) Granulomas are of two main types: • Foreign body granuloma • Immune granulomas Delayed type hypersensitivity reactions Fungal Infections: Bacteria: • Histoplasmosis • Blastomycosis • Tuberculosis • Leprosy Metal/Dust • Berylliosis • Silicosis Foreign body • Splinter • Suture • Graft material Sarcoidosis Parasites: • Schistosomiasis Acute Phase Response (systemic inflammatory response syndrome) • Fever: Usually seen in infections Pyrogens stimulate hypothalamus to form PG • Acute Phase proteins: CRP, Fibrinogen, Serum Amyloid A (SAA) • Leukocytosis: Leukemoid reactions, leukopenia • Others: Increased pulse rate, Increased blood pressure, decreased sweating, rigors, chill, anorexia, somnolence, malaise Defective Inflammation: • Increased susceptibility to infections • Delayed wound healing Excessive Inflammation: • Hypersensitivity reactions • Autoimmune disorders • Other non-immune related disorders AS, CHD, Alzheimer’s Disease • Pathology in many infections, metabolic disorders, etc.