Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Bipolar II disorder wikipedia , lookup
Asperger syndrome wikipedia , lookup
Causes of mental disorders wikipedia , lookup
Wernicke–Korsakoff syndrome wikipedia , lookup
Diagnosis of Asperger syndrome wikipedia , lookup
Rumination syndrome wikipedia , lookup
Glossary of psychiatry wikipedia , lookup
Symptoms of victimization wikipedia , lookup
Externalizing disorders wikipedia , lookup
Psychological trauma wikipedia , lookup
Dissociative identity disorder wikipedia , lookup
Depression in childhood and adolescence wikipedia , lookup
Treatments for combat-related PTSD wikipedia , lookup
Conversion disorder wikipedia , lookup
Post-traumatic amnesia wikipedia , lookup
Retrograde amnesia wikipedia , lookup
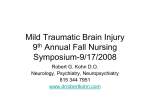
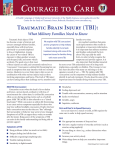
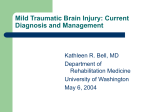
Wounds of War: Traumatic Brain Injury Rex M. Swanda, Ph.D., ABPP-CN Neuropsychology Program New Mexico VA Healthcare System Traumatic Brain Injury (TBI) Brain injury caused by an external mechanical force such as a blow to the head, concussive forces, acceleration-deceleration forces, or projectile missile (e.g., bullet). CONCLUSIONS TBI does not typically occur in isolation Emotional and psychosocial stressors Reported TBI most frequently involves mild TBI Credible research indicates that full cognitive recovery is the norm in mild TBI (e.g., LOC < 30 minutes) Important to identify TREATABLE symptoms No direct treatments for TBI Associated psychological symptoms are associated with subjectively reported TBI symptoms that ARE highly treatable Depression, PTSD, Substance Abuse Incidence of TBI 500,000 to 2,000,000 per year (civilian) Poorly defined Poorly documented Risk Factors Associated with TBI Age 15 to 24 years of age First 5 years of life Elderly Males outnumber Females 2:1 Except over age 75 Risk Factors Associated with TBI Lower Socio-Economic Status Unemployment Lower Education Prior History of a Medical Condition Affecting the Central Nervous System Alcoholism or Substance Abuse History of Prior Head Injury Frequent Causes of TBI Falls Motor Vehicle Accidents Interpersonal Violence Classification of TBI Closed Head Injury Skull intact, Brain tissue not exposed 90% of civilian head injury Diffuse effects are common • Attention / Executive Penetrating Head Injury (Open Head Injury) Skull and dura are penetrated Focal injury is more common High Risk Areas for Contusion Long-Term Consequences of TBI Cognitive consequences Emotional consequences Social consequences Indicators of Severity for all types of head injury Loss of Consciousness (Loss of Awareness) Coma (operationalized by Dikmen, et al. as Time to Follow Commands) Post Traumatic Amnesia (PTA) Signs of Intracranial Injury Glasgow Coma Scale 15 point scale measures presence, degree, and duration of coma Based on Eyes Opening response (1 – 5 pts) Best Verbal response (1 – 5 pts) Best Motor response (1 – 6 pts) Post-traumatic Amnesia A period of anterograde amnesia in which new memories cannot be consistently made and recalled that follows recovery of consciousness in head injury or other neurological trauma. The duration of PTA is often used as a predictor of the degree of recovery. Classification of Head Injury Mild Head Injury Glasgow Coma Scale 13 – 15 PTA 5 – 60 minutes Moderate Head Injury Glasgow Coma Scale 9 – 12 PTA up to 24 hours Moderate to Severe Head Injury Glasgow Coma Scale 3 – 8 PTA 1 to 7 days or longer What does empirical research tell us about the consequences of Traumatic Brain Injury Dikmen, S.S., Machamer, J.E., Winn, R., & Temkin, N.R. (1995). Neuropsychological outcome at 1-year post head injury. Neuropsychology, 9, 80-90. Dikmen, S., Machamer, J., & Temkin, N. (2001). Mild Head Injury: Facts and Artifacts. Journal of Clinical and Experimental Neuropsychology, 23, 729-738. What does empirical research tell us about the consequences of Traumatic Brain Injury Hoge, C.W., McGurk, D., Thomas, J.L., et al (2008) Mild traumatic brain injury in U.S. soldiers returning from Iraq. New England Journal of Medicine. 358, no. 5, 453-463. Outcome Research: Mild TBI Appropriately designed research studies indicate that virtually 100% mild head injured subjects show no cognitive impairment within about 3 months to a year (outside) post-injury EXCELLENT Prognosis for Mild Head Injury TBI Outcome Research: Surreya Dikmen, Ph.D. Studies date from 1986 Follow patients and controls over time Prospective Design Consecutive hospital admissions of welldefined Head Injury patients Harborview Medical Center (Seattle, WA), a Level I Trauma Center TBI Outcome Research: Dikmen Study minimized selection bias Large demographically representative group English-speaking only (for testing criteria) Did NOT screen out preexisting conditions Unusually high rates of follow-up 85% followed up after one year Outcome Research: Dikmen Pre-existing conditions included: Prior significant head injury Alcoholism receiving treatment History of cerebral disease Psychiatric disorder (schizophrenia, bipolar disorder) Outcome Research: Dikmen Broad spectrum of head injury severity Minimum injury criteria include: Any period of loss of consciousness Post-traumatic amnesia of at least 1 hour Other objective evidence of head trauma (e.g., hematoma) Injury severe enough to hospitalize Survival to complete at least 1 month follow-up for neuropsychological assessment baseline Outcome Research: Dikmen Trauma Control Subjects recruited from ER after trauma to parts of body, other than head Controls matched head-injured on age sex education Outcomes Following TBI Dose-Response Relationship Dikmen, et al. (1995) found a significant relationship between length of coma (Time to Follow Commands) and level of performance on sensitive neuropsychological measures at 1 year post-injury Greater cognitive impairment is associated with longer periods of coma Outcomes Following TBI Mild head injured patients (TFC < 1 hour) were indistinguishable from trauma controls at one year post-injury on sensitive measures of cognitive functioning Outcomes Following TBI Although there were no significant differences on cognitive testing, premorbid characteristics and risk factors were more powerful than head injury in explaining persistent psychosocial symptoms at one year post-injury (Dikmen, et al. 2001) Contributing Risk Factors Account for Persistent Symptoms in cases of Mild Closed Head Injury Age Education Pre-existing conditions Treatment for alcohol or substance abuse CNS disorder (prior head injury) Psychiatric condition (including PTSD) Somatoform-Spectrum diagnoses Dikmen’s Conclusion “It is equally unusual for mild head injury to produce deficits after 1 year as it is for severe head injury to produce no deficits after 1 year.” (Dikmen, et al., 1995) Recent Study of Soldiers Returning from Iraq Hoge, et al (2008, in NEJM) studied 2525 U.S. soldiers returning from Iraq. 124 (4.9%) reported injuries with LOC 43% of these met criteria for PTSD 260 (10.3%) reported altered Mental Status 27.3% of these met criteria for PTSD 435 (17.2%) reported other injuries 16.2% of these met criteria for PTSD 1760 reported no injury 9.1% of these met criteria for PTSD Recent Study of Soldiers Returning from Iraq Although the relationship is associative and not necessarily causal…… …“after adjustment for PTSD and depression, mild traumatic brain injury was no longer significantly associated with these physical health outcomes or symptoms, except for headaches.” Consistent with Dikmen’s research So, how do we account for subjective complaints of lasting symptoms following TBI ? Postconcussion Syndrome ICD-10 Diagnostic Criteria A. History of head trauma with loss of consciousness precedes symptoms onset by maximum of four weeks Postconcussion Syndrome ICD-10 Diagnostic Criteria B. Symptoms in 3 or more of the following categories: Headache, dizziness, malaise, fatigue, noise tolerance Irritability, depression, anxiety, emotional lability Subjective concentration, memory, or intellectual difficulties without neuropsychological evidence of marked impairment Insomnia Reduced alcohol tolerance Preoccupation with above symptoms and fear of brain damage with hypochondriacal concern and adoption of sick role. Misattribution of Symptoms Why do patients, families – even providers – “misattribute” symptoms, such as memory problems, “loss” of cognitive abilities, or declining cognitive performance – to brain injury? Psychological Theories for Understanding Postconcussion Syndrome and “Misattribution of Symptoms” “Good Old Days” Hypothesis “Nocebo” Effect Diathesis-Stress Model Expectation as Etiology “Good Old Days” Hypothesis Gunstad & Suhr (2001) Tendency of people to recall past symptoms and functioning more favorably than was actually the case Suggests that, following any negative event, people tend to attribute all symptoms to that negative event, regardless of a preexisting history of that very problem or any other factors that may be influencing that problem. Nocebo Effect Hahn (1997) The notion that expectations of sickness and associated emotional distress cause the sickness in question Suggests that response expectations are “anticipations of automatic reactions to particular situational cues” and are outside both volition and conscious thought. Diathesis-Stress Model Wood (2004) Examines the interaction between physiologic and psychological factors that generate and maintain postconcussional symptoms. Suggests that iatrogenic forces can influence a patient’s recovery after MTBI, especially if health care providers inadvertently reinforce misperceptions of symptoms or insecurities about recovery Diathesis-Stress Model In McCrea (2008, p. 176) “an unfortunate scenario unfolds when a patient with vague symptom complaints and no clear indication of significant head trauma is told he has “brain damage” and will never make a complete neurologic, symptom, or functional recovery.” “The long-term damage of creating that perception for a patient is most difficult to undo.” Expectation as Etiology Mittenberg et al (1992) Suggests that the incidence and persistence of PCS may be explained by the degree to which an individual misattributes common complaints to a prior head injury Examine in detail as an example of “normal” tendencies to misattribute symptoms Misattribution of Symptoms Poor understanding that many common symptoms represent a “final common endpoint” of many overlapping diagnoses and disorders Poor understanding of mechanisms of brain processing, injury, and recovery Poor understanding of base rates of symptoms among “normal” individuals Symptoms Overlap Across Diagnoses From: McCrea (2007) Mild Traumatic Brain Injury and Postconcussion Syndrome p. 160, Table 161 Headache Dizziness Irritability Memory Problems Attention Problems College Students 36 % 18% 36% 17% 42% Chronic Pain 80% 67% 49% 33% 63% Depressed 37% 20% 52% 25% 54% Non-TBI Personal Inj 77% 41% 63% 46% 71% Mild TBI 42% 26% 28% 36% 25% Poor Understanding of Brain Mechanisms Involved in Memory “Memory” complaints are among most common symptoms associated with postconcussion syndrome Information Processing Model of Memory helps clarify the role that “psychological factors” can play in memory complaints Example of the important role that basic education plays as a therapeutic intervention Information Processing Model of Memory Base Rates and Misattribution of Symptoms Base Rates: The frequency with which abnormal neuropsychological findings are observed among “normal” individuals. It is “normal” to perform in the impaired range on some cognitive measures Heaton, Grant, and Matthews norms indicate that very few healthy individuals complete a neuropsychological protocol without any impaired scores, while as many as 38% of “normals” perform in the impaired range on 6 or more discrete scores in a 40-score battery. Percent of “normal” individuals who score in the impaired range on 0 to 6 or more measures in a battery of 40 measures Expectation as Etiology Mittenberg, et al. (1992) 223 volunteers 100 pts with closed head injuries Average 1.7 years after injury Average reported LOC = 23 minutes 30-symptom checklist of items Affective Somatic Memory Examples of symptom checklist Forgets where car is parked Forgets why they entered a room Loses items around the house Sensitivity to bright light Blurry or double vision Concentration difficulty Depression Control Subjects Which symptoms do you (healthy volunteers) currently experience? ….Now imagine an MVA-related head injury 6 months before, in which you were knocked out, hospitalized for a week or two. Respond to the symptoms that you think you would have after an accident like this. Patients with head injuries Identify the symptoms you think you would have had before the accident (how you used to be) Then identify symptoms that you notice now, after the accident (how you are now) No difference between the incidence of Post-concussion Symptoms expected by controls and those reported by head injury patients. Control Group M = 14.8 s.d. = 7.6 Head Injured M = 13.8 s.d. = 8.3 Incidence of Expected and Actual Postconcussion Symptoms % controls % patients Headache 80.0 59.1 Anxiety 68.1 58.3 Concentration difficulty 66.8 70.5 Irritability 50.0 65.9 Forgets why entered room 34.8 50.6 Loses items around house 28.5 28.1 However, Head Injury patients significantly underestimated symptoms prior to injury, compared to normal base rates Head injury patients underestimated premorbid frequency of 21 specific symptoms compared to base rates of normal controls Normal Base Rates of normal controls compared to head injury patient’s premorbid estimates of symptoms % controls % patients Forgets where car parked 32.0 7.0 Loses car keys 31.0 6.0 Forgets groceries 28.3 9.0 Concentration difficulty 13.5 5.0 Forgets appointment dates 20.2 7.0 Loses items around house 17.0 4.0 “Results suggest a tendency for patients with head injuries to attribute [normally occurring] premorbid symptoms to head trauma.” Neuropsychological Assessment of Effort and Motivation Malingering (DSM-IV) …the intentional production of false or grossly exaggerated physical or psychological symptoms, motivated by external incentives such as avoiding military duty, avoiding work, obtaining financial compensation, evading criminal prosecution, or obtaining drugs. Diagnoses Involving Symptom Exaggeration or Unfounded Physical or Psychological Symptoms Malingering – intentional feigning or exaggerating symptoms of illness or injury for external gain. Intentional Production of Symptoms Absent Symptoms Satisfy Obvious Psychological Needs External Incentives Not Obvious Likely Somatoform Disorder Absent Not Obvious Likely Conversion Disorder Absent Not Obvious Symptoms worsened by stress and conflict Somatization Disorder Hypochondriasis Absent Not Obvious Misinterpretation of Physical Symptoms Factitious Disorder Present Not Obvious Need to Maintain the “Sick” Role Malingering Present Present Not Obvious Base Rates of Malingering and Symptom Exaggeration Mittenberg, Patton, Canyock, & Condit (2002) Surveyed ABCN diplomates Rates of cases involving “probable malingering” and “symptom exaggeration” 19% personal injury 30% disability 19% criminal 8% general criminal cases Base Rates of Malingering and Symptom Exaggeration Larrabee, G. (2003) Reviewed 11 studies 1363 consecutively evaluated mild traumatic brain-injury litigants. Found a rate of about 40% symptom exaggeration or malingering among the sample Base Rates of Malingering and Symptom Exaggeration Chafetz & Abrahams (2005) Adults seeking Social Security disability 13.8% met criteria for definite malingering 58.6% met criteria for probable malingering (two or more failed validity indicators) Combined definite/probable base rate of malingering of 72.4% Base Rates of Malingering and Symptom Exaggeration Bush, et al (2005) Likely rates of malingering or symptom exaggeration – and potential costs to the system (SSD, VA, personal injury litigation) – are significant enough that National Academy of Neuropsychology recommends that symptom validity testing be included as part of comprehensive neuropsychological test battery. What Makes Sense “Neuropsychologically” in a Specific Case? Circumstances of the Alleged Injury Reported Changes in Functioning Over Time Consideration of Brain – Behavior Relationships Pattern of Neuropsychological Performance Documented Evidence of Injury versus Patient’s Account of the Injury Consider subjective reports of LOC Force of Collision Level of toxic exposure In light of documentation Ambulance / Police Reports Medical Records Laboratory Reports Reported Changes Over Time versus Natural Course of Recovery Mild head injury symptoms should improve over time – not worsen “It is equally unusual for mild head injury to produce deficits after one year as it is for severe head injury to produce no deficits after one year.” Dikmen, et al., 1995 The pattern of neuropsychological performance should be consistent with the reported symptoms and circumstances of the alleged injury “Odd” complaints for mild head injury without signs of focal neuroanatomical injury Stuttering Loss of vocabulary Severe self-neglect with preserved ability to drive Loss of autobiographical memory Loss of developmentally overlearned skills Tying one’s shoes Spelling Two Main Approaches to Detect Poor Effort or Malingering Identification of motivationally-impaired patterns of performance on traditional neuropsychological tests Use of specific measures of effort Deviations from Expected Patterns of Functioning VIQ vs. PIQ differences on WAIS testing Strengths on “Hold” vs. “Don’t Hold” Measures Unexpected pattern of Index Scores Verbal Comprehension Index Perceptual Organization Index Working Memory Index Processing Speed Index Worse performance on easier vs harder items Specific Measures of Effort and Validity MMPI-2 Personality Self-Report “F” family (F, Fb, Fp, F – K) FBS VRIN Variable Response indicators TRIN True Response Set Forced Choice Recognition Techniques Many types of Stimuli Pictures, Faces, Words, Numbers, Textures Expectation for high levels of Success, even among significantly impaired individuals Chance rules 15-Item Memory 1 2 3 A B C 1 2 3 a b c Outright “Malingering” is Rare Malingering is only one point on a diagnostic continuum of poor effort and symptom exaggeration Outright “Malingering” is Rare Poor effort and symptom exaggeration are most frequently associated with: Chronic illness behavior Significant emotional symptoms • Depression • Anxiety • PTSD Poor expectations for one’s own performance (Nocebo effect) Effort and Motivation are best assessed in light of: Objective Records and Documentation Known brain-behavior relationships Natural history of recovery from injury Unusual pattern of performance on standard materials CONCLUSIONS TBI does not typically occur in isolation Emotional and psychosocial stressors are typically significant CONCLUSIONS Reported TBI most frequently involves mild TBI CONCLUSIONS Credible research indicates that full cognitive recovery is the norm in mild TBI Duration of documented Loss Of Consciousness is most frequently subtle, or less than 30 minutes CONCLUSIONS Important to identify TREATABLE symptoms No direct treatments for TBI, BUT Highly successful treatment programs for Depression PTSD Substance Abuse Family/Couples Therapy CONCLUSIONS TBI does not typically occur in isolation Emotional and psychosocial stressors Reported TBI most frequently involves mild TBI Credible research indicates that full cognitive recovery is the norm in mild TBI (e.g., LOC < 30 minutes) Important to identify TREATABLE symptoms No direct treatments for TBI Associated psychological symptoms are associated with subjectively reported TBI symptoms that ARE highly treatable Depression, PTSD, Substance Abuse