Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
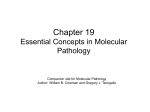
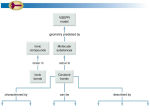
Chapter 19 PART IV: Molecular Pathology of Human Disease Molecular Basis of Diseases of the Gastrointestinal Tract Companion site for Molecular Pathology Author: William B. Coleman and Gregory J. Tsongalis FIGURE 19.1 Gastric carcinogenesis: Stepwise Progression of H. pylori-Associated Gastric Cancer (Panels A1–A4), and Hereditary Diffuse Gastric Cancer (Panels B1 and B2). Panel A1. Chronic active gastritis involving the mucosa of the gastric antrum (H&E stain, original magnification 10×); Panel A2. Immunohistochemical stain highlights H. pylori organisms with typical S and comma shapes, seen at higher magnification in the inset. H. pylori organisms typically appear attached or adjacent to the gastric surface and foveolar epithelium (original magnification 40×); Panel A3. Gastric mucosa with intestinal metaplasia and low-grade dysplasia/adenoma (H&E stain, original magnification 10×); Panel A4. Gastric carcinoma of intestinal type (moderately differentiated adenocarcinoma) (H&E stain, original magnification 10×); Panels B1 and B2 (Courtesy of Dr. Adrian Gologan, Jewish General Hospital, McGill University). Gastric mucosa of patient with hereditary diffuse gastric cancer (HDGC) with in situ signet ring cell carcinoma (arrow) (B1) and invasive signet ring cell carcinoma expanding the lamina propria between the gastric glands (E), (H&E stain, original magnification 20×). Companion site for Molecular Pathology Copyright © 2009 by Academic Press. All rights reserved. 2 FIGURE 19.2 Stepwise Progression of Molecular Events During Gastric Carcinogenesis. Companion site for Molecular Pathology Copyright © 2009 by Academic Press. All rights reserved. 3 FIGURE 19.3 Stepwise Progression of Colorectal Neoplasia: Progression of Neoplasia in Sporadic Colorectal Cancer and in Inflammatory Bowel Disease-Associated Colitis. In the sporadic colorectal cancer pathway, adenomas characterized in the early stages by low-grade epithelial dysplasia precede the development of high-grade dysplasia, which may then progress to invasive adenocarcinoma. In IBD-associated neoplasia, the background colonic mucosa reveals variable degrees of chronic colitis, and eventually foci of low-grade dysplasia develop, which in turn may progress to high-grade dysplasia and invasive adenocarcinoma. The morphologic features of the neoplastic lesions significantly overlap between sporadic colorectal cancer and IBDassociated neoplasia, but the inflammatory environment that characterizes chronic colitis dictates a number of different molecular mechanisms of neoplastic development and progression. Companion site for Molecular Pathology Copyright © 2009 by Academic Press. All rights reserved. 4 FIGURE 19.4 Colorectal Cancer Pathways: Histopathology and Molecular Correlates. Panels A and B: The Serrated Pathway. Adenocarcinomas that develop through the serrated pathway arise from serrated polyps that include traditional serrated adenomas; (A) and sessile serrated adenomas (B), (H&E stain, original magnification 5× and 10×, for panels A and B, respectively). Traditional serrated adenomas show both serrated architecture and dysplasia similar to that seen in adenomatous mucosa, whereas sessile serrated adenomas reveal architectural abnormalities but no evidence of classic dysplasia. Panels C and D: The Microsatellite Instability Pathway. Poorly differentiated colonic adenocarcinoma with prominent intratumoral lymphocytes, best seen in the inset (C), (H&E stain, original magnification 10×). By immunohistochemistry, the tumor cells are negative for MSH2, while the surrounding lymphocytes and stromal cells show preserved expression of MSH2 protein in the non-neoplastic cell nuclei (D), (Immunohistochemistry, original magnification 10×). (E) The presence of microsatellite instability in the tumor DNA is demonstrated by microsatellite instability at the microsatellite markers BAT25 and BAT26 characterized by the appearance of new PCR amplification peaks of smaller size (tailed arrows) as compared to non-neoplastic DNA from the same patient (arrow tip). Companion site for Molecular Pathology Copyright © 2009 by Academic Press. All rights reserved. 5 FIGURE 19.5 Molecular Events in the Stepwise Lesions of Sporadic Colorectal Carcinogenesis. Companion site for Molecular Pathology Copyright © 2009 by Academic Press. All rights reserved. 6 FIGURE 19.6 Molecular Events in the Stepwise Lesions of Inflammatory Bowel Disease-Associated Neoplasia. Companion site for Molecular Pathology Copyright © 2009 by Academic Press. All rights reserved. 7 FIGURE 19.7 Algorithm for Molecular Testing of HNPCC/Lynch Syndrome Colorectal Cancer. Modified from [305]. Companion site for Molecular Pathology Copyright © 2009 by Academic Press. All rights reserved. 8 FIGURE 19.8 The Wnt Pathway and Familial Adenomatous Polyposis. (A) Signaling of the Wnt pathway is mediated through the Frizzled family of receptors, and a co-receptor LRP5 or 6. In the absence of ligand, the pathway is inactive through the negative regulation of the downstream effector β-catenin. When present in sufficient quantity in the nucleus, β-catenin stimulates transcription of target genes. Lack of signaling through the Frizzled receptor results in sequestration of β-catenin in a multiprotein complex including APC, Axin, and other proteins, which exert a negative effect both through the cytoplasmic sequestration of βcatenin and by targeting it for destruction by the proteasome through phosphorylation. (B) In the presence of Wnt ligand, the Frizzled receptor and LRP5/6 form a complex which results in the recruitment and sequestration of Axin at the cell surface, thereby inhibiting the kinase activity of the APC complex. This results in the stabilization and nuclear translocation of β-catenin, thus resulting in transcription of target genes. (C) In the setting of an APC gene mutation, the multiprotein APC/Axin/β-catenin complex is disrupted, most commonly due to truncation of the APC protein in domains responsible for protein-protein interaction. This results in stabilization and nuclear translocation of β-catenin, with the net effect of constitutively active transcription of growth-promoting genes otherwise under tight regulation. (D) Typical appearance of polyps in FAP, which are indistinguishable from spontaneous nonsyndromic polyps, but are numerous and may eventually cover most of the surface of the colon with a carpet appearance (D1; From the files of the Department of Pathology, Hospital of the University of Pennsylvania). Tubular adenoma (D2) and adenomatous colonic mucosa (D3) at an early stage before the development of larger adenomas and adenocarcinomas (H&E stain, original magnification 5×). Companion site for Molecular Pathology Copyright © 2009 by Academic Press. All rights reserved. 9 FIGURE 19.9 APC Gene Mutation and Phenotype Correlation in FAP. The figure illustrates the APC gene functional domains and mutation-phenotype correlations. The APC protein product consists of 2843 amino acids with multiple functional domains, including a dimerization domain, microtubule domain, and binding sites for β-catenin and axin (pictured as gray boxes). Mutations within certain codon ranges may correlate to a clinical phenotype as depicted in the yellow boxes. Germline mutations generally fall within the entire spectrum of depicted mutational sites, while somatic mutations tend to cluster within the mutation cluster region (MCR). Of note, a profuse polyposis phenotype is seen in patients in whom a germline mutation between codons 1250 and 1464 is seen, with the clinical presentation of >5000 polyps. Mutation at codon 1309 is associated with profuse polyposis and earlier onset of disease. I1307K represents a mutation common in the Ashkenazi Jewish population. Adapted from [316,317,329]. Companion site for Molecular Pathology Copyright © 2009 by Academic Press. All rights reserved. 10