Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Lymphopoiesis wikipedia , lookup
Immune system wikipedia , lookup
Psychoneuroimmunology wikipedia , lookup
DNA vaccination wikipedia , lookup
Adaptive immune system wikipedia , lookup
Monoclonal antibody wikipedia , lookup
Immunosuppressive drug wikipedia , lookup
Polyclonal B cell response wikipedia , lookup
Molecular mimicry wikipedia , lookup
Innate immune system wikipedia , lookup
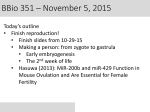
BJD British Journal of Dermatology C U TA N E O U S B I O L O G Y Intradermal injections of polyarginine-containing immunogenic antigens preferentially elicit Tc1 and Th1 activation and antitumour immunity H. Mitsui, T. Okamoto, M. Kanzaki, T. Inozume, N. Shibagaki and S. Shimada Department of Dermatology, Faculty of Medicine, University of Yamanashi, 1110 Shimokato, Chuo-shi, Yamanashi 409-3898, Japan Summary Correspondence Naotaka Shibagaki. E-mail: [email protected] Accepted for publication 9 September 2008 Key words antigen presentation ⁄ processing, protein transduction, skin inflammation, T cells, vaccine Conflicts of interest None declared. H.M. and T.O. contributed equally to this work. DOI 10.1111/j.1365-2133.2009.09490.x Background We previously have shown that nona-arginine protein transduction domain (R9-PTD) induced efficient protein-antigen (Ag) transduction of dendritic cells (DCs) in vitro, resulting in the efficient induction of strong Ag-specific immune responses mediated by CD8+ and CD4+ T cells and in superior antitumour effects in vivo in cancer-bearing mice. Objectives The Ag-specific immune responses caused by intradermal (i.d.) injections of R9-PTD-containing protein Ags without DC preparation were investigated. We also investigated the antitumour effects by intratumoral (i.t.) injections of rR9-containing protein Ags. Methods Synthesized SIINFEKL peptide, or recombinant ovalbumin fusion proteins (rOVA, rR9-OVA), were directly injected into abdominal skin in naı̈ve C57BL ⁄6 mice. OVA-specific cytotoxic T lymphocyte (CTL) activity, serum IgG titre and cytokine profiles were investigated. Histopathological analyses were also performed. In a cancer vaccination model, EG.7 (OVA-cDNA transfectants thymoma) cells were inoculated intradermally in C57BL ⁄6 mice, and the antitumour effects were evaluated by i.t. injections of rR9-OVA in a treatment setting. Results i.d. injections of rR9-OVA into naı̈ve C57BL ⁄6 mice elicited OVA-specific CTLs and produced IgG2-dominant immunoglobulin. The i.d. injections of rR9OVA also induced inflammatory cell infiltrates containing neutrophils, monocytes and lymphocytes, as well as production of inflammatory cytokines such as interferon (IFN)-c, interleukin-2 and IFN-inducible protein 10, with presenting SIINFEKL epitopes on major histocompatibility complex (MHC) class I molecules at the injection area. i.t. injections of rR9-OVA into EG.7 tumour mass significantly suppressed tumour growth, and these effects were completely abrogated by the depletion of CD8+ T cells. These antitumour effects were superior to those elicited by i.t. injections of rR9-OVA-treated DCs. Conclusions i.d. injections of rR9-containing immunogenic Ag without adjuvants simultaneously induce dual immunological effects: the induction of Tc1- and Th1-dominant immune responses, and the induction of inflammatory and CTLmediated immune responses at the injection area by expressing Ag epitopes on MHC class I molecules as targets. This simple vaccination approach with R9-PTDcontaining fusion proteins might be useful as prophylactic immunotherapy for cancer or infectious diseases. Cytotoxic T lymphocytes (CTLs) are acquired immune effector cells that are involved in host responses to viruses, tumours and other intracellular pathogens. Antigen (Ag)-specific CTL induction in vivo requires the internalization and ⁄or cross-presentation of Ag by professional Ag-presenting cells. However, phagocytotic Ag uptake may result in only a small amount of Ag epitopes on major histocompatibility complex (MHC) class I molecules due to inefficient Ag cross-presentation. Protein transduction domains (PTDs) ⁄cell-penetrating peptides (CPPs) are short stretches of cationic amino acids that enable peptides, proteins, oligonucleotides and other reagents efficiently to enter a variety of cell types. PTDs ⁄CPPs enter 2009 The Authors Journal Compilation 2009 British Association of Dermatologists • British Journal of Dermatology 2010 162, pp29–41 29 30 Polyarginine-containing immunogenic antigens and antitumour immunity, H. Mitsui et al. cells via macropinocytosis ⁄endocytosis after binding to anionic cell membrane components such as heparan sulphate.1–5 It has been suggested that PTDs leak into cytoplasm after macropinocytosis, depending upon the PTD concentration.6 Thus, PTDs ⁄CPPs offer a unique therapeutic opportunity for the treatment of many diseases. There are some reports on the in vivo tissue distribution of TAT-PTD ⁄cytoplasmic transduction peptide (an arginine-rich variant of TAT-PTD) fusion proteins through different routes of administration [portal vein, intravenous, intraperitoneal (i.p.) and oral].7,8 Previously, we demonstrated that polyarginine (R9)-PTD, known as the most efficacious PTD, induced more efficient protein transduction of dendritic cells (DCs) in vitro than the other PTDs studied including TAT-PTD; the R9-PTD-transduced DCs efficiently induced Ag-specific immune responses mediated by CD8+ and CD4+ T cells as well as a superior antitumour response in vivo using different model Ags.9,10 However, the clinical potential of DC therapy is limited, because the isolation and cultivation of DCs ex vivo require special facilities and materials, and the treatment expense might be too great. There are some reports that Ag-specific CTLs can be induced by using particulate carriers in vivo.11,12 If they could efficiently induce Agspecific CTLs and helper T (Th) cells, soluble protein Ags without adjuvants would be useful in terms of safety and the simplicity of preparation. There are several reports describing the additional biological effects (other than protein transduction) that are mediated by arginine ⁄arginine-rich cationic polypeptides. These cationic polypeptides act as antimicrobial reagents,13,14 leucocyte chemoattractants,14,15 inducers of substance P ⁄neurokinin-116 or bronchial hyper-responsiveness,17 and indispensable nutrients for the expressions of T-cell receptors in tumour microenvironments.18 Therefore, in the present study we intradermally injected rR9-containing ovalbumin (OVA) fusion protein (rR9-HA-OVA) as a model Ag and then investigated the resulting immune responses and performed histopathological analyses. Our results clearly demonstrate that intradermal (i.d.) injections of rR9-HA-OVA into naı̈ve mice elicited quite different Ag-specific immune responses when compared with those of rOVA without R9-PTD. Intratumoral (i.t.) injections of rR9-HA-OVA into EG.7-bearing mice elicited strong antitumour effects that were superior to those elicited by i.t. injections of rR9-OVA-treated DCs. This simple vaccination approach with R9-PTD-containing fusion proteins might be useful as prophylactic immunotherapy for cancer or infectious diseases. Materials and methods Mice and cells Six- to 8-week-old female C57BL ⁄6 mice were purchased from SLC Japan (Hamamatsu, Japan). Alymphoplasia immunodeficient mice (ALY ⁄NscJcl-aly ⁄aly; C57BL ⁄6 background) were purchased from CLEA Japan (Tokyo, Japan). All animal experiments were approved by the Institutional Review Board of the University of Yamanashi, Faculty of Medicine. EL-4 cells (murine thymoma cells) were purchased from the American Type Culture Collection (Manassas, VA, U.S.A.), and OVA cDNA stable transfectants (EG.7 cells) were provided by M. Bevan (University of Washington, Seattle, WA, U.S.A.). Cell lines were cultivated in RPMI 1640 containing 10% fetal bovine serum, glutamine and penicillin ⁄streptomycin (Invitrogen Japan, Tokyo, Japan). DCs were obtained by culturing C57BL ⁄6 bone marrow cells in RPMI 1640 containing 5% fetal bovine serum, glutamine, penicillin ⁄streptomycin (Invitrogen), murine recombinant granulocyte ⁄ macrophage colony-stimulating factor (GM-CSF) and recombinant interleukin (IL)-4 (10 ng mL)1 each; PeproTech, Rocky Hill, NJ, U.S.A.) for 5 days.9 After enrichment on 14Æ5% metrizamide gradients and overnight incubation, nonadherent and loosely adherent cells were harvested and used in experiments. Generation and characterization of recombinant protein antigens His6-tagged recombinant nona-arginine-haemagglutinin-OVA (rR9-HA-OVA), rHA-OVA, rR9-HA-GFP (green fluorescent protein) and rR9-HA-mFCRL (murine Fc receptor-like A) constructs (Fig. S1; see Supporting Information) were generated as previously described.9,10 High expression BL21 (DE3) (Novagen, Madison, WI, U.S.A.) transformants were selected after blotting lysates of transformants with anti-HA monoclonal antibody (mAb) (Covance, Richmond, CA, U.S.A.). Denatured recombinant fusion proteins were purified by sequential Ni2+ NTA-agarose chromatography, fast protein liquid ion exchange chromatography, and gel filtration chromatography as described.9 Proteins were stored at )70 C in phosphate-buffered saline (PBS) ⁄10% glycerol and thawed immediately before use. Sodium dodecyl sulphate–polyacrylamide gel electrophoresis was performed with NuPAGE 4–12% Bis-Tris gels and MOPS running buffer (Invitrogen). Endotoxin contamination of recombinant proteins was determined via Limulus lysate assay (BioWhittaker, Walkersville, MD, U.S.A.). Recombinant proteins were treated with polymyxin B sulphate (50 mg mL)1; Sigma-Aldrich, St Louis, MO, U.S.A.) before use. Reagents NH2-SIINFEKL-COOH (SIINFEKL) synthetic peptide and NH2RRRRRRRRR-COOH (R9) synthetic peptide were purchased from Qiagen (Valencia, CA, U.S.A.). Native OVA protein was purchased from Sigma-Aldrich. Complete Freund’s adjuvant (CFA) was purchased from Invitrogen. 25.D1.16 mAb reactive with SIINFEKL: H-2Kb complexes19 was provided by R. Germain (National Institute of Allergy and Infectious Disease, Bethesda, MD, U.S.A.). Mouse IgG, rat IgG and hamster IgG (isotype control), anti-Gr1 (RB6-8C5), anti-CD11b (M1 ⁄70) and anti-CD11c (HL3) mAbs were purchased from BD Pharmingen (San Diego, CA, U.S.A.). Antimouse CD8 mAb (53-6.7) 2009 The Authors Journal Compilation 2009 British Association of Dermatologists • British Journal of Dermatology 2010 162, pp29–41 Polyarginine-containing immunogenic antigens and antitumour immunity, H. Mitsui et al. 31 was purchased from eBioscience (San Diego, CA, U.S.A.). Anti-CD4 mAb (GK1.5) was provided by H. Yagita (Juntendo University, Tokyo, Japan). Analyses for R9-PTD-mediated GFP transduction in live cells For the evaluation of GFP protein transduction, DCs and EL-4 cells were incubated with rHA-GFP or rR9-HA-GFP (100 lg mL)1) in the presence of cell culture medium in 12well plates for 1–6 h at 37 C. Then, treated cells were washed twice with ice-cold PBS and analysed directly by flow cytometry (FACScan; BD Pharmingen). Treated DCs or EL-4 cells were also analysed directly using a fluorescence microscope ⁄laser scanning confocal microscope (Leitz DMRBF and Leica TCS4D; Leica, Heidelberg, Germany). Analyses for fluorescence intensities by intradermal injections of rGFPs in vivo To analyse the fluorescence intensities at the injection site after i.d. injections of rGFP proteins, naı̈ve mice were injected intradermally on the hair-shaved right flank with rR9-HA-GFP, rHA-GFP proteins (100 lg per mouse) or rHA-GFP (100 lg per mouse) mixed with synthetic R9 peptide (10 lg per mouse) (rHA-GFP + R9 peptide), and mean percentage of green fluorescence intensities after i.d. injections of rGFP in the presence of ultraviolet B were analysed by captured digital images (0, 0Æ5, 1, 2, 4 and 6 h after i.d. injections of rGFPs) with Adobe Photoshop software (Adobe Systems, Mountain View, CA, U.S.A.). Enzyme-linked immunosorbent assay for detection of anti-OVA antibodies Sera from immunized mice were collected just before they were killed. To determine the levels of anti-OVA IgG in mouse sera, 96-well flat-bottom microtitre plates were coated with 5 mg mL)1 of native OVA in 50 mmol L)1 Tris–HCl (pH 9Æ5) for 2 h and blocked with 1 mg mL)1 of skimmed milk in PBS ⁄1 mmol L)1 ethylenediamine tetraacetic acid for 2 h. Serum samples were added to the wells for 2 h.9 Horseradish peroxidase (HRP)-conjugated antimouse IgG antibody, antimouse IgG1, antimouse IgG2a, antimouse IgG2b (Jackson ImmunoResearch, West Grove, PA, U.S.A.) and a tetramethylbenzidine substrate kit (Pierce, Rockford, IL, U.S.A.) were used for detection. Absorbance at 450 nm was measured with a Powerscan HT multidetection microplate reader. Detection of cytokines from skin extracts To profile cytokine expression at Ag injection sites, skin samples (10 · 10 mm) that were pretreated for 12 h with SIINFEKL peptide (10 lg per mouse), rOVAs or rR9-HA-GFP (100 lg per mouse) by i.d. injections were homogenized, and extracts were collected. Then, multiple cytokine expression levels were detected with TransSignal mouse cytokine antibody array Ver. 1.0 (Panomics, Fremont, CA, U.S.A.). Images were collected and analysed with Adobe Photoshop software. Percentage intensity = [(experimental spot ) negative control spot) ⁄(positive control spot ) negative control spot)] · 100. Histopathological and immunohistochemical analyses Quantification of cytotoxic T lymphocytes Mice were immunized intradermally in the flank with 5 · 105 DCs that had been treated with SIINFEKL peptide (10 mmol L)1 : 1 lg mL)1 for 1 h) and with rOVAs (300 nmol L)1: 18–20 lg mL)1 for 18 h) ex vivo on day 0. Mice were also immunized intradermally in the flank with SIINFEKL peptide (10 lg per mouse) or rOVAs (100 lg per mouse) with or without 30 lL of CFA on day 0. On day 10, popliteal lymph node cells or splenocytes were harvested and restimulated in vitro with SIINFEKL peptide (1 lg mL)1) for 5 days. CTL activity was assessed on day 15 by using calcein release assays performed as previously described.9,10,20 Nonadherent effector cells were harvested from in vitro restimulation cultures. EL-4 or SIINFEKL peptide-treated EL-4 cells were labelled with calcein (Molecular Probes, Eugene, OR, U.S.A.), washed, and added to 96-well round-bottom microtitre plates with various numbers of effector cells. Plates were incubated for 2Æ5 h, supernatants were recovered, and calcein release was measured by using a Powerscan HT multidetection microplate reader (Dainippon Pharmaceutical Co., Tokyo, Japan). Percentage specific lysis = [(experimental ) spontaneous) ⁄ (maximal ) spontaneous)] · 100. Maximal lysis was achieved with 0Æ1% Triton X-100. To perform the histopathological analyses of Ag-injected skin, formaldehyde-fixed skin sections were stained with haematoxylin and eosin. Frozen skin sections were also stained with anti-HA mAb (to detect HA-containing fusion proteins) or 25.D1.16 mAb (to detect SIINFEKL: H-2Kb complexes) and with HRP-conjugated antimouse IgG. For the quantitative analyses of infiltrating cell populations at Ag injection sites, formaldehyde-fixed skin sections were stained with various antibodies (anti-Gr1 mAb, anti-CD11b mAb, anti-CD11c mAb, anti-CD4 mAb or anti-CD8 mAb), and the mean number of positive cells was counted per cellinfiltrating field (400 ·) in three independent areas. Tumour challenge study In the tumour treatment study, EG.7 or parental EL-4 cells (1 · 106) were injected intradermally into naı̈ve mice on day 0 followed by weekly injections of Ags by i.p., peritumoral or i.t. injections on days 3 and 10 with SIINFEKL peptide (10 lg per mouse), rOVAs or rR9-HA-GFP (100 lg per mouse). Tumour sizes were determined biweekly in a blinded fashion. In some experiments, EG.7-bearing mice were treated with liquid nitrogen with cotton-tip at tumour mass (cryotherapy) 2009 The Authors Journal Compilation 2009 British Association of Dermatologists • British Journal of Dermatology 2010 162, pp29–41 32 Polyarginine-containing immunogenic antigens and antitumour immunity, H. Mitsui et al. on days 3 and 10. Tumour index (in millimetres) = square root (length · width). For CD4+ and CD8+ T-cell depletion in vivo, mice received anti-CD4 (GK1.5) and ⁄or anti-CD8 (536.7) mAb or control rat IgG intraperitoneally twice (500 lg 1 day before the first immunization and 250 lg 1 day before the second immunization). Administration of anti-CD4 and ⁄or anti-CD8 mAb selectively depleted > 95% of the relevant lymphocyte subsets (assessed in the spleen 5 days after the second dose of mAb), whereas normal rat IgG had no effect (data not shown). Statistical analysis Differences between the means of the experimental groups were analysed by Student’s t-test. P < 0Æ05 was considered statistically significant. Results Production and characterization of recombinant nonaarginine-containing fusion proteins Average green fluorescence intensities (%) We previously demonstrated that rR9-PTD-containing fusion proteins (rR9-HA-OVA, rR9-HA-GFP, rR9-HA-mFCRL) (Fig. S1; see Supporting Information) could transduce bone-marrowderived DCs in vitro.9,10 These R9-PTD-mediated protein transductions were completed within 6 h (Fig. S2; see Supporting Information). Then we investigated the dynamics of fluorescence intensities at the injection area after i.d. injections of rGFPs in vivo. Our results indicated that i.d. injections of rR9-HA-GFP remained at the injection site (right flank) for a longer time, keeping higher fluorescence intensities (Fig. 1). These results indicate that i.d. injections of R9-containing protein Ags to naı̈ve mice might elicit different immune responses than those of conventional Ags. Immunological effects after intradermal injections of rR9-PTD-containing OVA Therefore, we first investigated the Ag-specific CTL activities and titres of Ag-specific IgG after immunizing naı̈ve mice with OVA Ags. SIINFEKL-specific CTL activities were elicited even by i.d. injections of rR9-HA-OVA (100 lg per mouse) alone without adjuvants against SIINFEKL-pulsed EL-4 cells (Fig. 2a), but not (nonpulsed) EL-4 cells (data not shown). In contrast, i.d. injections of synthetic SIINFEKL peptide (10 lg per mouse) alone or rHA-OVA without R9-PTD (100 lg per mouse) did not elicit detectable SIINFEKL-specifc CTL activities (Fig. 2a). Our results also demonstrate that i.d. injections of rR9-HA-OVA could elicit OVA-specific CTL activities in popliteal (sentinel) lymph nodes, but not in splenocytes (Fig. 2b). We also measured the OVA-specific IgG titres from the sera of mice immunized with OVA Ags. Titres of OVA-specific IgG were higher from mice immunized with rR9-HA-OVA alone than from mice immunized with rHA-OVA alone, or even with rR9-HA-OVA-treated DCs (Fig. 2c). We next determined the subtypes of IgG that were elicited by i.d. injections of rR9-HA-OVA. We found that IgG2 subtypes were elevated in sera from mice with rR9-HA-OVA treatment (Fig. 2d). Our results indicate that i.d. injections of rR9-HA-OVA might elicit Ag-specific CTLs and IgG2-dominant IgG production. Histopathological analyses of antigen-injected skin Naı̈ve mice that received i.d. injections of rR9-HA-OVA developed inflammation at the injection site, especially after the rR9-HA-GFP 0h rHA-GFP 120 rHA-GFP + R9 peptide 6h rR9-HA-GFP 100 80 rHA-GFP 0h 60 6h ** 40 rHA-GFP + R9 peptide 0h 20 6h 0 0 1 2 3 4 Time course (h) 5 6 Fig 1. Dynamics of fluorescence intensities at the injection site after intradermal (i.d.) injections of rGFP proteins in vivo. Naı̈ve mice were injected intradermally on the right flank with rR9-HA-GFP, rHA-GFP proteins (100 lg per mouse), or rHA-GFP (100 lg per mouse) mixed with synthetic R9 peptide (10 lg per mouse) (rHA-GFP + R9 peptide), and mean percentage of green fluorescence intensities after i.d. injections of rGFP under ultraviolet B were analysed by captured digital images (right panels: images at 0 h and 6 h after i.d. injections are shown). Results are shown as mean ± SD, and are representative of three individual experiments. **P < 0Æ01. 2009 The Authors Journal Compilation 2009 British Association of Dermatologists • British Journal of Dermatology 2010 162, pp29–41 Polyarginine-containing immunogenic antigens and antitumour immunity, H. Mitsui et al. 33 (a) rHA-OVA SIINFEKL-peptide 25 25 20 20 15 15 15 10 10 10 5 5 5 25 rR9-HA-OVA % lysis activity (SIINFEKL-EL4) Direct injection Mixture w/CFA 20 Ex-vivo treat w/DC 0 0 0 1 10 1 100 10 E/T ratio 100 1 E/T ratio (b) 35 10 100 E/T ratio 35 Popliteal LN 30 Splenocytes % lysis activity (EG.7) % lysis activity (EL-4) 30 25 20 15 10 5 25 20 15 10 5 0 0 1 10 100 1 E/T ratio 10 100 E/T ratio (c) (d) * * * * Fig 2. Immunological effects after intradermal (i.d.) injections of OVA antigens (Ags). (a) Induction of SIINFEKL-specific cytotoxic T lymphocytes (CTLs). Mice were immunized intradermally in the flank either with OVA Ags alone (SIINFEKL peptide: 10 lg per mouse, left panel; rHA-OVA protein: 100 lg per mouse, centre panel; or rR9-HA-OVA protein: 100 lg per mouse, right panel) (closed squares), with OVA Ags plus complete Freund’s adjuvant (CFA) (closed triangles), or with 5 · 105 dendritic cells (DC) that had been pretreated with OVA Ags ex vivo (SIINFEKL peptide: 1 lg mL)1 for 1 h, rOVAs: 18–20 lg mL)1 for 18 h) (closed circles) on day 0. On day 10, popliteal lymph node (LN) cells were harvested and restimulated in vitro with SIINFEKL peptide (1 lg mL)1) for 5 days. CTL reactivities with SIINFEKL-pulsed EL-4 or EL-4 cells (data not shown) were assessed on day 15. (b) i.d. injections of rR9-HA-OVA could elicit OVA-specific CTL activities at popliteal (sentinel) LNs but not splenocytes. Mice were immunized intradermally in the flank with rR9-HA-OVA (100 lg per mouse) without CFA on day 0. On day 10, popliteal LN cells or splenocytes were harvested and restimulated in vitro with mitomycin-C-pretreated (50 lg mL)1 for 45 min) EG.7 cells for 5 days. CTL reactivities with EL-4 cells or EG.7 cells were assessed on day 15 by calcein release assay. (c) Comparison of the level of anti-OVA IgG antibodies in individual mice. On days 0 and 7, mice were immunized intradermally in the flank with OVA Ags as described above. On day 21, an enzymelinked immunosorbent assay (ELISA) was performed with native OVA protein-coated plates. Sera from naı̈ve mice were used as a negative control, and sera from mice immunized with native OVA with CFA were used as positive control. *P < 0Æ05. (d) Similar ELISAs were performed with horseradish peroxidase-conjugated anti-IgG, IgG1, IgG2a and IgG2b to compare the levels of subtypes of anti-OVA antibodies. Data are representative of three individual experiments. *P < 0Æ05. Results are shown as mean ± SD. 2009 The Authors Journal Compilation 2009 British Association of Dermatologists • British Journal of Dermatology 2010 162, pp29–41 34 Polyarginine-containing immunogenic antigens and antitumour immunity, H. Mitsui et al. second immunization (upper panels of Fig. 3). We had previously never observed severe skin inflammation after injections of rR9-HA-OVA-treated DCs. We collected skin biopsies from the injection area 48 h after the second immunization at weekly intervals and performed histopathological analyses SIINFEKL (Fig. 3a–l). We found that the area injected with rR9-HAOVA was abundantly infiltrated by Gr1+ granulocytes (neutrophils), CD11b+ monocytes, and lymphocytes (both CD4+ and CD8+ T cells; Fig 3m). In contrast, the skin immunized by rHA-OVA was infiltrated by some monocytes, lymphocytes rHA-OVA rR9-HA-OVA rR9-HA-GFP (a) (b) (c) (d) (e) (f) (g) (h) (i) (j) (k) (l) 10x 400x * (m) PBS 15 SIINFEKL * rHA-OVA rR9-HA-OVA Cell number/field rR9-HA-GFP * 10 5 * 0 Gr1 CD11b CD11c CD4 CD8 Monoclonal antibodies Fig 3. Histopathological analyses of the antigen-injected skin. Naı̈ve mice were immunized in the flank with SIINFEKL peptide (10 lg per mouse), rOVAs, or rR9-HA-GFP (100 lg per mouse). After 48 h after the second immunization at a 1-week interval, skin biopsies were performed and vertical skin sections were stained with haematoxylin and eosin (a–h) and toluidine blue (i–l). Data are representative of three individual experiments. (m) The mean number of positive cells by immunohistochemical staining with monoclonal antibodies was counted per cell-infiltrating field (400 ·) at three independent areas of the same skin section. Results are shown as mean ± SD. *P < 0Æ05. PBS, phosphatebuffered saline. 2009 The Authors Journal Compilation 2009 British Association of Dermatologists • British Journal of Dermatology 2010 162, pp29–41 Polyarginine-containing immunogenic antigens and antitumour immunity, H. Mitsui et al. 35 We also investigated the cytokine profiles of the rR9-HA-OVA injection area. Skin biopsies from the Ag-injected site were homogenized, and the extracts were collected and studied with a cytokine antibody array. In contrast to the cytokine profile by rHA-OVA, i.d. injections of rR9-HA-OVA produced abundant Th1-type cytokines such as interferon (IFN)-c, IL-2 and IFN-inducible protein 10 (Fig. 4). i.d. injections of rR9HA-OVA also elicited production of G-CSF, M-CSF, GM-CSF, IL-1a and IL-4, but not of IL-5, IL-6 or IL-10. Although we used enzyme-linked immunosorbent assay to investigate IL-17 SIINFEKL 100 90 80 80 70 70 Intensity (%) 90 60 50 40 50 40 30 20 20 10 10 0 0 G-CSF M-CSF GM-CSF MIG MIP1-alpha IFN-gamma TNF-alpha IP-10 RANTES VEGF IL-1-alpha IL-2 IL-4 IL-5 IL-6 IL-10 IL-12 IL-13 30 rR9-HA-OVA 100 90 80 80 70 70 Intensity (%) 90 60 50 40 rR9-HA-GFP 60 50 40 30 30 20 20 10 10 0 0 G-CSF M-CSF GM-CSF MIG MIP1-alpha IFN-gamma TNF-alpha IP-10 RANTES VEGF IL-1-alpha IL-2 IL-4 IL-5 IL-6 IL-10 IL-12 IL-13 Intensity (%) 100 rHA-OVA 60 G-CSF M-CSF GM-CSF MIG MIP1-alpha IFN-gamma TNF-alpha IP-10 RANTES VEGF IL-1-alpha IL-2 IL-4 IL-5 IL-6 IL-10 IL-12 IL-13 Intensity (%) 100 Cytokine profiles of antigen-injected skin G-CSF M-CSF GM-CSF MIG MIP1-alpha IFN-gamma TNF-alpha IP-10 RANTES VEGF IL-1-alpha IL-2 IL-4 IL-5 IL-6 IL-10 IL-12 IL-13 (CD4+ T cells), eosinophils, and degranulated mast cells (as determined by toluidine blue staining). We also examined the skin immunized by rR9-irrelevant protein (rR9-HA-GFP). Although the types of infiltrating cells were similar to the infiltrating cells after rR9-HA-OVA injection, the magnitude of inflammation was less. The skin immunized by synthetic SIINFEKL peptide (Fig. 3a) or by synthetic R9 peptide alone (data not shown) was infiltrated by few cells. We summarized the numbers of infiltrating cells (per 400 · field) stained by mAbs in Figure 3m. These results demonstrate that i.d. injections of rR9-HA-OVA could induce severe inflammatory cell infiltration at injected skin tissue. Fig 4. Intradermal injections of rR9-HA-OVA elicit a Th1 cytokine profile at the injection area. Naı̈ve mice were immunized in the flank with SIINFEKL peptide (10 lg per mouse), rOVAs, or rR9-HA-GFP (100 lg per mouse). Twelve hours after antigen injections, skin samples were collected and homogenized, and then the extracts were collected. The expression of multiple cytokines was detected with the TransSignal mouse cytokine antibody array, and images were analysed with Adobe Photoshop software. Percentage intensity = [(experimental spot ) negative control spot) ⁄ (positive control spot ) negative control spot)] · 100. Data are shown as mean ± SD, and are representative of two individual experiments. 2009 The Authors Journal Compilation 2009 British Association of Dermatologists • British Journal of Dermatology 2010 162, pp29–41 36 Polyarginine-containing immunogenic antigens and antitumour immunity, H. Mitsui et al. and IL-23 cytokine production, neither of these cytokines was detected in skin extracts (data not shown). These results and the results in Figure 2d (IgG2-dominant OVA-specific antibody production) indicate that i.d. injections of rR9-HA-OVA elicit strong immune responses, especially Th1-dominant immune responses, in the area of the injected skin. Expression of antigen epitopes on major histocompatibility complex class I at the antigen-injected area Our preliminary data demonstrated that i.d. injections of rR9-HA-GFP could stay at the injection area for a long time, keeping high fluorescence intensities (Fig. 1). These results indicate that rR9-HA-OVA could be transduced into injected dermal tissue such as fibroblasts. Our present results demonstrate that high levels of IFN-c were secreted in the injection area (Fig. 4). Previously, we also demonstrated that high levels of the SIINFEKL epitope were presented on the MHC class I molecules of PTD-OVA-transduced EL-4 cells in vitro upon IFN-c treatment;20 this high level of presentation was presumably caused by the induction of immunoproteasomes and the upregulation of MHC class I. All these data indicate that the SIINFEKL epitope might be presented on MHC class I molecules of dermal cells by transduction and processing of rR9-HA-OVA in vivo. To investigate this hypothesis, skin sections from areas injected with OVA-Ags were immunostained with 25.D1.16 mAb, which recognizes only SIINFEKL: H-2Kb complexes.19 rR9-HA- SIINFEKL OVA still remained at the local injection area after 48 h, as detected by anti-HA mAb (Fig. 5c). Interestingly, SIINFEKL: H-2Kb complexes were detected only in skin injected with rR9-HA-OVA (Fig. 5g, k), but not in skin injected with the synthetic SIINFEKL peptide (Fig. 5e, i). Microscopic analyses of skin injected with rR9-HA-OVA demonstrated that 25.D1.16positive cells were dermal fibroblasts, endothelial cells and infiltrated inflammatory cells (Fig. S3; see Supporting Information). However, we could not determine which types of inflammatory cells expressed the SIINFEKL epitope. In contrast, the staining intensities with 25.D1.16 mAb were minimal in skin injected with rHA-OVA (Fig. 5f, j). These results indicate that the whole area intradermally injected with rR9-HA-OVA might be targeted by induced OVA-specific CTLs. Treatment of EG.7-bearing animals with rR9-HA-OVA Next, we performed an EG.7 treatment study. First, EG.7-bearing mice were immunized on days 3 and 10 by rR9-HA-OVA in different injection areas and by different routes, and we compared the antitumour effects. The i.t. injections with rR9HA-OVA elicited superior antitumour effects than injections in any other area (Fig. 6a). Next, to identify the minimal dose needed for the maximal antitumour effect, the antitumour effects of different doses of rR9-HA-OVA injections were compared. We found that i.t. injections of 100 lg of rR9-HAOVA per mouse optimally suppressed EG.7 tumour growth (Fig. 6b). Next, we compared the antitumour effects elicited rHA-OVA rR9-HA-OVA rR9-HA-GFP (a) (b) (c) (d) (e) (f) (g) (h) (i) (j) (k) (l) Fig 5. rR9-HA-OVA stayed longer at the injection area, and the SIINFEKL epitope was expressed on major histocompatibility complex class I molecules in the same area. Naı̈ve mice were immunized in the flank with SIINFEKL peptide (10 lg per mouse), rOVAs, or rR9-HA-GFP (100 lg per mouse). Forty-eight hours after antigen injections, skin samples were collected, and vertical skin sections were stained with anti-HA monoclonal antibody (mAb) (a–d) (original magnification · 10) or with 25.D1.16 mAb (e–l) (original magnification · 10 and · 400). These skin sections were not stained by isotype control IgG (data not shown). Data are representative of at least two individual experiments. 2009 The Authors Journal Compilation 2009 British Association of Dermatologists • British Journal of Dermatology 2010 162, pp29–41 Polyarginine-containing immunogenic antigens and antitumour immunity, H. Mitsui et al. 37 (a) 25 (b) 25 Untreated rR9-HA-GFP Intratumoral (20) 20 SIINFEKL Tumor index (mm) Intratumoral 15 10 5 Intratumoral (100) 20 Intratumoral (500) 15 10 * Tumor index (mm) Peritumoral Tumor index (mm) Untreated I.D. (opposite flank) 20 5 0 0 5 10 15 20 0 25 (d) 0 10 rR9-HA-OVA DC-rR9-HA-GFP 15 DC-rR9-HA-OVA 10 ** * 15 20 0 25 0 5 10 15 20 Days after EG.7 challenge Aly/Aly mice (e) 30 Untreated rR9-HA-OVA + anti-CD4 mAb rR9-HA-GFP 25 rR9-HA-OVA + anti-CD8 mAb rHA-OVA rR9-HA-OVA + anti-CD4, CD8 mAb rR9-HA-OVA Tumor index (mm) 20 5 Days after EG.7 challenge Untreated rR9-HA-OVA + isotype 25 rHA-OVA 5 Days after EG.7 challenge Tumor index (mm) (c) 25 Untreated I.P. 15 10 5 20 rR9-HA-OVA (I.P.) 15 10 5 0 0 0 5 10 15 20 Days after EG.7 challenge 25 0 5 10 15 20 25 Days after EG.7 challenge Fig 6. Antitumour effects mediated by intratumoral injections of rR9-HA-OVA in EG.7-bearing mice. EG.7 cells (1 · 106) were injected intradermally into naı̈ve mice (a–d) or Aly ⁄ Aly mice (e) on day 0 followed by two weekly injections of antigens by intraperitoneal (a), peritumoral (a) or intratumoral (a–e) injections on days 3 and 10. (a) rR9-HA-OVA (100 lg per mouse) was injected intraperitoneally (I.P.), intradermally (I.D.), peritumorally or intratumorally (five mice per group). (b) rR9-HA-OVA was injected intratumorally at different doses (20, 100 or 500 lg per mouse) (five mice per group). (c) Different antigens or antigen-treated dendritic cells were injected intratumorally (five mice per group). (d) rR9-HA-OVA was injected intratumorally on days 3 and 10. Mice also received anti-CD4 (GK1.5) and ⁄ or anti-CD8 (53-6.7) monoclonal antibody (mAb) or control rat IgG intraperitoneally on day 2 (500 lg per mouse) and day 9 (250 lg per mouse) (five mice per group). (e) Antigens were injected intratumorally or intraperitoneally into EG.7-bearing alymphoplastic Aly ⁄ Aly mice (five mice per group). Tumour index (in millimetres) = square root (length · width). Data are shown as mean ± SD, and are representative of at least two individual experiments. *P < 0Æ05, **P < 0Æ01. by i.t. injections of different OVA-Ags (Fig. 6c). Among the Ags tested, which included rR9-HA-OVA-treated DCs (DCrR9-HA-OVA) and cryotherapy with liquid nitrogen, rR9-HAOVA mediated the greatest antitumour effects (Table 1). We also performed an EG.7-rechallenge study with EG.7-rejected mice. All EG.7-rejected mice completely rejected a second challenge with EG.7 cells (1 · 106 per mouse) (15 of 15) and survived more than 100 days after the rechallenge (data not shown). We also performed treatment studies with CD4+ ⁄CD8+ cell-depletion antibodies to investigate whether the antitumour effects were mediated by T cells. We found that the effects of i.t. injections of rR9-HA-OVA were completely dependent on CD8+ T cells (Fig. 6d). Interestingly, the antitumour effects mediated by rR9-HA-OVA were partially suppressed with depletion of CD4+ cells, and the boosting antitumour effects after the second injection were diminished. We confirmed that i.t. injections of rR9-HA-OVA were not cytotoxic to the tissue ⁄tumour cells in alymphoplastic immunodeficient mice (Aly ⁄Aly; C57BL6 background) (Fig. 6e). These results indicate that antitumour effects against EG.7 cells by i.t. injections of rR9-HA-OVA were directly mediated by CD8+ CTLs, and CD4+ T cells supported their activities. Antitumour effects against parental EL-4-tumour-bearing animals with rR9-HA-OVA Our present data indicate that i.d. injections of rR9-HA-OVA in vivo elicited dual immunological effects. One effect is the induction of Tc1- and Th1-dominant immune responses, and the other effect is the induction of inflammatory responses in the injection area due to the expression of Ag epitopes on 2009 The Authors Journal Compilation 2009 British Association of Dermatologists • British Journal of Dermatology 2010 162, pp29–41 38 Polyarginine-containing immunogenic antigens and antitumour immunity, H. Mitsui et al. Table 1 Summary of tumour-free survival and tumour burden after intratumoral injections of peptides, proteins or antigen-transduced dendritic cells (DCs). EG.7-bearing mice were also treated with liquid nitrogen at tumour mass with cotton-tip (cryotherapy; group N) on days 3 and 10 Tumour-free mice Immunogen A: Untreated B: SIINFEKL peptide C: R9 peptide D: rR9-HA-GFP E: rR9-HA-mFCRL F: Native OVA protein G: rHA-OVA H: rHA-OVA + R9 peptide I: rR9-HA-OVA J: DC-rR9-HA-OVA K: DC-rR9-HA-GFP L: rHA-OVA (opposite flank) M: rR9-HA-OVA (opposite flank) N: Liquid nitrogen (cryotherapy) Tumour burden (mm) 0 ⁄ 25 0 ⁄ 10 0 ⁄5 2 ⁄ 20 (10%) 0 ⁄ 10 2 ⁄ 10 (20%) 5 ⁄ 19 (26%) 1 ⁄ 5 (20%) 20Æ00 20Æ33 17Æ16 15Æ33 16Æ58 9Æ22 8Æ90 11Æ39 ± ± ± ± ± ± ± ± 2Æ86 2Æ65 3Æ57 8Æ67 3Æ97 6Æ19 6Æ94 7Æ43 19 ⁄ 25 (76%) 6 ⁄ 10 (60%) 0 ⁄ 10 0 ⁄5 2Æ78 6Æ84 18Æ52 14Æ86 ± ± ± ± 5Æ16 9Æ17 2Æ24 3Æ44 0 ⁄5 12Æ92 ± 2Æ05 0 ⁄5 18Æ78 ± 1Æ97 Discussion Data from five individual treatment studies (using the same protocol as described in Fig. 6) were pooled (day 22–25 data reported). Tumour burdens represent the mean ± SD tumour indices (square root of the product of horizontal and vertical dimensions). E vs. G, P = 0Æ028; E vs. I, P < 0Æ001; G vs. I, P = 0Æ0033. MHC class I molecules as targets. Previously, we demonstrated that PTD-containing OVA could be transduced into EL-4 cells (parental cells of EG.7 that do not express OVA) in vitro and that PTD-containing OVA-treated EL-4 cells were lysed by OVA-specific CTLs in vitro.20 We next compared the antitumour effects against EG.7 and parental EL-4 cells mediated by i.t. injections of fusion proteins. i.t. injections of rR9-HA- (a) 25 Untreated (b) rHA-OVA 25 OVA suppressed both EG.7 and EL-4 tumour growth (Fig. 7), but EL-4 tumour masses did progress after the injections were discontinued (Fig. 7b). The expression levels of H-2Kb on EG.7 and EL-4 cells were almost identical, and both cell lines grew progressively in the same way in C57BL ⁄6 mice (data not shown). Finally, we investigated that the SIINFEKL epitope was presented on MHC class I molecules of tumour cells by transduction and processing of rR9-HA-OVA in vivo by i.t. injection. Skin sections from tumour areas injected with OVAAgs were immunostained with anti-HA mAb or 25.D1.16 mAb (Fig. 8). rR9-HA-OVA still remained at the local injection area after 48 h as detected by anti-HA mAb (Fig. 8f, i), and SIINFEKL: H-2Kb complexes were also detected on the (EL-4) tumour cells (Fig. 8o). Thus, rR9-HA-OVA might be transduced into EG.7 ⁄EL-4 cells in vivo by i.t. injections. However, the expression levels of OVA might be transient in EL-4 cells due to protein degradation and ⁄or cell proliferation. Our results demonstrate that i.d. injections of R9-PTD-containing immunogenic protein Ags in vivo simultaneously induced dual immunological effects (induction of Ag-specific immune responses and induction of Th1-dominant inflammation at the injection area). We have not analysed in detail the mechanism by which i.d. injections of rR9-containing Ags induce Ag-specific Tc1- and Th1-mediated immune responses. However, the sentinel lymph nodes might be crucial for these responses, as i.d. injections of rR9-HA-OVA elicited little antitumour effects in alymphoplastic (Aly ⁄Aly) mice (Fig. 6e), and the antitumour effects mediated by i.d. injections at the opposite site were inferior (Fig. 6a). Moreover, OVA-specific CTL activities were detected in sentinel lymph nodes but were minimal in splenocytes (Fig. 2b). Our results demonstrate that this simple and economical vaccination approach elicited superior antitumour effects than DC-based immunotherapy alone (Fig. 6c, Table 1). The superior antitumour effects mediated by direct injection of rR9-HA-OVA might be partly due to the adjuvant effects of Untreated rHA-OVA rR9-HA-OVA Tumor index (mm) rR9-HA-OVA rR9-HA-GFP 20 20 rR9-HA-GFP rR9-HA-mFCRL 15 15 10 10 ** 5 ** 5 0 0 0 5 10 15 20 Days after EG.7 challenge 25 0 5 10 15 20 Days after EL-4 challenge 25 Fig 7. Antitumour effects mediated by intratumoral injections of rR9-HA-OVA in EG.7- or EL-4-bearing mice. OVA-expressing EG.7 (a) or parental EL-4 (b) cells (1 · 106) were injected intradermally into naı̈ve mice (five mice per group) on day 0, followed by two weekly intratumoral injections of antigens (100 lg per mouse) on days 3 and 10. Data are shown as mean ± SD, and are representative of three individual experiments. **P < 0Æ01. 2009 The Authors Journal Compilation 2009 British Association of Dermatologists • British Journal of Dermatology 2010 162, pp29–41 Polyarginine-containing immunogenic antigens and antitumour immunity, H. Mitsui et al. 39 Untreated rHA-OVA rR9-HA-OVA (b) (c) (d) (e) (f) (g) (h) (i) (j) (k) (l) (m) (n) (o) 25.D1.16 mAb. Anti-HA mAb H&E (a) Fig 8. Histopathological analyses of the rOVA-injected skin in EL-4-bearing mice. (Parental) EL-4 cells (1 · 106) were injected intradermally into naı̈ve mice on day 0. EL-4-bearing mice were immunized by weekly injections of rOVAs (rHA-OVA, rR9-HA-OVA) by intratumoral injections on days 3 and 10. Forty-eight hours after the second immunization, skin biopsies were performed and vertical skin sections were stained with haematoxylin and eosin (a–c), anti-HA monoclonal antibody (mAb) (d–i) or 25.D1.16 mAb (j–o) (original magnification · 10 and · 400). These skin sections were not stained by isotype control IgG (data not shown). Data are representative of at least two individual experiments. arginine-rich cationic proteins. Recently, it was demonstrated that F4 ⁄80+ tumour-associated macrophages (TAM) of EL-4bearing mice inhibited T-cell-mediated immune responses via induction of T-cell apoptosis through TAM-producing arginase and NO.21 Another study found that the success of immunotherapy by CTLs against established tumours might be dependent upon the destruction of (CD11b+) tumour stromal cells, which are produced by the host-cancer interaction.22 Therefore, the antitumour effects mediated by i.t. injections of rR9-containing Ags themselves, which are superior to the effects of Ag-treated DCs ex vivo (Fig. 6c), might be due to higher killing activities against tumour stromal cells by the transduction of Ags into those cells and by the expression of Ag epitopes on MHC class I molecules. 2009 The Authors Journal Compilation 2009 British Association of Dermatologists • British Journal of Dermatology 2010 162, pp29–41 40 Polyarginine-containing immunogenic antigens and antitumour immunity, H. Mitsui et al. We recently reported that autoantigen Fc receptor-like A (FCRLA), which is specifically expressed in melanocytes, melanoma cells and some B-cell states (Epstein–Barr virus-transformed B cells, germinal centre centroblasts and diffuse large B-cell lymphoma),23 could be useful as a shared target Ag in immunotherapy for B-cell malignancies.10 We are currently investigating the enhancement of the antitumour effects caused by direct injections of rR9-HA-mFCRL with A20 B-cell lymphoma cells and B16 melanoma cells, as it is difficult to break the immunological tolerance by using conventional autoantigens. Temporary but superior antitumour effects against parental EL-4 cells by i.t. injections of rR9-HA-OVA (Fig. 7b), but not by (less immunogenic) rR9-HA-GFP, may indicate that i.t. injections of rR9-containing immunogenic foreign Ags might be a unique and attractive immunotherapeutic approach for cancer treatment. Similar antitumour effects against EL-4 tumour mass were also observed by i.t. injections of another rR9-PTD-containing immunogenic foreign Ag (Leishmania Ag; LACK24) (our unpublished observation). Previously, several types of tumour cells stably transfected with OVA cDNA (EL-4 thymoma, A20 B-cell lymphoma, B16 melanoma) were utilized with OVA as a model tumour-associated Ag,25–32 as immune tolerance might be less inducible in immunogenic foreign Ags. We are also investigating the unique immunotherapeutic approaches provided by i.t. injections of rR9-HAOVA against A20 and B16 cells; we expect to observe the induction of tumour-specific immune responses such as epitope spreading. Our present results demonstrate that R9-PTD-containing proteins stayed for a long time at the injection area when injected intradermally (Fig. 1), and they transduced into local tissue cells. In contrast to rR9-HA-OVA, i.d. injections of the less immunogenic rR9-HA-GFP elicited less inflammation at the injection area (Figs 3d and 5d). These results indicate that in vivo application of R9-PTD-containing fusion molecules to local skin lesions might be useful as a novel cell-transduction approach for molecular-targeting therapies that could deliver medicines locally without major systemic side-effects. In summary, this simple approach may lead to unique therapies that provide important clinical benefits to patients. Acknowledgments This work was supported by a grant from the Ministry of Education and Science of the Japanese Government (no. 18591241). References 1 Chauhan A, Tikoo A, Kapur AK et al. The taming of the cell penetrating domain of the HIV tat: myths and realities. J Control Release 2007; 117:148–62. 2 Patel LN, Zaro JL, Shen W-C. Cell penetrating peptides: intracellular pathways and pharmaceutical perspectives. Pharm Res 2007; 24:1977–92. 3 Goun EA, Pillow TH, Jones LR et al. Molecular transporters: synthesis of oligoguanidinium transporters and their application to drug delivery and real-time imaging. ChemBioChem 2006; 7:1497–515. 4 Wadia JS, Dowdy SF. Transmembrane delivery of protein and peptide drugs by TAT-mediated transduction in the treatment of cancer. Adv Drug Deliv Rev 2005; 57:579–96. 5 Kaplan IM, Wadia JS, Dowdy SF. Cationic TAT peptide transduction domain enters cells by macropinocytosis. J Control Release 2005; 102:247–53. 6 Fuchs SM, Raines RT. Pathway for polyarginine entry into mammalian cells. Biochemistry 2004; 43:2438–44. 7 Cai S-R, Xu G, Becker-Hapak M et al. The kinetics and tissue distribution of protin transduction in mice. Eur J Pharm Sci 2006; 27:311–19. 8 Kim D, Jeon C, Kim J-H et al. Cytoplasmic transduction peptide (CTP): new approach for the delivery of biomolecules into cytoplasm in vitro and in vivo. Exp Cell Res 2006; 312:1277–88. 9 Mitsui H, Inozume T, Kitamura R et al. Polyarginine-mediated protein delivery to dendritic cells presents antigen more efficiently onto MHC class I and class II and elicits superior antitumor immunity. J Invest Dermatol 2006; 126:1804–12. 10 Inozume T, Mitsui H, Okamoto T et al. Dendritic cells transduced with autoantigen FCRLA induce cytotoxic lymphocytes and vaccinate against murine B-cell lymphoma. J Invest Dermatol 2007; 127:2818–22. 11 Ikegawa T, Yamasaki Y, Shakushiro K et al. Induction of cytotoxic T lymphocytes following immunization with cationized soluble antigen. Vaccine 2004; 22:2609–16. 12 Yamasaki Y, Ikenaga T, Otsuki T et al. Induction of antigen-specific cytotoxic T lymphocytes by immunization with negatively charged soluble antigen through scavenger receptor-mediated delivery. Vaccine 2007; 25:85–91. 13 Reddy KVR, Yedery RD, Aranha C. Antimicrobial peptides: premises and promises. Int J Antimicrob Agents 2004; 24:536–47. 14 Bhat S, Milner S. Antimicrobial peptides in burns and wounds. Curr Protein Pept Sci 2007; 8:506–20. 15 Djanani A, Mosheimer B, Kaneider NC et al. Heparan sulfate proteoglycan-dependent neutrophil chemotaxis toward PR-39 cathelicidin. J Inflamm (Lond) 2006; 3:14. 16 Coyle AJ, Perretti F, Manzini S et al. Cationic protein-induced sensory nerve activation: role of substance P in airway hyperresponsiveness and plasma protein extravasation. J Clin Invest 1994; 94:2301–6. 17 Madison JM, Schramm CM. Cationic proteins and bronchial hyperresponsiveness. Am J Respir Cell Mol Biol 2000; 22:513–16. 18 Rodriguez PC, Quiceno DG, Zabaleta J et al. Arginase I production in the tumor microenvironment by mature myeloid cells inhibits T-cell receptor expression and antigen-specific T-cell responses. Cancer Res 2004; 64:5839–49. 19 Porgador A, Yewdell JW, Deng Y et al. Localization, quantitation, and in situ detection of specific peptide-MHC class I complexes using a monoclonal antibody. Immunity 1997; 6:715–26. 20 Shibagaki N, Udey MC. Dendritic cells transduced with protein antigens induce cytotoxic lymphocytes and elicit antitumor immunity. J Immunol 2002; 168:2393–401. 21 Kusmartsev S, Gabrilovich DI. STAT1 signaling regulates tumor-associated macrophage-mediated T cell deletion. J Immunol 2005; 174:4880–91. 22 Zhang B, Bowerman NA, Salama JK et al. Induced sensitization of tumor stroma leads to eradication of established cancer by T cells. J Exp Med 2007; 204:49–55. 23 Inozume T, Matsuzaki Y, Kurihara S et al. Novel melanoma antigen, FCRL ⁄ FREB, identified by cDNA profile comparison using DNA 2009 The Authors Journal Compilation 2009 British Association of Dermatologists • British Journal of Dermatology 2010 162, pp29–41 Polyarginine-containing immunogenic antigens and antitumour immunity, H. Mitsui et al. 41 24 25 26 27 28 29 30 chip are immunogenic in multiple melanoma patients. Int J Cancer 2005; 114:283–90. Mendez S, Gurunathan S, Kamhawi S et al. The potency and durability of DNA-, and protein-based vaccines against Leishmania major evaluated using low-dose, intradermal challenge. J Immunol 2001; 166:5122–8. Moore MW, Carbone FR, Bevan MJ. Introduction of soluble protein into the class I pathway of antigen processing and presentation. Cell 1988; 54:777–85. Nishimura T, Iwakabe K, Sekimoto M et al. Distinct role of antigenspecific T helper type 1 (Th1) and Th2 in tumor eradication in vivo. J Exp Med 1999; 190:617–27. Brockstedt DG, Podsakoff GM, Fong L et al. Induction of immunity to antigens expressed by recombinant adeno-associated virus depends on the route of administration. Clin Immunol 1999; 92:67– 75. Dobrzanski MJ, Reome JB, Dutton RW. Type 1 and type 2 CD8+ effector T cell subpopulations promote long-term tumor immunity and protection to progressively growing tumor. J Immunol 2000; 164:916–25. Bellone M, Cantarella D, Castiglioni P et al. Relevance of the tumor antigen in the validation of three vaccination strategies for melanoma. J Immunol 2000; 165:2651–6. Sato M, Chamoto K, Nishimura T. A novel tumor-vaccine cell therapy using bone marrow-derived dendritic cell type 1 and antigenspecific Th1 cells. Int Immunol 2003; 15:837–43. 31 Chamoto K, Tsujji T, Funamoto H et al. Potentiation of tumor eradication by adoptive immunotherapy with T-cell receptor genetransduced T-helper type 1 cells. Cancer Res 2004; 64:386–90. 32 van Broekhoven CL, Parish CR, Demangel C et al. Targeting dendritic cells with antigen-containing liposome: a highly effective procedure for induction of antitumor immunity and for tumor immunotherapy. Cancer Res 2004; 64:4357–65. Supporting Information Additional Supporting Information may be found in the online version of this article: Fig S1. Amino acid sequence of nona-arginine (R9)-PTD and schematic representation of recombinant fusion proteins and OVA antigens. Fig S2. Flow cytometric analyses of rGFP-treated live cells in vitro. Fig S3. Histopathological analyses of 25.D1.16-positive cells at rR9-HA-OVA injection area. Please note: Wiley-Blackwell are not responsible for the content or functionality of any supporting materials supplied by the authors. Any queries (other than missing material) should be directed to the corresponding author for the article. 2009 The Authors Journal Compilation 2009 British Association of Dermatologists • British Journal of Dermatology 2010 162, pp29–41