Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
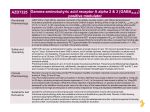
Polysubstance dependence wikipedia , lookup
Cannabinoid receptor antagonist wikipedia , lookup
Psychopharmacology wikipedia , lookup
Discovery and development of angiotensin receptor blockers wikipedia , lookup
Compounding wikipedia , lookup
NK1 receptor antagonist wikipedia , lookup
Nicotinic agonist wikipedia , lookup
Plateau principle wikipedia , lookup
Pharmacognosy wikipedia , lookup
Pharmaceutical industry wikipedia , lookup
List of comic book drugs wikipedia , lookup
Prescription costs wikipedia , lookup
Pharmacogenomics wikipedia , lookup
Prescription drug prices in the United States wikipedia , lookup
Drug interaction wikipedia , lookup
Neuropsychopharmacology wikipedia , lookup
Drug design wikipedia , lookup
Drug discovery wikipedia , lookup
Theralizumab wikipedia , lookup
Farmacología Clínica
{
Dr. Carlos Fernando Estrada Garzona
Departamento de Farmacología
Universidad de Costa Rica
Ñ
PRINCIPIOS DE FARMACOCINETICA CLINICA
Ó
Ñ
ESTADO ESTACIONARIO
PRINCIPIOS DE FARMACODINAMIA
Ó
EFICACIA CLINICA DE MEDICAMENTOS
OBJETIVOS
FARMACOCINETICA
stained steady-state effective concentration of drugs in the fluids bath
1. Overview of pharmacology. Pharmacokinetics (PK) relates to the effect of the body o
and principally includes bioavailability, distribution,
and clearance. Pharmacodyna
Clin Lab Med 28 (2008) 485–497
relates to drug concentration and receptor availability. The response to drug concentra
be therapeutic, subtherapeutic, or toxic, depending on considerations involving both PK
principles. (From Linder MW, Valdes R Jr. Pharmacogenetics: fundamentals and app
it has also been shown that clinical responses can be predicted and the peak/
MIC ratio by measuring the antibiotic’s AUC over the dosing interval and
dividing that value by its MIC against the target organism [3]. In essence,
Peak/MIC (Concentration-Dependent)
Concentration
AUC/MIC
Time > MIC (Time-Dependent)
MIC
0
Time (Hours)
Fig. 1. Pharmacokinetic and pharmacodynamic parameters affecting antibiotic potency. AUC,
area under the curve; MIC, minimum inhibitory concentration.
Crit Care Clin 24 (2008) 335–348
Drug
c=
˜ Vapp
x
of Pharmacy
1Institute
x (e-k1t-e-k2t)
Memorial University of
Newfoundland
St. John’s, Newfoundland
Canada
Time (t)
of Bonn
k2 -University
k1
Germany
A. Time course of drug concentration
Drug concentration in blood (c)
164 color plates by Jürgen Wirth
Intravenous
Intramuscular
Subcutaneous
Oral
Time (t)
B. Mode of application and time course of drug concentration
Thieme
Stuttgart · New York · 2000
Lüllmann, Color Atlas of Pharmacology © 2000 Thieme
Lüllmann, Color Atlas of Pharmacology
© 2000
Thieme
All rights reserved.
Usage
subject to terms and conditions of licens
All rights reserved. Usage subject to terms and conditions of license.
Ñ
Velocidad à C max
Ñ
f absoluta = AUC ev / AUC iv
Ñ
f
Ñ
Bioequivalencia farmacocinética = + 20%
Ñ
y t máx
relativa = AUC ev / AUC ref
Bioequivalencia terapéutica =
Ó EFICACIA + TOLERABILIDAD
Biodisponibilidad
Ñ
FISIOLOGICOS
Ó
Ó
Ñ
PATOLOGICOS
Ó
Ó
Ñ
NEONATO-AM-EMBARAZO
VACIAMIENTO GÁSTRICO
TGI
HEPATICO
IATROGENICOS
Ó
Ó
FÁRMACOS
CYP
ABSORCIÓN
Institute of Pharmacy
University of Bonn
Germany
Memorial University of
Newfoundland
St. John’s, Newfoundland
Distribution in the Body
31
Canada
Drug is
not bound
to plasma
proteins
Drug is
strongly
bound to
plasma
proteins
164 color plates by Jürgen Wirth
Effect
Effect
Effector cell
Effector cell
Plasma
Biotransformation
Biotransformation
Renal elimination
Renal elimination
concentration
Plasma
Free drug
concentration
Bound drug
Free drug
Time
Thieme
Stuttgart · New York · 2000
Time
A. Importance of protein binding for intensity and duration of drug effect
Lüllmann, Color Atlas of Pharmacology © 2000 Thieme
All rights reserved. Usage subject to terms and conditions of licens
Lüllmann, Color Atlas of Pharmacology © 2000 Thieme
All rights reserved. Usage subject to terms and conditions of license.
Ñ
Concentración máxima / C máx
Ó
Ñ
Obesidad vs LEC aumentado
Ó
Ñ
Dosis de carga vs dosis
mantenimiento
Liposoluble / hidrosoluble
Unión a proteínas plasmáticas
DISTRIBUCIÓN
Institute of Pharmacy
Memorial University of
University of Bonn Pharmacokinetics Newfoundland
45
Germany
St. John’s, Newfoundland
Canada
Concentration (c) of drug in plasma [amount/vol]
Co
164 color plates by Jürgen Wirth
Plasma half life t 1
1
c t 1 = — co
2
2
ln 2
t 1 = —–
2
k
2
ct = co · e-kt
ct: Drug concentration at time t
co: Initial drug concentration after
administration of drug dose
e: Base of natural logarithm
k: Elimination constant
Unit of time
Time (t)
Thieme
Stuttgart · New York · 2000
Lüllmann, Color Atlas of Pharmacology © 2000 Thieme
All rights reserved. Usage subject to terms and conditions of licens
Notional plasma volume per unit of time freed of drug = clearance [vol/t]
Ñ
FISIOLOGICOS
Ó
Ñ
PATOLOGICOS
Ó
Ó
Ñ
EDAD-SEXO-EMBARAZO-EJERCICIO
RENAL-HEPATICO-CARDIACO
TABAQUISMO
IATROGENICOS
Ó
Ó
INDUCCIÓN-INHIBICION ENZIMÁTICA
pH URINARIO
ELIMINACION
tained by dose rate, bioavailability (f), and clearance (Cl) of the drug (see
Fig. 2). The catalytic activity of drug metabolizing enzymes (DMEs) is the
Fig. 2. Dose rate (D) and frequency of dose administration (t) determined by physician based
on the patient bioavailability (f) and clearance (Cl) to accomplish steady-state serum drug concentration. Abbreviation: Css, steady state serum drug concentration.
Clin Lab Med 28 (2008) 485–497
Dose
ship was Loading
defined previously
in Eq
the desired target concentration:
The loading dose is one or a
the aim of (Equation
achieving 2–1
the
the loading dose is
If the clinician chooses the desired
A
lo
ance and bioavailability for that d
steady
state
by
the
admin
dosing interval can be calculated.
long relative to the tempo
Examplet1/2 of lidocaine is usually
Goodman and Gilman'ʹs The Pharmacological Basis of Therapeutics, Twelfth Edition, 2011
Fig. 3. Pharmacodynamics of drug response. (A) Relationship be
tors and drug response, where 1A is a low number, and 1B is a hi
Relationship of drug response to affinity of receptors, where 2A
and 2B is low affinity. The 50% effective drug concentration C2A is
ceptor compared with concentration C2B. (From Weber W. Human
M, Harper PS, Scriver C, et al, editors. Pharamcogenetics. New Yo
1997. p. 28; with permission.)
FARMACODINAMIA
Review
(f) Receptor dimerization
TRENDS in Pharmacological Sciences
Vol.25 No.4 April 2004
25-year receptor revolution
(a) Spontaneously occurring
active states
New mechanisms
of signaling
Ri (inactive)
Constitutive activity,
inverse agonism
Ra (active state 1)
(e) Allosterism
Drug-like
molecules for
peptide receptors
(b) G-protein pleiotropy
G
Ra (active state 2)
(d) Auxiliary coupling
proteins
(i.e. RAMPs, RCP)
Organ-selective and
ligand-selective
agonists
(c) Agonist-selective
active states
G
• Tissue-directed
recombinant screening
• Phenotypic versus genotypic
organ selectivity
TRENDS in Pharmacological Sciences Vol.25 No.4 April 2004
TRENDS in Pharmacological Sciences
Figure 4. Discoveries of G-protein-coupled receptor (GPCR) behavior through biochemical research conducted during the past 25 years. See the main text for specific de
and examples. Abbreviations: RAMPs, receptor activity-modifying proteins; RCP, receptor component protein.
efficacy in compounds. It is given by the upper asymp
the concentration/response curve and is, therefore, rel
100
% response/binding
100
75
50
25
0
75
response (agonist A)
response (agonist B)
50
binding (agonist A/B)
25
0
-11 -10 -9 -8 -7 -6 -5 -4 -3 -2 -1
-12 -11 -10 -9 -8 -7 -6 -5 -4 -3 -2 -1
log [agonist] M
log [agonist] ( M )
100
% response
% maximal response
efinition of the efficacy of a candidate drug is required.
Many drugs are, however, antagonists, that is, compounds
75
A
British Journal ofagonist
Pharmacology
(2008) 153, 1353–1363
50
& 2008 Nature Publishing
agonist B Group All rights reserved 0007–1188/0
www.brjpharmacol.org
25
b2-Adrenoceptor reserve on human airways
MA Giembycz
A
B
Salbutamol
100
100
N = 11
Relaxation
(% Maximum)
N=8
75
75
50
50
25
25
Inactivation
Comparative
0
0
C
100
Terbutaline
25
50
75
Inactiv
Compa
0
100
0
25
50
D (2009), 158, 287–299
British Journal of Pharmacology
© 2009 The Author
Procaterol
Formoterol
100British Pharmacological Society
Journal compilation © 2009 The
KB´/α
2007.47:1-51. Downloaded from www.annualreviews.org
I on 12/01/10. For personal use only.
KA/α
the
nt
ing
ativity
eric
hosteric
ns were
ation 6.
etween
ctional
t
binding
igand
the ratio
s affinity
ite alone
A
P
a
KB´
b
1.0
0.5
L
P
Alllosteric
1
D
an
U
KB
KA
binding [A*]
alent
both
losteric
eric
dicated
Orthosteric
Annu. Rev. Pharmacol. Toxicol. 2007. 47:1–51
α =as 300
First published online
a Review in Advance on
September 29, 2006
α = 100
The Annual Review of Pharmacology and Toxicology is
K
d
A
A.N. Bateson / Sleep Medicine 5 Suppl. 1 (2004) S9–S15
Loreclezole/
Etomidate
GABA
GABA
Barbiturates?
Steroids?
Avermectins?
Propofol?
B2
Zinc
furosemide
Volatile
anaesthetics/
Alcohols
Convulsants (PTX)
P
P
P
drug binding sites of the GABAA receptor. (A) Cartoon showing the four transmembrane domains of a single subunit of the
smembrane domain 2 is shown as the shaded barrel that lines the pore ofSleep
the ion
channel.5 (B)
Schematic
plan
view of a GABAA
Medicine
Suppl.
1 (2004)
S9–S15
e subunits with the pore in the centre of the heteromeric molecule; adapted with permission from Whiting et al. 1999 [55].
cartoon of the GABAA receptor sitting in the plasma membrane with ligand-binding sites indicated; adapted with permission from
3392
BRIEF REVIEWS: AT1 RECEPTOR ACTI
The Journal of Immunology, 2007, 179: 3391–3395.
FIGURE 1. AT1-AA may underlie many features of preeclampsia by interacting with AT1 receptors on different cell types. AT1-AA from preeclamptic
FIGURE 2.
tion in norm
sFlt-1 is incre
We have sugg
a brake to in
under preecla
the maternal