Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Hormone replacement therapy (male-to-female) wikipedia , lookup
Hypothalamic–pituitary–adrenal axis wikipedia , lookup
Hypothyroidism wikipedia , lookup
Graves' disease wikipedia , lookup
Sexually dimorphic nucleus wikipedia , lookup
Vasopressin wikipedia , lookup
Hyperthyroidism wikipedia , lookup
Neuroendocrine tumor wikipedia , lookup
Hyperandrogenism wikipedia , lookup
Growth hormone therapy wikipedia , lookup
Kallmann syndrome wikipedia , lookup
Pituitary apoplexy wikipedia , lookup
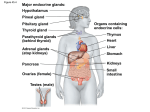
Neuro Chapter 17: Pituitary and Hypothalamus (pages 791-805) The pituitary and hypothalamus are the link between the neural and endocrine systems, and communicate through synaptic transmission The hypothalamus is the central regulator of homeostasis - To maintain homeostasis, the hypothalamus regulates 4 other systems and participates in: o Homeostatic mechanisms – controlling hunger, thirst, sexual desire, sleep-wake cycles o Endocrine control – through the pituitary o Autonomics o Limbics o Mnemonic – HEAL The pituitary forms from two different embryo pouches – page 792 - The anterior pituitary (adenohypophysis) forms from a thickened area of ectoderm on the roof of the developing pharynx, that invaginate to form Rathke’s pouch The posterior pituitary (neurohypophysis) forms from an evagination of the floor of the developing ventricular system The anterior pituitary has glandular cells that secrete lots of hormones into circulation - This release of hormones is controlled by the hypothalamus through the vascular portal system The posterior pituitary doesn’t have glandular cells, and instead has axons and terminals of neurons whose cell bodies are in the hypothalamus - These terminals secrete hormones oxytocin and vasopressin (ADH) into circulation The hypothalamus is part of the diencephalon – page 793 - It forms the walls and floor of the inferior part of the 3rd ventricle, and is separated from the thalamus by a shallow groove on the wall of the 3rd ventricle, called the hypothalamic sulcus Mammary bodies – paired structures that form the posterior part of the hypothalamus Infundibulum – means “funnel,” and runs from inferior as the pituitary stalk, and it’s anterior is called the median eminence o The median eminence is where hypothalamic neurons release things to go through portal vessels to the anterior pituitary The pituitary sits in the pituitary fossa, formed by the anterior and posterior clinoid process, which together with the sphenoid bone form the sella turcica - Just below the floor of the sell turcica is the sphenoid sinus, which allows the pituitary fossa to be accessed by transsphenoidal surgery The dura covering the superior part of the pituitary fossa is called the diaphragm sella - The pituitary is just behind and inferior the optic chiasm o So pituitary tumors can compress the optic chiasm, causing visual problems like bitemporal hemianopia Major hypothalamic nuclei – page 794 - - Periventricular nucleus – most medial nuclei, and lies closest to the 3rd ventricle The fornix fibers pass through the hypothalamus on the way to the mammillary body, dividing the hypothalamus into a medial hypothalamic area and a lateral hypothalamic area o The lateral hypothalamic area has the lateral hypothalamic nucleus, and the medial forebrain bundle, which carries many connections to and from the hypothalamus Most the nuclei are in the medial hypothalamic area, which is divided into 4 regions from anterior to posterior o The preoptic area is most anterior, and comes from the telencephalon instead of the diencephalon like the hypothalamus, but it’s still functionally a part of the hypothalamus The lateral and medial preoptic nuclei are continuations of the lateral and medial hypothalamic areas o The rest of the medial hypothalamus can be divided into 3 areas from anterior to posterior: The anterior hypothalamic region (aka supraoptic region) includes the anterior hypothalamic nucleus, supraoptic nucleus, paraventricular nucleus,a dn suprachiasmatic nucleus Some neurons in both the supraoptic and paraventricular nuclei have oxytocin or vasopressin, and project to the posterior pituitary The suprachiasmatic nucleus is the “master clock” for circadian rhythm o Receives info from retinal ganglion cells that have the pigment melanopsin, which conveys info about day-night cycles from the optic chiasm to the suprachiasmatic nucleus The middle hypothalamic region (aka tuberal region) includes the arcuate nucleus, ventromedial nucleus, and dorsomedial nucleus The arcuate nucleus is one of the hypothalamic nuclei projecting to the median eminence to control the anterior pituitary The posterior hypothalamic region (aka mammillary region) includes the medial, intermediate, and lateral mammillary nuclei, and the posterior hypothalamic nucleus Hypothalamic control of the autonomics: - The hypothalamus has descending projections from mainly the paraventricular nucleus, but a little from the dorsomedial hypothalamic nucleus and lateral and posterior hypothalamus, down to the symp and parasymps of the autonomic nervous system o The descending autonomic fibers travel in the medial forebrain bundle, then into the dorsolateral brainstem, and then synapse onto pregang parasymp nuclei int eh o brainstem and intermediate zone of the sacral spinal cord, and onto pregang symp neurons in the intermediolateral cell column of the thoracolumbar spinal cord The amygdala and limbic cortex gives input to the hypothalamus to regulate autonomics Hypothalamic-Limbic pathways: - - - The hippocampal formation of the limbic system projects to the mammillary bodies through the fornix o The mammillary bodies then project to the anterior thalamic nucleus, which projects to the limbic cortex in the cingulate gyrus The amygdala connects to the hypothalamus through the stria terminalis and ventral amygdalofugal pathway The limbic-hypothalamic connections are important for emotional influence of autonomics (like when your palms get sweaty when you’re nervous), and on homeostasis, including the immune system (like how depressed people are more prone to infection) Hypothalamic hamartoma – rare benign tumor that causes seizures with laughing episodes o Shows link between hypothalamus and limbics o Starts in early childhood, and also shows irritability and aggression, with cognitive impairment o Some hypothalamic hamartomas secrete gonadotropin releaseing hormone, leading to early puberty Other jobs of the hypothalamus: - - - The suprachiasmatic nucleus in the anterior hypothalamus regulates circadian rhythm o The GABA neurons in the ventral lateral preoptic area (VLPO) help non-REM sleep by inhibiting the arousal systems, including histamine, orexin, serotonin, dopamine, and adrenergics and cholinergics o So lesions of the anterior hypothalamus that include the VLPO, will cause insomnia Lesions in the posterior hypothalamus, where all those neurons for histamine and other arousal stuff are, will cause hypersomnia (very sleepy) The lateral hypothalamus is important in appetite o Lesions here cause decrease in body weight The medial hypothalamus has the ventromedial nucleus, which inhibits appetite o So lesions to the medial hypothalamus can lead to obesity o Leptin is a hormone made by adipose, that binds to the hypothalamus to decrease appetite o Ghrelin is a hormone released by the gastric mucosal cells, and it binds the hypothalamus to stimulate appetite Thirst is activated by osmoreceptors in the anterior hypothalamus o Lesions of the lateral hypothalamus decrease water intake (yes it says lateral) The anterior hypothalamus detects increased body temperature o Anterior hypothalamic lesions can cause hyperthermia - The posterior hypothalamus works to conserve heat o Lesions of the posterior hypothalamus cause poikilothermia, where the body temp changes along with the environment because both heat conservation areas of the posterior, and descending pathway from the anterior, are destroyed Endocrine jobs of the pituitary and hypothalamus: - - - - The anterior pituitary makes hormones adrenocorticotropic hormone (ACTH), growth hormone (GH), prolactin, thyroid-stimulating hormone (TSH), luteinizing hormone (LH), and folliclestimulating hormone (FSH) The intermediate pituitary makes pro-opiomelanocortin (POMC) and melanocyte-stimulating hormone (MSH) The posterior pituitary releases oxytocin and vasopressin (ADH aka arginine vasopressin, AVP) Neurons in the hypothalamus controls release of anterior pituitary hormones by releasing hormones into the hypophysial portal system o The pituitary gets blood from the inferior and superior hypophysial arteries, which both branch from the internal carotid o The first capillary plexus of the portal system is at the median eminence, so neurons next to the 3rd ventricle, and many hypothalamic nuclei, project to the median eminence Nuclei include the arcuate, periventricular, medial preoptic, and paraventricular nuclei o Here they secrete factors to promote or inhibit pituitary hormone release o Portal veins then carry the factors to the anterior pituitary o All of the hypothalamic factors are peptides, except prolactin release-inhibiting factor (PIF), which is just another name for dopamine Hormones released by the anterior pituitary then go into the 2nd capillary plexus of the portal system, and are drained by veins to the cavernous sinus, and then to the internal jugular vein The posterior pituitary has a capillary plexus too, which carries away oxytocin and ADH o The cell bodies of neurons that release these hormones are in the supraoptic and paraventricular nuclei Both nuclei have both hormones, but no neurons have both, some have one and some have the other Page798-799 What the hormones do: - - ACTH – stimulates the adrenal cortex to make glucocorticoids, especially cortisol o Glucocorticoids are big on controlling electrolyte balance and promoting glucose mobilization o Also has a smaller ability to stimulate making of mineralocorticoid aldosterone TSH – stimulates the thyroid gland to make thyroxine (T4) and triiodothyronine (T3) o Thyroid hormones promote cell metabolism - GH – causes the liver, kidneys, and other organs to make insulin-like growth factors (IGF, aka somatomedins), which promote increased growth of long bones and tissues Prolactin – causes mammillary glands to make milk LH and FSH – regulate ovarian hormones for menstruation and oogenesis in females, and regulate testicular hormones and spermatogenesis in males Oxytocin – causes contractions of smooth muscle in breasts for milk, and contractions of the uterus during labor Vasopressin (ADH) – promotes water retention by the kidneys, which concentrates the urine The hypothalamic-pituitary axis is regulated by many neuroendocrine feedback loops: - Ex: release of CRH by the hypothalamus and ACTH by the anterior pituitary, both are inhibited by cortisol in the blood o Chronic taking of exogenous steroids can suppress ACTH making to the point the adrenals atrophy and can’t make enough cortisol if you remove the steroids Pituitary adenoma – slow growing benign tumor that comes from glandular epithelial cells in the anterior pituitary - - It’s a common tumor that can happen at any age, but is most common around 40 A pituitary adenoma can come from any of the epithelial cell types in the anterior pituitary, and most pituitary adenomas secrete at least one pituitary hormone The hormones released are in excess, and don’t respond to feedback inhibition Even small pituitary microadenomas cause hormone problems The minority of pituitary adenomas that don’t release hormone (aka silent) often grow a lot larger before you see symptoms Headache is common, and more common in large tumors Large tumors can also compress the optic chiasm, causing visual problems o The characteristic problem in a pituitary adenoma is bitemporal hemianopia Untreated large tumors can eventually cause hydrocephalus and compress the brainstem o Hydrocephalus – basically brain swelling The most common hormone secreted by a pituitary adenoma is prolactin (half!) Treatment options for pituitary adenomas include meds and surgery o Prolactin-secreting tumors respond well to treatment with dopaminergic agonists like bromocriptine or cabergoline, which inhibit prolactin release and shrink tumors o Non-prolactin releasing tumors are usually treated with surgery, since drugs are less effective o Surgery is done with a transsphenoidal approach, where they go through the nose and through the sphenoid sinus and through the floor of the pituitary fossa Clinical presentation of types of pituitary adenomas: o Prolactin-secreting adenomas: Usually show amenorrhea in women, hypogonadism in men, galactorrhea, infertility, hair loss, decreased libido, and weight gain o o Galactorrhea – spontaneous milk from the nipples High prolactin inhibits LHRH from the hypothalamus, which causes decreased LH and FSH In women this delays resumption of menses during lactation Any pituitary tumor can cause headache and visual symptoms Diagnose by high prolactin GH-secreting adenomas: Cause acromegaly – slow progressive overgrowth of bones and soft tissues Acromegaly is characterized by enlarged hands and feet, coarsened facial features, and a protuberant jaw GH excess in kids before the epiphyseal closure will cause gigantism Other problems seen in excess GH are carpal tunnel, arthritis, infertility, hypertension, and diabetes Diagnose by symptoms, and high GH and IGF-1 ACTH-secreting adenomas – cause Cushing disease Cushing syndrome – general name for excess glucocorticoids of any reason Cushing’s syndrome shows a characteristic “cushingoid” appearance, with a round “moon-shaped” face, and deposition of fat on the trunk more than the extremities, causing truncal obesity o So they’re described as “spiderlike” Excess glucocorticoids also causes acne, hirsutism, hypertension, diabetes, edema, immunosuppression, osteoporosis, avascular necrosis of the femoral head, amenorrhea, decreased libido, myopathy, fatigue, and psych problems like mania, psychosis, and depression Endogenous Cushing’s syndrome is caused by primary adrenal adenomas or adenocarcionmas only about 15% the time o The rest are caused by Cushing’s disease or ectopic ACTH making, like in bronchial carcinoma Cushing’s disease – cause of Cushing syndrome caused by a ACTH-secreting pituitary adenoma Diagnosing the cause of Cushing syndrome: Low ACTH usually suggests the adrenals, since excess cortisol will cause feedback decrease of ACTH making If you have an ACTH making tumor, use the dexamethasone suppression test o Giving them a low dose of dexamethasone at nite will work like cortisol for negative feedback to decrease cortisol levels or urine cortisol the next morning o If low dose doesn’t work, use high dose o ACTH secreting pituitary tumors usually will be suppressed by this dose, while ectopic tumors and adrenal tumors will not Can also give them CRH, which increases plasma ACTH and cortisol in pituitary adenomas, but not in ectopic or adrenal tumors When these tests still didn’t tell you, do petrosal sinus sampling, where you insert catheters through the femoral veins up to the internal jugular veins to reach the inferior petrosal sinuses on both sides o You then sample to see the ACTH levels o ACTH-secreting tumors will show at least double the ACTH levels of a peripheral vein o Then give them CRH, and measure ACTH every 5 minutes o An increase of 3 times what it was is diagnostic of a pituitary adenoma TSH-secreting adenomas – a rare cause of hyperthyroidism Instead, hyperthyroidism is usually primary, like Grave’s disease, thyroiditis, toxic goiter, and thyroid adenomas Symptoms of hyperthyroidism are nervousness, insomnia, weight loss, tremor, excessive sweating, heat sensitivity, increased symps, and frequent bowel movements One way to differentiate is Grave’s will cause thyroid ophthalmopathy, but not in TSH-secreting adenomas Grave’s is characterized by inflammatory involvement of the thyroid, skin, and orbital tissues leading to proptosis and extraocular muscle fibrosis Other neuro signs of Grave’s are proximal muscle weakness, tremor, dyskinesia, and dementia In primary thyroid problems, TSH levels are completely suppressed, while in TSH secreting tumors, TSH will be high Hypothyroidism is usually caused by primary thyroid problems like autoimmune thyroid disease, iodine deficiency, and rarely caused by pituitary or hypothalamic insufficiency Lesions of the hypothalamus or pituitary though when present, commonly cause TSH making to be decreased Symptoms of hypothyroidism include lethargy, weight gain, cold intolerance, smooth dry skin, hair loss, depression, and constipation If it gets bad enough it can lead to myxedema coma and heart involvement Other important neuro signs include neuropathy, carpal tunnel, myalgias, ataxia, and dementia Both hypo- and hyperthyroidism can present in the elderly as just dementia or depression - Hypothyroidism in utero or infancy can cause cretinism, characterized by mental retardation, shortness, and microcephaly o LH or FSH secreting adenomas often cause infertility, and are usually large tumors Up to 1/10 of people getting an MRI for any reason will have a small, benign pituitary incidentaloma, with no symptoms or problems Diabetes insipidus (DI) – making of lots of dilute urine, caused by deficiency of ADH (called central or neurogenic DI) or the kidneys don’ listen to ADH (nephrogenic DI) - Symptoms of DI include severe thirst, polyuria, and polydipsia If they don’t keep up with drinking water to replace what’s lost, they get dehydrated quickly and can die To diagnose DI, they’ll have polyuria with low urine osmolality (solutes), but high plasma osmolality (solutes) A dose of vasopressin (ADH) will cause urine osmolality to rise in neurogenic DI, but not nephrogenic Common causes of DI include neurosurgery, head trauma, and infltrative or cancerous lesions of the pituitary or hypothalamus or 3rd ventricle Syndrome of inappropriate antidiuretic hormone (SIADH) – excess ADH making causes low serum sodium (hyponatremia, from reabsorbing lots of water through aquaporines), and ↑ urine osmolality - Hyponatremia with increased urine osmolality is not specific for SIADH, and can also be seen in hypovolemia or edema’s like heart failure or cirrhosis Treat by restricting fluid intake, and vaprisol (a vasopressin blocker) Severe cases you give them hypertonic saline, but make sure not to correct the hyponatremia too quickly or you can cause central pontine myelinolysis Panhypopituitarism – deficiency of all pituitary hormones - - ACTH deficiency – causes hypocortisolism, with fatigue, weakness, decreased appetite, and impaired response to stress, leading to hypotension, fever, hypoglycemia, and ↑ mortality rate TSH deficiency causes hypothyroidism ADH deficiency causes diabetes insipidus LH and FSH deficiency cause hypogonadism, decreased libido, amenorrhea, and infertility GH deficiency in kids causes them to be short Prolactin deficiency in women causes inability to lactate Oxytocin deficiency causes impaired milk release The most common cause of panhypopituitarism is primary pituitary tumors & their treatment Rarely, pituitary tumors can randomly hemorrhage, causing pituitary apoplexy o Shows sudden headache, meningeal signs, cavernous sinus syndrome, vision loss, hypotension, and depressed level of consciousness Treat by exogenously replacing the hormones o o o o o ACTH deficiency is treated by daily dose of steroids like prednisone or hydrocortisone, with increased doses needed during times of stress, like infection or surgery Diabetes insipidus is treated with ADH analogs Hypothyroidism is treated with synthetic thyroid hormones Hypogonadism is treated with test or estrogen/progesterone, and fertility can be restored sometimes by LH and FSH substitution GH replacement can help growth in kids, and improve lipid profile in adults Path Chapter 24: The Endocrine System (pages 1098-1107) The anterior pituitary makes up about 80% of the pituitary gland Cells the anterior pituitary can show in histo are: - Acidophils- eosinophilic cytoplasm Basophils- basophilic cytoplasm Chromophobe- poorly staining cytoplasm Five types of pituitary cell types: - Somatotrophs- acidophils that make GH, and are half the anterior pituitary cells Lactotrophs (mammotrophs)- acidophils that make prolactin Corticotrophs- basophils that make ACTH, POMC, MSH, lipotropin, and β-endorphin Thyrotrophs-basophils that make TSH Gonadotropes- basophils that make FSH and LH o FSH stimulates making of graafian follicles in the ovary o LH induces ovulation and making of the corpus luteum The posterior pituitary consists of modified glial cells called pituitcytes, and axon terminals from the hypothalamus, that carry oxytocin and ADH (vasopressin) to the posterior pituitary and store them in the axon terminals Hypopituitarism is a result of decreased pituitary hormones, and can be caused by ischemia, surgery, radiation, inflammation, and nonfunctional tumors Pituitary lesions often cause changes to the sella turcica you can see on radiographic images - - Optic nerves and the chiasm are close to the sella, so pituitary tmors often compress crossing fibers of the chiasm, causing visual field problems, classically a defect in lateral (temporal) visual fields, called bitemporal hemianopsia These tumors can also cause increased intracranial pressure symptoms, like headache, nausea, and vomiting Pituitary apoplexy- acute hemorrhage into an adenoma, causing its rapid enlargement o It’s an emergency that can cause sudden death Page 1100 The most common cause of hyperpituitarism is an adenoma of the anterior lobe - - Pituitary adenomas are classified by the hormone they make Some adenomas can release two hormones (usually GH and prolactin), and any more than two is rare Functional adenomas cause excess hormone, and nonfunctional do not Large pituitary adenomas can get so big they destroy the pituitary and cause hypopituitarism Microadenomas are small ones, and macroadenomas are big ones Genetic causes of pituitary adenomas: o G protein mutations The α subunit of a GS protein is coded by the GNAS gene Normally, GS is inactive and bound to GDP Ligand binding causes GDP to leave, and GTP to bind, activating the G protein, leading to cAMP This effect is transient, due to GTPase in the α subunit, which hydrolyzes GTPGDP A mutation in GNAS to the α subunit GTPase activity will cause persistent making of cAMP, once the G protein’s been activated, leading to unchecked cellular proliferation GNAS mutations are a common cause of adenomas in pituitary cells that use G proteins and cAMP, like somatotrophs and corticotrophs o Most pituitary adenomas are sporadic, and not many area inherited Four genes that cause familial pituitary adenomas: MEN1, CDKN1B, PRKAR1A, and AIP3 Germline mutations to MEN1 cause multiple endocrine neoplasia syndrome type 1 (MEN-1) MEN1 makes the tumor suppressor protein menin People with MEN-1 get tumors in many endocrine organs, including the pituitary Mutations to CDKN1B mutate the checkpoint regulator KIP1, causing a “MEN-1 like syndrome” Protein kinase A regulatory subunit 1α (PRKAR1A) gene mutation causes Carney complex, which causes pituitary and endocrine tumors PRKAR1A codes a tumor suppressor to regulate protein kinase A, and therefore cAMP AIP mutations often cause acromegaly Problems with cell cycle checkpoint genes, like cyclin D1, p53, and RB1 can cause pituitary tumors, as can mutations to the HRAS oncogene Morphology of pituitary adenomas o Typical pituitary adenomas are soft, circumscribed lesions that can be confined to the sella turcica, or extend superiorly to compress the optic chiasm o Invasive adenomas infiltrate neighboring tissue o o Macroadenomas are more commonly invasive, and more likely to have necrosis and hemorrhage The main identifying factor is an absence of a reticulin network Atypical adenomas are more likely to be aggressive Types of pituitary adenomas: - - - Prolactinomas- most common hyperfunctioning pituitary adenoma o Most have weakly acidophilic or chromophobic cells, called sparsely granulated o Rare cases are very acidophilic, and called densely granulated prolactinoma o Prolactinomas commonly undergo dystrophic calcification, and can result in “pituitary stones” o Prolactin secretion will be proportional to how big the adenoma is o Prolactinemia (increased blood prolactin) causes amenorrhea, galactorrhea, loss of libido, and infertility ¼ of cases of amenorrhea are from a prolactinoma o Prolactinemia can also be caused normally by pregnancy, nipple stimulation, and stress Lactotroph hyperplasia can also happen when dopamine inhibition from the hypothalamus is taken away o Because of these other causes of increased prolactin, even if you have a pituitary adenoma and ↑ prolactin, it doesn’t mean it’s a prolactin-secreting tumor o Treat with surgery and bromocryptine (dopamine agonist) GH somatotroph adenomas o Second most common functioning pituitary adenoma o Can also be densely granulated or sparsely granulated Densely granulated adenomas-acidophilic and have strong GH staining in the cytoplasm (more granules means more hormone) Sparsely granulated adeonams- have chromophobe cells and weak staining for GH o Chronic increase in GH triggers liver secretion of IGF-1 o Gigantism happens in children, with ↑body size and disproportionately long arms & legs o Acromegaly happens in adults, with growth of lots of things Organs, jaw, hands, feet, and bone density all ↑, with sausage fingers o Diagnose with ↑GH and IGF-1, and failure of glucose to ↓GH o Treat with surgery, somatostatin analogs, or GH receptor antagonists ACTH corticotroph adenomas o Usually small, basophilic(densely granulated) but sometimes chromophobic (sparsely granulated) o Stains PAS thanks to carbs in POMC o ACTH adenomas cause excessive adrenal secretion of cortisol, leading to hypercortisolism aka Cushing syndrome - When Cushing syndrome is caused by a primary tumor at the pituitary, it’s called Cushing disease o Nelson syndrome-destructive adenomas after surgery to remove the adrenals to treat Cushing, since no negative feedback to inhibit a preexisting corticotroph adenoma Gonadotroph adenomas are hard to catch, and usually aren’t noticed until you get neural symptoms from the growing tumor Hypothyroidism with evidence of posterior pituitary dysfunction, like diabetes insipidus, is almost always a problem at the hypothalamus - Can be caused by: o Tumors, brain trauma or injury, hemorrhage o Pituitary surgery or radiation can accidentally cause hypopituitarism o Pituitary apoplexy- sudden hemorrhage into the pituitary, causing an adenoma o Ischemia of the pituitary o Sheehan syndrome-postpartum necrosis of the anterior pituitary During pregnancy the a. pituitary enlarges, without an increase in blood supply o Rathke cleft cysts o Empty sella syndrome-destruction of the pituitary from enlarged sella Primary empty sella- problem in diaphragma sella allows arachnoid mater and CSF to get into the sella and compress the pituitary Secondary empty sella- a mass enlarges the sella o Genes o Hypothalamus problems o Inflammation and infection Posterior pituitary syndromes can cause diabetes insipidus and excess ADH - Diabetes insipidus- caused by ADH deficiency or kidney issue that leads to excessive urination thanks to the kidneys not being able to resorb water from the urine The most common hypothalamus lesion is a glioma or craniopharyngioma - - Adamantinomatous craniopharyngiomas- normally seen in kids o Usually has calcifications and compact lamellar keratin, called “wet keratin”, which is diagnostic Papillary carniopharngyiomas- normally seen in adults