Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
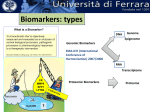
Molecular mimicry wikipedia , lookup
Immune system wikipedia , lookup
Hygiene hypothesis wikipedia , lookup
Polyclonal B cell response wikipedia , lookup
Adaptive immune system wikipedia , lookup
Sjögren syndrome wikipedia , lookup
Innate immune system wikipedia , lookup
Management of multiple sclerosis wikipedia , lookup
Psychoneuroimmunology wikipedia , lookup
Cancer immunotherapy wikipedia , lookup
Adoptive cell transfer wikipedia , lookup
FDA Tools to Accelerate Clinical Development of Therapeutics Addressing Unmet Medical Needs Amy S. Rosenberg, M.D. Division Director, Office of Biotechnology Products CDER, FDA FDA Regulated Research: Innovation & Compliance March 3, 2017 The Ohio State University and Nationwide Children’s Hospital Disclosure and Disclaimer Unless specified as FDA Guidance or Regulations, this speech reflects the views of the author and should not be construed to represent FDA’s views or policies. I have no financial relationships to disclose. 2 3 3 No Magic Bullets for Preventing or Curing Complex Infectious Diseases: Failure to Successfully Address Latent States • • • • HIV EBV CMV Ebola 4 4 No Magic Bullets for Complex Diseases • Most solid tissue advanced cancers • Autoimmune Diseases • Muscular Dystrophies 5 5 Immune Responses that Mediate or Modulate Human Disease Neurodegenerative Disease Eg Alzheimer’s B cells Neutrophils ASHD ILCs Muscular dystrophies Eg DMD Macrophages Autoimmune Disease (Eg Type 1 diabetes) HSC T cells NK cells Cancer Checkpoint inhibition; IDO; neovascularization Eosinophils Manipulation of T-Cell Populations and Functions for Disease Indications Teff Checkpoint Inhibitor Antagonists Treg Cancer Chronic Infection Teff Treg Checkpoint Inhibitor Agonists Teff Treg Autoimmunity Graft Rejection 7 Advanced Cancer is a Complex Disease and Not Generally Amenable to Single Targeting “Magic Bullet” Strategy • Check point blockade only one therapeutic modality to address cancer • Emergence of tumor resistance: loss of expression of target antigens; alternative survival signaling pathways • Microenvironment derived suppressive factors (eg IDO) and cells (Tregs, MDSC) • Tumor angiogenesis • Tissue modifying enzymes that facilitate proliferation and metastases 8 8 Heterogeneity in Cellullar Content and Expression of PDL1 on Tumors: Tailoring of Cancer Immunotherapy (Smyth M et al 2015) Median PFS in melanoma patients treated with Nivolumab and ipilmumab: 14 months among patients with PDL1 expressing tumors 9 Tumor-Expressed IDO Recruits and Activates MDSCs in a Treg-Dependent Manner (Holmgaard R et al 2015) Systemic expansion of CD11b+Gr1int myeloid cells Myeloid cells MDSCs Migration to tumors Tumor cells Tregs CTLs ? Conversion to MDSCs in tumors PD-L1 INOS Arg1 Activation of Tregs IDO TGFb CTLs TNFa 1. Enhanced tumor growth 2. Resistance to immune checkpoint blockade 10 10 Addressing Remodeling of the Tumor Microenvironment to Facilitate Tumor Angiogenesis and Metastasis: Blockade of Matrix Degradation Factors (Spinelli F et al 2015) 11 From Immunologic Tolerance to Robust Tumor Immunity IDO IDO inducers? inhibitors MMP inhib CD47 block Tolerizing Vaccines Vaccines Tregulatory CART CARTs? TILs/CPbloc Therapeutics to boost/stabilize Tregs Diminish Reprogram Inflammation inflammation and Induce & block Tolerance escape Block Convert immune Teff to tolerance Tregs Checkpoint Activating Antibodies for antibodies Coinhibitory Molecules ESTABLISH CANCER TOLERANCE CURES Stimulate Stimulate Adaptive Tregulatory immunity cells Eliminate Destroy Autoreactive tumor cells Cells Combination Chemotherapy/ Therapeutics? Radiotherapy Virotherapy 12 Challenges • Improved outcomes in melanoma: cures still relatively rare: greater longevity of PFS • Improved efficacy in non-melanoma “sterile” tumors with lower immunogenicity: how to enhance neoantigen expression, expression of check point targets: radiotherapy, other modalities? • Minimize toxicities: avoidance of global autoimmunity; more specific targeting of tumor vs healthy tissue • Combination therapies rather than sequential treatments – Preclinical verification: efficacy and elucidation of toxicities – Dosage considerations 13 13 Manipulation of T-Cell Populations and Functions for Disease Indications Teff Checkpoint Inhibitor Antagonists Treg Cancer Chronic Infection Teff Treg Checkpoint Inhibitor Agonists Teff Treg Autoimmunity Graft Rejection 14 Contraction injury Initiation and Perpetuation of Innate and Adaptive Immunity in Dystrophic Muscle Dystrophin deficient muscle Leaky membrane DAMPs muscle Ag ATP Innate immune activation T cells Macrophage Innate immune cells Cytokines & Chemokines Th2 B cell CD4 Adaptive immune activation IL-2,IL-4,IL-6 CD4 Th1 Plasma cells M2 IL-10, TGF-b IFN-g Tregs APC M1 TNF-a, IL-6,IL-1 CD8 Muscle remodeling,15degeneration, regeneration, inflammation and fibrosis 15 Dystrophin Replacement Therapy Should be Highly Effective in DMD but…. • Preexisting, age correlated, dystrophin immunity in a substantial percentage of patients: revertant fiber expression of dystrophin at low levels and in an inflammatory environment that promotes HLA expression on muscle primes dystrophin responses rather than tolerizes; • Dystrophin appears as a neoantigen to DMD patients as the majority have frame shift mutations leading to nonsense mediated decay of dystrophin mRNAs and lack of protein expression; • Dystrophin expression therapy elicits primary or boosts memory dystrophin specific immune responses 16 16 Preexisting Immunity to Dystrophin: Relationship to Revertant Fiber Expression of Dystrophin 17 Oligoclonal T Cell Populations at the Site of Muscle Degeneration in Duchenne Muscular Dystrophy: Specificity for Dystrophin? DMD Patients Vb1 Vb2 Vb3 Vb4 Vb5.1 Vb5.2 Vb6 Vb7 Vb8 Vb9 Vb10 Vb11 Vb12 Vb13 Vb14 Vb15 Vb16 Vb17 Vb18 Vb19 Vb20 84 85 86 5 pre-implant 1 mo post 6 mo post 6 pre-implant 1 mo post 6 mo post 8 pre-implant 1 mo post 6 mo post – + – + + + – – + – – – – – – – + + – – + – + + – – – – – – – – – – – – – – – – – – – – + – – – – – – – – – – – – – – – – – – – – – + + + + + + – – – – – + + + + – – – + – – – – – – – – – – – – – – – – – + – – – – – – – – + – – – – – – – – – – – – – – – – – + + + – – – – – – – – – + + – + – – + + – – – – – – – – – – – – – – – – – – – – – – – – – – – – – – – – – – – – – – – – – + + + + + – + + – – – – – – – – + – – – + + – + + – – – – – – – – – – – – – + – – – + + – – – – – – – – – – – – – – – – – – aQuantitation of TCR transcripts was accomplished through amplification of a Ca-Ca region as an internal control for variation among samples (28), con-comitantly with a TCR b-chain transcript, to assess the relative amount of each of 20 known TCR Vb families. Quantity of TCR Vb transcripts was expressed as a percentage of the quanity of the co-amplified Ca-Ca transcripts. In this table, the symbol + indicates values greater than 5%, and – indicates values <5%. Gussoni E et al J. Immunol 1994 18 Selection for the RVSG Motif in T cells Infiltrating Muscle in DMD Patient #5 Patient #8 Pre-implant TGC AGT GCC CAG CGT GTG TCT GGA AAC Pre-implant TGC AGT GCT AGT AGG GTG TCC GGT GAA C S C S C S A Q R V S G N Jb 1.3 (Y) Myoblast-injected leg 1 mo after transplant TGC AGT GCC CAG CGT GTG TCT GGA AAC A Q R V S G N Q R V S G N Jb 1.3 S A G R V S G N Jb 1.3 (Y) Jb 1.3 TGC AGT GCT AGG AGG GTG TCT GGA AAC C S A R R V S G N Jb 1.3 C S A S R V S G N Jb 1.3 Myoblast-injected leg 6 mo after transplant TGC AGT GCT AGC CGA GTA TCT GGA AAC C S C S A S R V S G E Jb 1.4 A Q R V S G T Jb 1.4 Myoblast-injected leg 6 mo after transplant TGC AGT GCT CAG AGG GTG TCG GGA ACA TGC AGT GCA GGG AGG GTC TCT GGA AAC C S Placebo-injected leg 1 mo after transplant TGC AGT GCT CAG AGG GTG TCG GGA ACA Placebo-injected leg 1 mo after transplant TGC AGT GCC CAG CGT GTG TCT GGA AAC A C Patient #6 A Q R V S G T Jb 1.4 Patient #4 Placebo-injected leg 1 mo after transplant TGC AGT GCC TTG AGG GTG TCG GGC ATT C S A L R V S G N Jb 2.1 (Y) Patient #86 TGC AGT GCT AGT AGG GTT TCT GGA AAC C S A S R V S G N Jb 1.3 (¶) Pre-implant TGC AGT GCT TCT CGG GTC TCT GGA AAC C S A C S A C S A S R V S G N Jb 1.3 (Y) Placebo-injected leg 1 mo after transplant TGC AGT GCT TCT CGG GTC TCT GGA AAC S R V S G N Jb 1.3 Myoblast-injected leg 6 mo after transplant TGC AGT GCT AAC AGG GTC TCT GGA ACA N R V S G N Jb 1.3 aNucleotide and amino acid sequences of the Vb2 T cells expressing the RVSG CDR3 motif. In some samples, clones with an identical nucleotide sequence were found more than one time. The symbol (Y) designates clones found two times, and (¶) designates clones found five times in the same sample 19 Expression of Dystrophin Revertant Fibers in a Patient with a deletion in Dystrophin exons 46-51 (Arechavala-Gomeza V et al Neuromuscular Disorders 2010) Time of Diagnosis + 6 years A B C Dys1 Dys2 Dys3 D E F Ex56-60 a-sarcoglycan B-dystroglycan G H I Dys1 Dys2 Dys3 J K L a-sarcoglycan B-dystroglycan UTR 20 Conclusions: • T cells invading the muscle of DMD patients transcribe similar receptors. • A selective T cell response directed to a specific antigen or antigens is occurring in DMD muscle. • The nature of the antigen or antigens that trigger these T cells is unknown: epitope spread within dystrophin and to other muscle specific proteins? • Likely specific for an ongoing process in DMD muscle, as no similarities were found in infiltrating T cells from control samples including fresh samples from muscle degenerating as a result of other diseases or conditions Gussoni E et al 1994 21 21 Dystrophin Immunity Present Prior to and Boosted by Gene Therapy with mini-Dystrophin Cassette A B dystrophin exon 350 MDP1 IFN-g SFC/106 PBMC 300 250 MDP3 200 p74 150 50 MDP2 55/56 CP 100 Revert Fibers MDP1 MDP2 MDP3 p74 CP Pretreatment Day 30 59 50 0 Pre-treatment Day 30 Post Gene Transfer 70 Mendell JR et al NEJM 2010 22 Evidence of Preexisting Immunity to Dystrophin: Revertant Fiber Expression Priming Patient ID Treatment Regimen Mutationa 12 21 74 39 19 35 11 14 59 Naïve Prednisone Naïve Naïve Naïve Prednisone Naïve Naïve Prednisone Splice exon 12 Del ex 45 Del ex 46-50 Del ex 48-50 Del ex 48-50 Del ex 50 Del ex 49-54 Nonsense ex 59 Nonsense ex 69 Truncating Mutation Location of Immune (prediction) Response + + + + + + + + + Location of Response Relative T Cell to Mutation Location Phenotype Exons 42-50 Exons 1-9 Exons 42-50 Exons 42-50 Exons 17-26 Exons 50-59 Exons 17-26 Exons 70-79 Exons 59-69 Downstream Upstream Upstream Upstream Upstream Downstream Upstream Downstream Uostream CD4 CD4 CD8 CD4 CD4/CD8 CD4 CD8 CD4 CD4 aDel, deletion; ex, exon. All are truncating mutations that are predicted to result in an interrupted mRNA reading frame. Flanigan KM et al HUMAN GENE THERAPY 24:797–806 2013 23 23 Age Increases the Probability of Dystrophin Reactive T cells in DMD Patients 1.0 DMD Steroid Naïve DMD Deflazacort Prednisone Estimated Probability 0.9 0.8 0.7 0.6 0.5 0.4 0.3 0.2 0.1 0.0 0 10 20 Age (years) 24 30 24 Steroids Diminish Frequency of Immunity to Dystrophin in DMD Percentage of Patients with Positive Immune Responses 100 80 p = 0.0423* 60 40 20 0 11/53 20.8% 9/17 52.9% DMD Steroid Treated DMD Steroid Naïve 25 N = 21 Normal 25 Role of Tregs in DMD: Suppression of Type 1 Pro-inflammatory Responses Evidence that Tregs modulate dystrophinopathy through the regulation of the immune response to injured muscle. Treg IL-10 M2 Mac Fibroblasts Progenitor populations M1 Mac X T cells Danger signals Dystrophin deficiency Contraction-induced injury Initial bout of injury and repair (acute injury) Subsequent cycles of degeneration and regeneration (chronic injury) Villalta SA and J. Bluestone STM 2014 Tregs are Elevated in Muscle of Human Subjects with DMD/BMD CD3/DAPI A FoxP3/DAPI Overlay B C Control 50 mm D E F Dystrophic 2.E-05 1.E-05 0.E-05 1.6E-06 1.2.E-06 8.0.E-07 4.0.E-07 0.0.E-00 P <0.01 4.5 4.0 3.5 3.0 2.5 2.0 1.5 1.0 0.5 0.0 NS IL-10 Fold Change (AU) 3.E-05 P <0.05 FoxP3+ Cell/mm2 CD3+ Cell/mm2 4.E-05 % FoxP3+ Cells Among CD3+ 50 mm 9.0 8.0 7.0 6.0 5.0 4.0 3.0 2.0 1.0 0.0 P <0.05 Villalta SA et al STM 2014 27 IL-2 Complex Treatments Increase Tregs and Reduce Muscle Inflammation and Injury in mdx mice Low-dose IL-2c treatment preferentially induces Tregs in vivo Y anti-IL-2 Ab recombinant IL-2 Treg non Tregs Villalta SA and J Bluestone STM 2014 TLRs DAMPs Enzymes CK P2X7 ATP Inflammasome/NF-kB Rawat et al., Am J Pathol. 2010 Jun;176(6):2891-900. 2010 Uaesoontrachoon et al., J Pathol. 2013 Oct;231(2):199-209 Henriques-Pons et al., Hum Mol Genet. 2014 May 15;23(10):2604-17 Pro-inflammatory cytokines and chemokines Myofiber death Damage Associated Molecular Patterns: (DAMPS): Endogenous Ligands of Toll Like Receptors Sloane et al., 2010 30 TLR7 is Highly Upregulated in the Muscle Fibers in Infants and in Symptomatic Patients with DMD DMD Healthy A B C D Isotype-DMD CMD Chen YW et al Neurol.2005 31 Myd88, a Common Adaptor of TLR Signaling Pathways through NF-kB Cell Membrane TRAM TRIF IRAK TIR DD TIR DD MyD88 TLR2 TLR4 Nucleus Endosome TRAM TRIF MyD88 NF-kB activation TLR 7/8/9 TLR3 IRF3 Inflammation 32 GRMD Muscle Histology Improved by Oral NFk-B Antagonist CAT-1041 Hammers DW et al JCI Insight 2016 33 Bridge Between Innate and Adaptive Immunity: NF-kB Activation by TLR Signaling Induces HLA Class I Expression on Dystrophic Muscle and Antigen Presentation A B C D p65 DMD p65 Cont Dystro Def Muscle E HLA Class I DMD F HLA Class I Cont 34 Conclusions • Optimization of dystrophin replacement therapy requires early treatment to preclude conditions of immunologic sabotage • Treatment early in disease course (infancy) prior to symptomatology with appropriate anti-inflammatory agents may prolong muscle viability and strength and prolong life • Inhibition of complement activation and generation of C’ attack complex may diminish C’ mediated destruction of muscle • The potential of TGF-b to have antithetical disease stage effects should be further investigated • Reduction of the inflammatory response may diminish expression of HLA class I and II, diminishing presentation of dystrophin peptides to the immune system. • Reduction of inflammatory response critical in context of boosting and enhancing Tregulatory cells and suppression of dystrophin specific immunity 35 35 Strategies to Preclude Dystrophin Immunity Require Administration of Replacement Therapy in Optimized Setting • Newborn screening for early diagnosis • Diminish the innate immune response – Anti-inflammatory therapies: • • • • • Steroids TLR and/or NFkB antagonists; Complement attack complex inhibitors: ecalizumab Inflammatory cytokine antagonists: a-TNF, IL-1? IVIG for immune modulation and protection against infection • Preclude or Eliminate Dystrophin Specific Immunity – – – – Early treatment Anti-inflammatory therapies Tregulatory cell promoting therapies: low dose IL-2; rapamycin, IL-10 Treg cellular therapy: per kidney transplant protocols; in phase 2 studies 36 Requirement for Immune Tolerance Induction in Rare Muscle Wasting Disease: Robust Immune Response Neutralizes Life Saving Enzyme Replacement Therapy in Pompe Disease High Titer CRIM+ Low Titer CRIM+ CRIM– (Kishnani PS et al 2011) 37 Immune Tolerance Induction to Enzyme Replacement Therapy: Greatly Improved Survival 1.00 3 on ventilator became ventilator free CN ERT + ITI* Ventilator Free Survival (n=7) * 0.75 0.50 CN ERT Monotherapy (n=11) 0.25 0.00 0 Banugaria SG et al PlosOne 2013 5 10 15 Months 20 25 30 High Titer and Sustained Antibody Responses: Unresponsive to Immune Suppressive Agents (Banugaria SG et al Genet Med 2013) High Titer Sustained Antibody Responses are Mediated by Long Lived Plasma Cells:Unaffected by MTX/Rituximab CD20 Rituximab Memory B cell Methotrexate Therapeutic protein CD20 BCR Cytokines B cell CD20? Short lived Plasma cell Peptide Antibodies MHCII APC TCR Helper T cell Long lived Plasma cell Bortezomib Antibodies Targeting Long Lived Plasma Cells with Bortezomib Reduces Antibody Titer in Patients with HSAT (Banugaria SG et al Genet Med 2013) FDA Tools to Accelerate Clinical Development of Products Addressing Unmet Medical Needs 43 43 44 Codevelopment Should Ordinarily be Reserved for Situations that Meet All of the Following Criteria • The combination is intended to treat a serious disease or condition. • There is a strong biological rationale for use of the combination – e.g., the agents inhibit distinct targets in the same molecular pathway or steps in disease pathogenesis; provide inhibition of both a primary and compensatory pathway; or inhibit the same target at different binding sites to decrease resistance or allow use of lower doses to minimize toxicity. • A full nonclinical characterization of the activity of both the combination and the individual new investigational drugs, or a short-term clinical study on an established biomarker, suggests that the combination may provide a significant therapeutic advance over available therapy and is superior to the individual agents – • A nonclinical model should demonstrate that the combination has substantial activity and provides greater activity, a more durable response (e.g., delayed resistance), or a better toxicity profile than the individual agents. There is a compelling reason why the new investigational drugs cannot be developed independently – e.g., monotherapy for the disease of interest leads to resistance, one or both of the agents would be expected to have very limited activity when used as monotherapy. 45 Overview of FDA Expedited Development Pathways • • • • Fast Track Breakthrough Accelerated Approval Priority Review 46 Approval Pathways for Drugs and Biologics Traditional (Regular) Approval Based on: Improvement in a direct measure of clinical benefit: eg Longer life, better life, or established surrogate Accelerated Approval Initiated 1992 for HIV: viral load surrogate Based on: Improvement in surrogate endpoint reasonably likely to predict clinical benefit over available therapy Requires postmarketing studies to confirm benefit Used frequently in Oncology 47 FDA Tools: Expedited Programs for Serious Conditions – Drugs and Biologics Program Qualifying Criteria: Serious condition and… Features Fast Track -Nonclinical or clinical data demonstrate potential to meet an unmet medical need -Or, QIDP -Actions to expedite development and review --E.g., meetings; rolling review Breakthrough Therapy -Preliminary clinical evidence indicates drug may demonstrate substantial improvement on a clinical significant endpoint over available therapies -All Fast Track features -Intensive guidance on efficient drug development -Organizational commitment Accelerated Approval -Provides meaningful advantage over available therapies -demonstrates effect on surrogate or clinical endpoint that can be measured earlier than irreversible morbidity or mortality -Approval based on a surrogate or intermediate clinical endpoint reasonably likely to predict clinical benefit Priority Review -Would provide a significant improvement in safety or effectiveness -Or, other qualifying programs -Shorter review clock goal for marketing applications (6 mo vs 10 mo) QIDP = qualifying infectious disease product; 48 Guidance for Industry Expedited Programs for Serious Conditions – Drugs and Biologics U.S. Department of Health and Human Services Food and Drug Administration Center for Drug Evaluation and Research (CDER) Center for Biologics Evaluation and Research (CBER) May 2014 Procedural OMB Control No. 0910-0765 Expiration Date: 03/31/2017 See additional PRA statement in section X of this guidance. 49 Available at: http://www.fda.gov/downloa ds/Drugs/GuidanceComplian ceRegulatoryInformation/Gui dances/UCM358301.pdf FDA Expedited Programs Breakthrough Therapy Fast Track NonClinical Early Clinical IND Submission Dose Exploration / Prelim Activity Priority Review Registration Trial(s) SPA NDA/BLA Submission Accelerated Approval APPROVAL FDA Review Efficacy and Safety Data If considering accelerated approval, post-marketing clinical trials should be underway at the time of approval. 50 Breakthrough Therapy Designation • Signed into law in 2012 • For serious life threatening disease, a drug, based on preliminary clinical evidence, has substantial improvement over available therapy • Approximately 40% of BT requests across drug center have been in Oncology – About a third of these have been granted 51 Examples of Breakthrough Therapies in NSCLC • Osimertinib in T790M mNSCLC – First in human to accelerated approval ~2.8 years – <5 month review • Nivolumab in 2nd line sq mNSCLC – 3.5 month review; • Pembrolizumab in 1st line PDL1 high mNSCLC 52 Breakthrough Therapy: Opportunities and Challenges – Opportunities: • “All Hands on Deck” for Transformative Therapies: – Aligns and Prioritizes Key FDA review teams (Clinical, Statistics, Manufacturing, Clinical Pharmacology, Toxicology, Inspections) • Optimizes communication between FDA and Sponsor – Challenges: • What is the right threshold for granting a BT designation? • What constitutes available therapy? • How late is too late? Timing of BT designation request • Resource saturation for both FDA and Sponsor? • On what basis should we rescind a BT therapy? • Manufacturing timelines can be a bottleneck 53 Summary • Expedited programs such as breakthrough and accelerated approval increasingly utilized to expedite access of transformative therapies to patients • Increased proliferation of novel, adaptive master protocols, seamless designs • Consideration of new approaches to response metrics, companion diagnostics, “real world” data 54 Acknowledgements • Gideon Blumenthal, Office of Hematology and Oncology Products • Steven Kozlowski, Director, Office of Biotechnology Products • Janet Woodcock, Director, CDER 55 56