Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
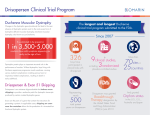
•inherited group of progressive myopathic disorders resulting from defects in a number of genes required for normal muscle function •Muscle weakness is the primary symptom.. •X-linked inheritance occurs with the following dystrophies: Duchenne and Becker muscular dystrophies Emery-Dreifuss muscular dystrophy dystrophinopathies. • are caused by mutations of the dystrophin gene • Duchenne muscular dystrophy (DMD) is associated with the most severe clinical symptoms • Becker muscular dystrophy (BMD) has a similar presentation to DMD, but a relatively milder clinical course Duchenne • Duchenne muscular dystrophy (DMD) is the most common dystrophinopathy, • resulting from complete absence of the dystrophin gene product: the subsarcolemmal protein, dystrophin The dystrophin molecule anchors the cytoskeleton of muscle cells to the extracellular matrix, via the dystrophin glycoprotein complex. This includes the sarcoglycans (mutations in which cause limbgirdle muscular dystrophies) and dystroglycans. Muscle cells that lack dystrophin are mechanically fragile, and fail after a few years, hence progressive muscle weakness. Fig. 6.4 ©Scion Publishing Ltd GENETICS AND PATHOGENESIS • DMD is a relentlessly progressive skeletal muscle disorder,caused by a mutation in the X-linked dystrophin gene, resulting in absence of a critical protein, dystrophin • The gene spans a distance of more than2.5 million base pairs and is the largest human gene isolated to date • In more than90 percent of males with the DMD genotype, there is an absence of dystrophin resulting from an “out-of-frame” mutation that disrupts normal dystrophin transcription GENETICS AND PATHOGENESIS,…. • Dystrophin is located on the cytoplasmic face of the plasma membrane of muscle fibers, functioning as a component of a large, tightly associated glycoprotein complex • Dystrophin normally stabilizes the complex, thereby shielding it from degradation. • In its absence, the glycoprotein complex is digested by proteases. • Loss of these membrane proteins may initiate the degeneration of muscle fibers, resulting in muscle weakness Duchenne muscular dystrophy • the clinical onset of weakness usually occurs between two and three years of age • In some cases, the onset of symptoms occurs later. • Children also frequently have varying degrees of mental retardation. • an occasional child may have average or above-average intelligence. DMD: Clinical manifestation • Weakness • Cardiomyopathy • Orthopedic complications Weakness • proximal before the distal limb muscles, • the lower before the upper extremities. • has difficulty running, jumping, and walking up steps. • When arising from the floor, affected boys may also use hand support to push themselves to an upright position, an action termed Gower's sign. • An unusual waddling gait, lumbar lordosis, and calf enlargement are usually observed. • Complaints of leg pain may also be found with early disease. Patients are usually wheelchair bound by the age of twelve. Cardiomyopathy • primary dilated cardiomyopathy (DCM) • conduction abnormalities, especially intraatrial and interatrial but also involving the AV node, and a variety of arrhythmias, primarily supraventricular • The cardiomyopathy is characterized by extensive fibrosis of the posterobasal left ventricular wall • Significant mitral regurgitation Cardiomyopathy,... • The incidence of symptomatic cardiomyopathy in patients with DMD increases gradually in the teenage years • about one-third of patients by age 14 years, one half by 18 years, and all patients older than 18 Orthopedic complications • Fractures involving the arms and legs are frequent. One series of 378 patients (ages 1 to 25 years) with DMD found that 79 (21 percent) had experienced fractures The most common mechanism was falling • A progressive scoliosis develops in nearly all children with DMD. • Scoliosis, in combination with progressive weakness, results in impaired pulmonary function. With progressive disease, patients may eventually suffer acute respiratory failure. Physical examination • pseudohypertrophy of the calf and (occasionally) quadriceps muscles • lumbar lordosis • a waddling gait • shortening of the Achilles tendons • hyporeflexia or areflexia DMD: Diagnosis Gower’s sign Becker muscular dystrophy • the age of onset of symptoms of those with BMD is usually later • the degree of clinical involvement milder • remain ambulatory at least until age 15 and commonly into adult life • Mental retardation and contractures are also not as common or severe • The distinction between BMD and limb-girdle dystrophy is often hard to make in patients with a negative family history for BMD Becker muscular dystrophy,… • cardiac involvement in BMD can be more severe • echocardiography revealed evidence of cardiac involvement in 60 to 70 percent of patients (mean age 18) with subclinical or benign BMD • Echocardiography reveals early right ventricular involvement with the later development of left ventricular dysfunction • All four chambers are eventually involved with fibrosis, • a cardiomyopathy with heart failure can be rapidly progressive • abnormalities of the AV node and infranodal conduction system can result in fascicular and bundle branch block and can progress to complete heart block. Prognosis • Patients with DMD are often confined to wheelchair by about age 12 years and die in their late teens or twenties from respiratory insufficiency or cardiomyopathy • Patients with BMD typically remain ambulatory beyond the age of 16 years and into adult life, and usually survive beyond the age of 30 years LABORATORY AND PATHOLOGIC FINDINGS • • • • • • Creatine kinase Electrocardiogram Electromyography Muscle biopsy Dystrophin analysis Genetic analysis SYMPTOM MANAGEMENT • • • • Vaccination Cardiac disease Pulmonary complications Complications related to anesthesia and sedation • Orthopedic interventions • Nutrition TREATMENT • • • • • Glucocorticoids Gene therapy Aminoglycosides PTC124 therapy Creatine PROGNOSIS • there may be some improvement between three and six years of age. However, this is followed by gradual but relentless deterioration, leading to wheelchair confinement by the age of approximately 12 years • Most patients with DMD die in their late teens or twenties from respiratory insufficiency (most commonly) or arrhythmia secondary to cardiomyopathy • patients with BMD typically remain ambulatory beyond the age of 16 years and into adult life; they usually survive beyond the age of 30 years and have a mean age of death in the mid 40s • The most common cause of death is heart failure from dilated cardiomyopathy, which also causes considerable morbidity in these patients despite their milder skeletal muscle involvement