Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Adaptive immune system wikipedia , lookup
Lymphopoiesis wikipedia , lookup
IgA nephropathy wikipedia , lookup
Polyclonal B cell response wikipedia , lookup
Psychoneuroimmunology wikipedia , lookup
Innate immune system wikipedia , lookup
Cancer immunotherapy wikipedia , lookup
Systemic lupus erythematosus wikipedia , lookup
Sjögren syndrome wikipedia , lookup
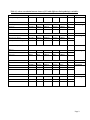
Significance of intrarenal B and T lymphocytic infiltrates in lupus nephritis Nashwa M. Emara, Mona A. Abou Elmahasen, Eman Saad Omar, Adel Zaki El-saidy, Zeinab I. El shawarby and Samia A.Youssef Abstract: Lupus nephritis (LN) is one of the most serious complications of systemic lupus erythematosus (SLE). The true prevalence of clinical lupus nephritis in persons with SLE is probably around 50%, being higher in certain ethnic groups and in children. It was hypothesized that intrarenal B cells form part of a local system with pivotal involvement in the pathogenesis of lupus nephritis. It enhances immunological responses and exaggerates the local immune response to persisting autoimmune damage in the tubulointerstitium. T cells cause tissue injury by activating and providing help to nephritogenic antibody-producing B cells, recruiting macrophages and dendritic cells (DCs), and producing cytokines. Aim: This retrospective study aims to assess intrarenal B and T lymphocytic infilterates in cases of lupus nephritis using CD20 and CD3and determine their possible value in lupus nephritis and their possible relation to clinical outcome. Results: Intrarenal B &T cells were more likely to be associated with class IV LN. LN activity index (AI), chronicity index (CI), proteinuria and serum creatinin had a significant statistical correlation with intrarenal B and T cell infiltrates. Conclusion: The current study concludes that interstitial inflammatory infiltrates and CI, but not AI could be used as prognostic factors in lupus nephritis and also may concludes that the presence of intrarenal B:T cell infiltrates and its grading could be used as a prognostic factor in patients of lupus nephritis. It shall provide a hope for management and improvement of prognosis of lupus nephritis patients especially the resistant cases by trials of anti CD20 drugs. Page 1 Introduction: Nephritis is a major cause of morbidity and mortality in patients with lupus. Nephritis occurs in approximately 50% of lupus patients, but rates vary significantly between genders (with female to male ratio 9:1) (Sada & Makino; 2009). The pathogenesis of lupus nephritis involves extrarenal and intrarenal pathogenic mechanisms. The extrarenal etiology of systemic lupus and lupus nephritis is based on multiple combinations of genetic variants that compromise those mechanisms normally assuring immune tolerance to nuclear autoantigens. The intrarenal etiology of lupus nephritis involves antibody binding to multiple intrarenal autoantigens rather than the deposition of circulating immune complexes (ICs) (Lech & Anders; 2013). Following the formation and/or deposition of ICs in the kidney, interactions between resident renal cells and infiltrating inflammatory cells promote tissue injury. Local cytokine, chemokine and adhesion molecule production leads to further influx of inflammatory cells and production of proinflammatory cytokines, ultimately resulting in renal inflammation, tissue injury and fibrosis. Lupus T cells express increased levels of molecules necessary for homing to the kidney (Wang et al; 2010). Mechanisms by which T cells contribute to tissue injury include activating and providing help to nephritogenic antibody-producing B cells, recruiting macrophages and dendritic cells (DCs), and producing cytokines (Apostolidis; 2011). Till now the role of pathogenic B cells were supposed to have a variety of functions that contribute to lupus nephritis. As they produce autoantibodies that can cause renal damage via disruption of cellular functions, cytotoxicity mediated by interactions with complement and release of inflammatory mediators. Presence Page 2 of germinal center-like structures and T cell-B cell aggregates in the kidney suggest in situ secretion of pathogenic antibodies, including nephritogenic antibodies, and ICs in human lupus patients (Chang et al; 2011, Hutloff et al; 2004). Material and Methods: Tissue samples Formalin-fixed, paraffin-embedded 57 renal biopsy specimens were obtained from Urology and Nephrology Center -Mansura University (UNC) and department of pathology, Faculty of Medicine, Benha University, during the years from 2009 to 2010. The studied biopsies were divided into control group formed of 6 biopsies of morphologically normal renal tissue (obtained postmortem) and the study group which was formed of 57 biopsies of different classes of lupus nephritis. All cases fulfilled the American College of Rheumatolgy criteria for diagnosis of SLE (Crow; 2013). Clinical evidence of LN was obtained in all cases and LN diagnosis was confirmed by examination of renal biopsy specimen. The following demographic, clinical and laboratory data were collected at time of renal biopsy: age, sex, 24 hr proteinuria, levels of serum creatinine, and presence or absence of anti-nuclear antibodies (ANA) (all the studied cases were positive for ANA). In addition to follow up of eighteen cases of the whole study group whose clinicopathologic data were available. The follow up was for one year from the diagnosis by clinical, laboratory and renal biopsy. Histopathological study: All patients underwent ultrasound-guided renal needle biopsy. Renal tissues obtained by biopsy were fixed in 10% neutral-buffered formalin, dehydrated gradually, and embedded in paraffin. Six serial tissue sections were cut at 3-4 Page 3 micrometer. The first two slides were used for immunostaining and the remaining four slides were used for Hematoxylin and Eosin, Periodic Acid-Schiff, Masson’s Trichrome, and Periodic Acid-Silver Methenamine. The biopsy specimens were classified using the International Society of Nephrology/Renal Pathology Society (ISN/RPS) 2003 classification of LN (Weening et al., 2004). Activity and Chronicity Indices of renal tissue injury were scored according to National Institutes of Health system (Austin; et al; 1983 ). Renal tissue injury was evaluated on the basis of activity and chronicity indices according to methods reported by Austin et al 1983. Activity index was calculated as the sum of the scores (on a scale of 1–3) of endocapillary proliferation, karyorrhexis, fibrinoid necrosis (the score was multiplied by 2), cellular crescents (the score was multiplied by 2), hyaline deposits, leukocyte exudation, and interstitial inflammation. The score of the chronicity index was the sum of the scores (on a scale of 1–3) for glomerular sclerosis, fibrous crescents, tubular atrophy, and interstitial fibrosis. Each activity and chronicity factor is graded on a scale of 0, 1, 2, and 3 depending on the percentage of involvement of glomeruli present in sections; where 0 (absence of lesions), 1 (lesions involving up to 25%), 2 (lesions involving 25–50%), and 3 (lesions involving >50%) (Gomaa et al ., 2014). Intervals of Activity and chronicity indices For the activity index, the biopsy specimens were classified in three intervals according to Makni et al., 2009 as follow: 1- AI of 5 or less was described as moderately active lupus nephritis. 2- AI of 5–9 was described as active lupus nephritis. 3- AI of >9 was described as extremely active lupus nephritis. Page 4 Chronicity index was classified in two intervals according to Makni et al., 2009 as follow: 1- CI of 3 or less was described when the specimen showed weak and limited chronic changes. 2- CI of more than 3 was described when the specimen showed widespread chronic changes. Scoring of tubulointerstitial inflammatory infilterate - 0 (nil), normal. - 1+ (mild), <25% of the acreage of interstitium affected. - 2+ (moderate), 25–50% of the acreage of interstitium affected. - 3+ (severe), >50% of the acreage of interstitium affected in each specimen (Yu et al., 2010). Levels of proteinuria was estimated according to Ivanyi., 2001: (+1) Proteinuria: less than 0.5 g /24 h urine, (+2) Proteinuria: 0.5-1g/24 h urine, (+3) Proteinuria: 1-2 g/24 h urine, (+4) Proteinuria: more than 2 g/24 h urine. Serum creatinin The typical human reference ranges for serum creatinine are 0.5 to 1.0 mg/dl for women and 0.5 to 1.5 mg/dl for men, above these levels creatinin was considered elevated or high serum creatinin (Faull., 2007). Division into progressors and non progressors was based on the slope of serum Creatinin according to Makni et al; 2009: Progressors were defined when creatinin increased by two fold or more from the lowest creatinine level reached under treatment, while The non-progressors were defined when serum creatinin level of patients was stable or improved. Page 5 Immunohistochemistry and quantification: Immunohistochemical staining of serial sections was performed for each LN patient using the following antibodies: CD20 (Labvision, cat, NO.MS-340-S0, USA) and CD3 (Labvision, cat, NO. MS401SO, USA) using DAKO envision flex method to detect the presence & distribution of B & T lymphocytes respectively through their membranous expression for such immunohistochemical markers. Sections were cut at 4 micrometer and mounted on positively charged slides. Sections were deparaffinized in xylene and rehydrated through descending grades of ethyle alcohol. Slides were washed with distilled water three times for 2 minutes each and placed in pressure cooking slide dish and covered with sufficient antigen retrieval solution and placed in pressure cooking at +125C0 in TRIS/EDTA buffer PH 8.5 for 5 minutes for antigen retrieval. Pressure cooking was continued at 80% power for 5 minutes then 60% for 5 minutes. Endogenous peroxidase activity was blocked by covering the sections with Envision TMFlex Peroxidase-Blocking reagent (DAKO, cat. NO. SM801) (which contains 3% H2O2) and incubated for 5 minutes. The sections were covered with primary mouse monoclonal anti-human CD3 (Labvision, cat, NO. MS401SO, USA) and CD20 (Labvision, Cat, NO.MS-340-S0, USA) at dilution of 1:50 then slides were incubated at room temperature for one hour. Slides were rinsed with buffer solution and were incubated at room temperature with Envision TMFlex/HRP (DAKO, cat. NO. SM802) for 30 minutes. The sections were covered with prepared DAB and incubated at room temperature for 10 minutes then washed with distilled water. Slides were counterstained was with mayer's hematoxylin (DAKO S3309) for 10 seconds. Slides were rinsed with tap water and dehydrated by dipping them several times in three changes of 95% ethanol followed by three changes of 100% ethanol. Slides were cleared by dipping several times in three changes of xylene and coverslippeded with mounting media (DPX). Page 6 Sections were screened on low power to show areas stained with CD20 and CD3, then examined using x400 objective and screened for both CD20 and CD3. Results of renal biopsies were classified according to organizational stage of intrarenal inflammatory infilterates descriped by Steinmetz et al.; 2008 and Shen et al.; 2012 who classified renal biopsies in four different groups as follow: Grade 0: shows no B cells but scattered or cluster like structure of T cells. Grade 1: consists of infiltrate of scattered T- and B-cells. Grade 2: consists of infiltrate have cluster-like structure but no T- or B-cell zones are evident . Grade 3: consists of infiltrates of clearly distinguishable separate T- and B-cell areas. Grade 4: consists of infiltrates of a highly organized structure with a central network of FDCs. All renal biopsies were scored with no prior knowledge of the clinical and laboratory analysis of patients. Statistical analysis: SPSS (version 16.0 software) statistical program was used, on a personal computer. The Pearson correlation coefficient was used to correlate different clinicopathologic variables to the median values of defined patient groups. Values were expressed as mean and standard deviation. P value of 0.05 or less was considered to be statistically significant. Page 7 Results: Clinical and histological results: The age of all studied cases ranges between 13 - 49 years with mean age ( 28.05 , SD+ 9.01). Out of fivety seven cases, fivety one (89.5%) were female, six (10.5%) cases were male with nearly female to male ratio 9:1 . -Distribution of of the ISN/RPS classification of the 57 patients was as follows: seven cases(12.3%) are class II, nine cases (15.8%) are class III, twenty seven cases (47.4%) are class IV ,seven cases (12.3%) are class V, seven cases (12.3%) are class VI. -Regarding the activity index: Fourteen cases (26.4%) are moderately active LN (0-5/24), twenty (35.1%) cases are active LN (5-9/24), twenty three (40.4%) cases are extremely active LN (>9/s24). -Regarding the chronicity index: Six cases (10.5%) show no obvious chronic changes, thirty one (54.5%) cases show weak and limited chronic changes (03/12), twenty (35.1%) cases show wide spread chronic changes(>3/12). -Regarding interstitial inflammtory infiltrate: Twenty six cases (45.6%) show mild (1+) inflammatory infiltrate, twenty four cases (42.1%) show moderate (2+) inflammatory infiltrate, seven cases (12.3%) show severe (+3) inflammatory infiltrate. -Regarding proteinuria: Two cases (3.5%) have (+1) proteinuria (<0.5 gm/24 hr urine), eight cases (14%) have (+2) proteinuria (0.5-1 gm/24hr urine), two case (3.5%) have (+3) proteinuria (1-2 gm/24 hr urine), fourty five cases (79%) have (+4) proteinuria (>2 gm /24 hr urine). -Regarding serum creatinin level: Twenty two cases (38.6%) have normal serum creatinine levels, thirty five cases (61.4%) have elevated serum creatinine levels. Page 8 Table (1): shows correlation between classes of LN with different clinicopathologic variables: Classes of lupus nephritis Clinicopathologic variable Total Significance P >0.05 (Insig) II III IV V VI Moderately active LN 6(85.7%) 1(11.1%) 1(3.7%) 2(28.6%) 4(57.1%) 14 Active LN 1(14.3%) 6(66.7%) 6(22.2%) 4(57.1%) 3(42.9%) 20 Extremely active LN 0(0%) 2(22.2%) 20(74.1%) 1(14.3%) 0(0%) 23 No chronic changes 2(28.6%) 0(0%) 3(11.1%) 1(14.3%) 0(0%) 6 Weak chronic changes 5(71.4%) 6(66.7%) 13(48.1%) 5(71.4%) 2(28.6%) 31 Widespread chronic changes 0(0%) 3(33.3%) 11(40.7%) 1(14.3%) 5(71.4%) 20 Mild(+1) 5(71.4%) 7(77.8%) 10(37%) 4(57.1%) 0(0%) 26 Moderate(+2) 2(28.6%) 2(22.2%) 12(44.4%) 3(42.9%) 5(71.4%) 24 Severe(+3) 0(0%) 0(0%) 5(18.5%) 0(0%) 2(28.6%) 7 +1 2(28.6%) 0(0%) 0(0%) 0(0%) 0(0%) 2 +2 2(28.6%) 1(11.1%) 4(14.8%) 1(14.3%) 0(0%) 8 +3 1(14.3%) 0(0%) 1(3.7%) 0(0%) 0(0%) 2 +4 2(28.6%) 8(88.9%) 22(81.5%) 6(85.7%) 7(100%) 45 Normal 5(71.4%) 7(77.8%) 6(22.2%) 4(57.1%) 0(0%) 22 Elevated 2(28.6%) 2(22.2%) 21(77.8%) 3(42.9%) 7(100%) 35 Total 7 9 27 7 7 57 Activity index Chronicity index P=0.031(Sig) Inflammmatory infiltrate P=0.004(Sig) Proteinuria P=0.003(Sig) S.creatinin P=0.003(Sig) Page 9 - No significant statistical correlation was detected between lupus nephritis classes and activity index, as it was found that most of cases of class II (85.7%) are moderately active lupus nephritis, in class III (66.7%) are active lupus nephritis, in class IV 74.1% are extremely active lupus nephritis. In class V most of cases 57.1% are active LN, whereas class VI was divided into (57.1%) moderately active and (42.9%) active LN (Table 1). - There was a significant statistical correlation between LN classes and chronicity index, as it was found that (71.4%) of class II and (66.7%) of class III have weak chronic changes. In class IV (48.1%) show weak chronic changes, (40.7%) show widespread chronic changes. In class V (71.4%) show weak chronic changes and in class VI (71.4%) show widespread chronic changes (Table 1). - There was a significant statistical correlation between LN classes and interstitial inflammatory infiltrate, as it was found that 71.4% of class II and 77.8% of class III have (+1) inflammatory infiltrate. While 44.4% of class IV have (+2) inflammatory infiltrate and 18.5% have (+3) infiltrate. In class V, 57.1% have (+1) inflammatory infiltrate, in class VI (71.4%) of cases have (+2) & (28.6%) have (+3) inflammatory infiltrate (Table 1). -There was a significant statistical correlation between LN classes and proteinuria, as cases in class II have different levels of proteinuria with nearly close percentage, but in class III 88.9% have (+4) proteinuria. In Class IV, 81.5% have (+4) proteinuria. In class V, 85.7% have (+4). All cases (100%) of class VI had +4 proteinuria (Table 1). -There was a significant statistical correlation between LN classes and serum creatinine , as most cases (71.4) of class II and (77.8%) of class III have normal serum creatinine level. In class IV, (77.8%) of cases have elevated serum creatinine. (57.1%) of class V have normal serum creatinine. All cases (100%) of class VI have elevated serum creatinine (Table 1). Page 10 Immunohistochemical results and their correlations: Upon staining of CD20 & CD3 of the same cases to show microanatomical organization of intrarenal lymphocytic infiltrate, renal biopsies were classified into four different groups as follow: eleven cases (19.3%) were negative for CD20 but showed scattered positive CD3 T cells and this group named non B cell group (Figure 1). In the B cell group twenty cases (35.1%) were grade 1 (Figure 2), twenty one cases (36.8%) were grade 2 (Figure 3), five cases (8.8%) were grade 3 (Figure 4; 5). No patients are identified in grade 4 (Table 2). - There was a significant statistical correlation between grades of B:T cell infitrates and LN classes, as it was shown that 63.7% of cases of grade 0 (non B cell group) were between class II &III (36.4% in class II, 27.3% in class III) . Sixty percent (60%) of cases of grade 1 were between class III & IV, (25% in class III, 35% in class IV) and 61.9% of grade 2 were in class IV and 80% of grade 3 were in class IV (Table 2). - There was a significant statistical correlation between grades of B:T cell infiltrates and activity index, as it was found that 54.5% of grade 0 (non B cell group) were moderately active LN (low AI), while the majority of grade 1 cases showed higher AI; as 45% were active LN and 25% were extremely active LN. Also in grade 2 about 95% showed higher AI and 80% of grade 3 were extremely active LN (Table 2). - There was a significant statistical correlation between B: T cell infiltrates and chronicity index as most cases (90.9%) of grade 0 (non B cell group) showed low CI (18.2% shows no obvious chronic changes and 72.7% shows weak chronic changes), while (85%) of grade 1 showed higher CI (60% shows weak chronic Page 11 changes and 25% shows widespread chronic changes), whereas 47.6% of grade 2 and 80% showed widespread chronic changes (Table 2). - There was a significant statistical correlation between B:T cell infiltrates and interstitial inflammatory infiltrate, as all cases(100%) of grade 0 (non B cell group) had (+1) interstitial inflammatory infiltrate. Sixty percent (60%) of grade 1 had (+1) inflammatory infiltrate. In grade 2 (71.4%) had (+2) inflammatory infiltrate. While in grade 3, 40% had (+2) inflammatory infiltrate and 60% had (+3) inflammatory infiltrate (Table 2). - There was a significant statistical correlation between B:T cell infiltrates and proteinuria , as 54.5% of grade 0 (non B cell group), 80% of grade 1, 90.4% of grade 2 and 80% of grade 3 have (+4) proteinuria (Table 2). - There was a significant statistical correlation B &T cell infiltrates and serum creatinin level , as it was found that 81.8% of grade0 (non B cell group) had normal serum creatinin while 55% of grade 1,81% of grade 2, 100% of grade 3 had elevated serum creatinin level (Table 2). Page 12 Table (2): shows correlation between B and T cell grades with clinicopathologic variables: B and T cell grades B cell group Total Significance Classes II III IV Non B cell group Grade 0 4(36.4%) 3(27.3%) 3(27.3%) Grade 1 2(10%) 5(25%) 7(35%) Grade 2 1(4.8%) 1(4.8%) 13(61.9%) Grade 3 0(0%) 0(0%) 4(80%) 7 9 27 V VI 1(9%) 0(0%) 4(20%) 2(10%) 2(9.5%) 4(19%) 0(0%) 1(20%) 7 7 6(30%) 1(4.8%) 1(20%) 14 9(45%) 5(25%) 7(33.3%) 13(61.9%) 0(0%) 4(80%) 20 23 2(18.2%) 3(15%) 1(4.8%) 0(0%) 6 8(72.7%) 12(60%) 10(47.6%) 1(20%) 31 1(9.1%) 5(25%) 10(47.6%) 4(80%) 20 11(100%) 0(0%) 0(0%) 12(60%) 7(35%) 1(5%) 3(14.3%) 15(71.4%) 3(14.3%) 0(0%) 2(40%) 3(60%) 26 24 7 P =0.0001(Sig) 2(18.2%) 3(27.3%) 0(0%) 6(54.5%) 0(0%) 3(15%) 1(5%) 16(80%) 0(0%) 1(4.8%) 1(4.8%) 19(90.1%) 0(0%) 1(20%) 0(0%) 4(80%) 2 8 2 45 P=0.019 (Sig) 9(81.8%) 2(18.2%) 9(45%) 11(55%) 4(19%) 17(81%) 0(0%) 5(100%) 22 45 p= 0.0001(Sig) 11 20 21 5 57 Activity index Moderately 6(54.5%) active Active 4(36.4%) Extremely 1(9.1%) active Chronicity index No chronic changes Weak chronic changes Widespread chronic changes Inflammator y infiltrate Mild (+1) Moderate (+2) Severe (+3) Proteinuria +1 +2 +3 +4 Serum creatinin Normal Elevated Total P=0.003(Sig) P=0.0001(Sig) P=0.002(Sig) Page 13 - There was no significant statistical correlation between progression and activity index of lupus nephritis. As it had been found that 50% of non progressors and 40% of progressors were extremely active LN. So, progression is not associated with increase in the AI (P value>0.05). - There was a significant statistical correlation between progression and chronicity index of LN .As seventy five percent (75%) of non progressors were without obvious chronic changes while all progressors (100%) showed widespread chronic changes. (P value=0.0001) (Table 3). - There was a borderline significant statistical correlation between progression of the disease and the interstitial inflammatory infiltrate, as 75% of non progressors have mild (+1) infiltrate while the progressors shows more infiltrate as 60% have (+2) infiltrate and 20% have +3 infiltrate (P value=0.079) (Table 3). - There was no significant statistical correlation between progression of lupus nephritis and proteinuria. As seventy five percent (75%) of non progressors and 90% of progressors have (+4) proteinuria (P value >0.05) (Table 3). - There was a significant statistical correlation between progression of lupus nephritis and grades of B:T cell infiltrates as 25% of non progressor were grade 0 (non-B cell group) and 62.5% of the same group were grade (1) while all prorgressors were in the B &T cell group (B- cell group) ( P value=0.006) (Table 3). Page 14 Table (3): progression of lupus nephritis in relation to clinicopathologic variables and B & T cell grades: Variable LN classes Class III Class IV Class V AI Moderately active Active Extremely active Progression of LN Non Progressor progressor Significance Total 2(25%) 6(75%) 0(0%) 2(20%) 7(70%) 1(10%) 4(22.2%) 13(72.2% 1(5.6%) P>0.05(Insig) 0(0%) 2(20%) 2(11.1%) P>0.05(Insig) 4(50%) 4(50%) 5(40%) 4(40%) 8(44.4%) 8(44.4%) 6(75%) 2(25%) 0(0%) 0(0%) 6(33.3%) 2(11.1%) 0(0%) 10(100%) 10(55.6%) 6(75%) 1(12.5%) 1(12.5%) 2(0%) 6(60%) 2(20%) 8(44.4%) 7(38.9%) 3(16.7%) P=0.079(borderline sig) 1(12.5%) 1(12.5%) 6(75%) 1(10%) 0(0%) 9(90%) 2(11.1%) 1(5.6%) 15(83.3%) P >0.05(Insig) 2(25%) 0(0%) 2(11.1%) P =0.006(Sig) 5(62.5%) 1(12.5%) 0(0%) 3(30%) 4(40%) 3(30%) 8(44.4%) 5(27.8%) 3(16.7%) 8 10 18 CI No changes Weak chronic changes Widespread chronic changes Inflammatory infiltrate Mild(+1) Moderate(+2) Severe(+3) Proteinuria +2 +3 +4 B & Tcell grades Non B cell group B cell group Grade 1 Grade 2 Grade 3 Total P=0.0001(Sig) Page 15 Discussion: Lupus nephritis is an immune complex GN & it is considered one of the most and serious complication of SLE (Lech & Anders., 2013). Up to 60% of SLE patients develop lupus nephritis (Hseih et al., 2011). The pathogenesis of lupus nephritis involves a variety of pathogenic mechanisms. Although the pathogenesis of lupus nephritis is not clear, production of pathogenic antibodies is traditionally viewed as the principle contribution of B cells to the pathogenesis of immunemediated glomerulonephritis. However, it is increasingly appreciated that B cells have a much broader role in such diseases, functioning as antigen-presenting cells, regulators of T cells, macrophages, and dendritic cells, as well as being involved in the formation of local lymphatic expansion (Shen et al., 2012). In this study the mean age of studied cases was 28.05 and SD was ±9.01, and the majority of cases was in the second and third decades. This agrees with Rus et al (2007) and Brent et al (2014); who reported that LN patients typically occurs in patients aged 20-40 years. In agreement with our results Sada & Makino (2009), Arfaj et al (2009), Brent et al (2014) and Satirapoj et al (2015) found that female to male ratio was nearly 9:1 and this may be explained by that endogenous sex hormones have a role in disease predisposition. Currently; very few publications are available concerning the demographic, clinical, and pathological features of LN and their correlations in developing countries (Shariati-Sarabi et al; 2013, Chen et al; 2014 and Satirapoj et al.; 2015). Page 16 In this study; the activity index of LN was increasing from class II to class IV, while 57.1% of class V were active LN, whereas, 57.1% and 42.9% of class VI were moderately active and active LN respectively, and although the results were statistically insignificant; yet from the table 66.7% of class III were active and 74.1% of class IV were extremely active. Similar to our results; Satirapoj et al (2015) found that class III and IV had a higher activity index. This may be explained by the fact that Class V showed no residual activitiy unless it is combined with III or IV and class VI is advanced sclerosing lesions. This study showed that CI was progressing with higher classes, as 71.4% of class II and 66.7% of class III showed weak chronic changes; while 71.4% and 71.4% of class V and VI respectively showed widespread chronic changes and the results were statistically significant. This result was parallel to that of Nasri et al (2014) & Satiroapoj et al (2015) & Fugo et al (2014). This could be explained by; as the lupus nephritis disease progress from class I to class VI the activity index decrease while chronicity index increase to be the highest in class VI which is termed advancing sclerosing lupus nephritis. However Hseih et al (2011) study showed that ISN/RPS Class III or IV proliferative nephritis was somewhat more common in subjects with severe interstitial nephritis (which had +3 inflammatory infiltrate), our study revealed that the score of interstitial inflammatory infiltrate was increasing with higher classes as 71.4% of class II showed +1 inflammatory infiltrate while 100% of class VI showed +3 inflammatory infiltrate (P value = 0.004). Thus, the study concluded that severe interstitial nephritis may be widespread regardless of ISN/RPS lupus nephritis class and this could be explained by the pathogenesis of glomerular and interstitial pathology in lupus nephritis had different mechanisms (Chan et al., 2007). Page 17 This study revealed that proteinuria may be high regardless the class of lupus nephritis as patients in class II,III,IV,V,VI were 42.9%, 88.9%, 85.5%, 85.9, 100% respectively had +3 & +4 proteinuria (significant statistical correlation P value=0.003) ,and this also had been observed by Makni et al (2009). This finding could be explained by that podocytes are highly specialized epithelial cells that form part of the filtration barrier in the kidney, and their loss reflects a malfunction in glomerular filtration and result in loss of protein in urine (Bollian-y-Gotia et al; 2011). In agreement with Nezhad & Sepashkah (2008) and Satirapoj et al. (2015) studies; our study revealed significant statistical correlation between lupus nephritis classes and serum creatinine (P value= 0.003) as 71.4% of class II had normal serum creatinine and all the seven cases (100%) of class VI had elevated serum creatinine. This could be explained by predominant chronicity of these cases in form of diffuse global glomerulosclerosis, tubular atrophy and interstitial fibrosis is often will be associated with loss of renal function (elevated serum creatinine). So, we can concluded that serum creatinin and histologic evaluation of LN patients are important prognostic factors. There was significant statistical correlation between different classes of lupus nephritis and intrarenal B &T cells ((P value=0.003); as high grades of B&T cell infiltrate (grade 2&3) were mainly in class IV) agrees with Shen et al (2012) and Sun et al (2013) studies who noted that the B cell infiltration was more likely to be associated with class IV LN (the most aggressive class). This could be explained by that pathogenic B cells have a variety of functions such as producing autoantibodies that can cause renal damage via disruption of cellular functions, cytotoxicity mediated by interactions with complement and release of inflammatory mediators. And MRL/lpr lupus-prone mice that have B cells unable Page 18 to secrete antibodies still develop nephritis, this may indicate that there are additional B-cell functions, such as antigen presentation and activation of pathogenic T cells and proinflammatory cytokine production which contribute to kidney injury (Nowling & Gilkeson., 2011). Expression of B:T cell infiltrates was increasing in ascending manner with activity and chronicity indices (P value = 0.0001,0.002 respectively); as 54.5% of non B –cell group had low AI (Active LN) and 72.7% of non B-cell group showed weak chronic changes while 80% of grade 3 had a higher AI (Extremely active LN) and widespread chronic changes and this result was in line with Shen et al (2012) study. This finding suggest the role of B & T cell infiltrates in increasing the inflammatory process in lupus nephitis as Apostolidis et al (2011) reported that mechanisms by which T cells contribute to tissue injury include activating and providing help to nephritogenic antibody-producing B cells, recruiting macrophages and dendritic cells (DCs), and producing cytokines. It was not a striking finding when we found that B:T cell infiltrates correlated with the extent of inflammatory infiltrate (as it is a part of a whole) (p value = 0.0001). Hseih et al (2011) study confirms this finding and this increases the suggestion of the dominant roles of B and T cell infiltrates in pathogenesis and progression of lupus nephritis. Although there was a significant statistical correlation between B:T cell infiltrates and proteinuria (p value = 0.019), it may not be considered a true significancy as 54.5% of the non B-cell group and 80% of grade 3 had (+4) proteinuria. This result against Sun et al (2013) study, which found that the level of proteinuria (g/24 hours) in grade 0 was lower than other grades. It could be explained by that proteinuria is highly variable and reversible clinical presentation. This finding may suggest the role of B and T cells in prtoteinuria as recruitment of Page 19 B & T cells occur parallel to binding of podocytes to dsDNA which cause widespread, segmental effacement of podocyte foot processes that leads to proteinuria (Nowling & Gilkeson; 2011 , Yung & Chan; 2012). About eighty two percent of non B- cell group had normal serum creatinine, while all cases of grade 3 had elevated serum creatinine. There was a significant statistical correlation between B:T cell aggregates and serum creatinine level (p value = 0.0001). Shen et al (2012), Sun et al (2013) studies were in line with us. It may be explained by that B cells serve as a local immune system & have an important role in deteriorating renal function in lupus nephritis & in progression of renal diseases; Shen et al (2012) was beside my suggession and reported that intrarenal B cells form part of a local system that enhances the immunological response by functioning as antigen presenting cells, and as a source of cytokines promoting T cell proliferation and lymphatic neoangiogenesis. In this way, intrarenal B cells could aggravate the local immune response to persisting autoantigens in the tubulointerstitium, resulting in persistence and chronicity of renal inflammation. And this explanation could be confirmed by Sarwal et al (2003) and Heller et al (2007) studies which confirm the role of B cells in deteriorating renal function by demonstrating that the accumulation of CD 20 positive B cells in the tubulointerstitium was associated with steroid resistant acute allograft rejection and graft loss. B cells are recruited in the kidney via specific chemokines such as BCA1/CXCL13 and its specific receptor CXCR5, and local expression of B-cell survival factors such as APRIL and BLyS (which are important factors for intrarenal B cells in lupus nephritis patients). Antagonists of these chemokines, such as anti-BAFF/BCA-1 antibodies or corresponding receptors may have Page 20 therapeutic efficacy in patients with autoimmune disorders of this type (Neusser et al., 2011). In agreement with Kiremitci and Ensari (2014) who reported that the ISN/RPS classification provided significant advances in the handling of renal biopsies of SLE patients, but does not sufficiently stress the involvement of nonglomerular compartments such as the tubulointerstitium which may also be related to the prognosis, as 90% of progressors and all (100%) non progressors were in class III & IV. There was no significant statistical correlation between class and progression, and this suggests that class could not predict renal outcome in lupus nephritis patients and another factor is needed. Also Dolff et al (2010) and Hseih et al (2011) reported that Class III and IV LN have several pathogenic and histopathological similarities and patients with these types of LN share a poor long term renal survival due to deterioration of kidney function. So; the aim of clinical & the first therapeutic goal is to reduce disease activity and to restore renal function or to prevent deterioration in both classes of lupus nephritis. Our result revealed that AI provided no prognostic value in LN progression; as there was no significant statistical correlation between AI and progression of lupus nephritis (P>0.05). (50%) of non progressors and (40%) of progressors showed extremely active LN. This result agrees with Hseih et al (2011) and Jaipaul (2013) studies but against Kammoun et al (2011) study which revealed that high AI has been shown to predict poor renal outcome in LN patients. This could be explained by that the activity score is based on the degree of glomerular inflammation, which is more reversible with treatment. The chronicity index was increasing with progression of lupus nephritis (P = 0.0001); as 75% of non progressors showed no obvious chronic changes and all progressors 100% had widespread chronic changes. Parallel to us Hseih et al Page 21 (2011) and Jaipaul (2013) reported that the chronicity index predicts progression of lupus nephritis to renal failure; and this could be explained by the fact that crescent formation, glomerular sclerosis, tubular atrophy and interstiatial fibrosis are entities of CI will impair creatinine clearance with subsequent elevated serum creatinine. Nasri et al (2014) confirm this suggestion by finding that the serum creatinine (which progression in our study is based on) positively correlated with proportion of glomeruli with crescents. The progression occurs by contribution of anti-ds DNA antibody (main antibody in LN) into tubulo-interstitial fibrosis in lupus nephritis by induction of both cell-associated and soluble fibronectin secretion in (proximal tubular epithelial cells) PTEC, the former adds to extracellular matrix deposition while the latter amplifies the fibrotic process through induction of TGF-β1 and collagen type I (Yung et al., 2015). Parallel to Makni et al (2009); our result revealed no significant statistical correlation between proteinuria and progression of lupus nephritis (p>0.05),so proteinuria could not used as an indicator for progression of LN. However Falk et al (2014) reported that proteinuria may have a role in pathogensis of progression of renal diseases based on response of the renal tubules to proteinuria, as it causes increased tubular synthesis of macrophagic and other chemokines, with increased tubular cellular proliferation and apoptosis, (apoptosis more than proliferation) leading to interstitial inflammation and fibrosis. So, medical controlling and diminution of proteinuria may leads to slowing of progression. Grades of B:T cell aggregates and interstitial inflammatory infiltrate was increasing with progression of LN cases (P value = 0.006, 0.079 respectively), as 25% of the non progressor group was (grade 0) (non B-cell group) and 62.5%was grade 1, while 70% of the progressor group were grade 2 and grade 3(a significant statistical correlation). This result runs parallel to Yu et al (2010) and Bagavant Page 22 & Fu (2009) studies. The current study suggets importance of intrarenal B cells in progression of lupus nephritis as it can be used as a predictor for progression. This study suggested that B cells may have a role in interstitial fibrosis; However; little was known about the role of B cells in the process of renal interstitial fibrosis, as Heller et al (2007) study support our hypothesis by demonstrating that a model of CCI4-induced liver fibrosis approximately half of the infiltrating cells in the liver were found to B cells. Eliminating B cells significantly improved liver injury with decreases collagen deposition. This improvement was not T-cell or immunoglobulin-dependent. It may be explained by that B cells might be involved in interstial injury through release of cytokines and chemokines, as antigen-presenting cells, via augmentation of T-cell responses and through neolymphogenesis. Regarding kidney, Sun et al (2013) described the high prevalence of intrarenal B cells in immune mediated diseases, including renal transplant rejection and glomerulonephritis, local B-cell infiltrates could play a role in tissue injury such as fibrosis, neolymphangiogenesis, and ectopic lymphomagenesis by deposition of immune complexes and/or autoantibodies which induce the secretion of cytokines in the renal resident cells, which promote the infiltration and activation of leukocytes (T & B cells) which also produce cytokines that leads to the further immune response and disease progression . Conclusion: The present work reported that the presence of intrarenal B & T cell infiltrates and their classification into grades according to microanatomical organization in patients suffered from lupus nephritis could suggest the role of intrarenal B & T lymphocytic infiltrates in pathogenesis and progression of lupus nephritis. Page 23 The current study revealed that the non B-Cell group (grade 0) had lower histopathological and clinical parameters, while different grades of the B-Cell group had elevated histopathological and clinical parameters in ascending manner with CD20 & CD3 expression. This finding may suggest the role of B cell in deteriorating the histopathological and clinical conditions of the patient. This finding suggests that trials of treatment with anti CD20 may provide a new strategy in management of LN especially in resistant cases to the ordinary medical protocol. Figure (1): shows negative immunohistochemical staining of CD20 in LN, grade 0 (non-B cell group). (CD20 ×400). Page 24 Figure (2): shows immunohistochemical staining of CD3 in previous case of LN: scattered positive T cells (grade 0) (CD3 ×400). Figure (3): shows immunohistochemical staining of CD20 in LN, cluster like structure of CD20 positive B cells (grade 2) (CD20 ×400). Page 25 Figure (4): shows immunohistochemical staining of CD20 in LN: clearly distinguishable zone of CD20 positive B cells (grade 3)(CD20 ×400). Figure (5): shows immunohistochemical staining of CD3 in previous case of LN, clearly distinguishable zone of CD3 positive T cells (grade 3) (CD3 ×400). Page 26 Refrences: Apostolidis SA, Crispin JC, Tsokos GC: IL-17-producing T cells in lupus nephritis. Lupus. 2011; 20(2):120-124. Austin HA, Muenz LR, and Joyce KM, et al. Prognostic factors in lupus nephritis. Contribution of renal histologic data. Am J Med.1983; 75(3)382:391. Bagavant H and Fu S M. Pathogenesis of kidney disease in systemic lupus erythematosus. Curr Opin Rheumatol. 2009; 21(5) 489:494. Chang A, Henderson SG, Brandt D, et al. In situ B cell-mediated immune responses and tubulointerstitial inflammation in human lupus nephritis.J Immunol .2011;186(3)1849:1860. Crow MK. Etiology and pathogenesis of systemic lupus erythematosus. Kelley's Textbook of Rheumatology. 9th ed; 2013:chap 79. De Zubiria Salgado A and Herrera-Diaz C. Lupus Nephritis: An Overview of Recent Findings. Autimmune Dis J. 2012. Dooley MA.Clinical and laboratory features of lupus nephritis. Dubois' Lupus Erythematosus. 7th ed. Chapter 56.2007;1112:11130. Faull R. "Prescribing in renal disease". Australian Prescriber .2007;30 (1)17:20. Gomaa W, Bahla S, Habhab W, et al. Clinicopathological characteristics of lupus nephritis in Western region of Saudi Arabia: An experience from two tertiary medical centres . Journal of Microscopy and Ultrastructure. 2014; 2( 1) 12:19. Heller F, Lindenmeyer MT, Cohen CD, et al. The contribution of B cells to renal interstitial inflammation. Am J Pathol. 2007 ; 170(2)457:468. Hseih C., Chang A., Brandt D., et al. Tubulointerstitial inflammation and scarring predict outcome in lupus nephritis.NIH Public Access.2011;63(6):865874. Hutloff A, Büchner K, Reiter K, et al. Involvement of inducible costimulator in the exaggerated memory B cell and plasma cell generation in systemic lupus erythematosus. Arthritis Rheum. 2004 ; 50(10):3211-3220. Page 27 JaipaulN.Lupusnephritis.2014 ;http://www.merckmanuals.com/professional/genitourinarydisorders/glomerula r-disorders/lupus-nephritis 74(4)448:457. Kammoun K, Jarraya F, Bouhamed L,et al. Poor Prognostic Factors of Lupus Nephritis. Saudi J Kidney Dis Transpl .2011;22(4)727:732. Kiremitci S and Ensari A. Classifying Lupus Nephritis: An Ongoing Story. he Scientific World Journal.Volume 2014 (2014). Lech M & Anders H J .The pathogenesis of lupus nephritis. J Am Soc Nephrol. 2013; 24 (9)1357:1366. Makni K, Jarraya F, Khabir A, et al.Renal α-smooth muscle actin:A new prognostic factor for lupus nephritis. Nephrology (carlton).2009;14(5):499-505. Neusser MA, Lindenmeyer MT, Edenhofer I, et al. Intrarenal production of Bcell survival factors in human lupus nephritis.Mod Pathol. 2011;24(1)98:107. Nowling T K & Gilkeson G S. Mechanisms of tissue injury in lupus nephritis. Arthritis Research & Therapy. 2011; 13(6)250:259. Ramanujam M, Bethunaickan R, Huang W, et al. Selective blockade of BAFF for the prevention and treatment of systemic lupus erythematosus nephritis in NZM2410 mice. Arthritis Rheum. 2010 ; 62(5)1457:1468. Sada KE and Makino H. Usefulness of ISN/RPS Classification of Lupus Nephritis. Japan J Korean Med Sci .2009; 24 ( 1)7:10. Sarwal M, Chua MS, Kambham N, et al.Molecular heterogeneity in acute renal allograft rejection identified by DNA microarray profiling. N Engl J Med. 2003 Jul 10; 349(2)125:138. Shen Y, Sun C Y, Wu F X, et al.Association of intrarenal B-Cell infiltrates with clinical outcome in lupus nephritis. Journal of Immunology Research. Clinical and Developmental Immunology. Volume 2012 (2012). Steinmetz OM, Velden J, Kneissler U, et al. Analysis and classification of B cell infiltrates in lupus and ANCA-associated nephritis. Kidney Int. 2008; Page 28 Sun C Y, Shen Y, Chen X W, et al.The charachteristics and significance of locally infiltrating B cells in lupus nephritis and the association with local BAFF expression.International journal of rheumatology. Volume 2013 (2013). Wang A, Guilpain P, Chong BF, et al. Dysregulated expression of CXCR4/CXCL12 in subsets of patients with systemic lupus erythematosus. Arthritis Rheum. 2010; 62(11)3436:3446. Weening JJ, D’Agati VD, Schwartz MM, et al.The classification of glomerulonephritis in systemic lupus erythematosus revisited. J Am Soc Nephrol ; 15 (2)241:250. Yu F, Wu LH, Tan Y, et al. Tubulointerstitial lesions of patients with lupus nephritis classified by the 2003 International Society of Nephrology and Renal Pathology Society system. Kidney Int. 2010; 77(9)820:829. Yung S, Ng CY, Ho SK, et al. Anti-dsDNA antibody induces soluble fibronectin secretion by proximal renal tubular epithelial cells and downstream increase of TGF-β1 and collagen synthesis. J Autoimmun. 2015; 58; 111:122. Page 29