Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Separation anxiety disorder wikipedia , lookup
Excoriation disorder wikipedia , lookup
Alcohol withdrawal syndrome wikipedia , lookup
Autism spectrum wikipedia , lookup
Antipsychotic wikipedia , lookup
Major depressive disorder wikipedia , lookup
Mental disorder wikipedia , lookup
History of mental disorders wikipedia , lookup
Bipolar disorder wikipedia , lookup
Bipolar II disorder wikipedia , lookup
Panic disorder wikipedia , lookup
Rumination syndrome wikipedia , lookup
History of psychiatry wikipedia , lookup
Mental status examination wikipedia , lookup
Antisocial personality disorder wikipedia , lookup
Abnormal psychology wikipedia , lookup
Conduct disorder wikipedia , lookup
Depersonalization disorder wikipedia , lookup
Classification of mental disorders wikipedia , lookup
Child psychopathology wikipedia , lookup
Generalized anxiety disorder wikipedia , lookup
Factitious disorder imposed on another wikipedia , lookup
Spectrum disorder wikipedia , lookup
Glossary of psychiatry wikipedia , lookup
Emergency psychiatry wikipedia , lookup
Schizoaffective disorder wikipedia , lookup
Narcissistic personality disorder wikipedia , lookup
Diagnostic and Statistical Manual of Mental Disorders wikipedia , lookup
Asperger syndrome wikipedia , lookup
Controversy surrounding psychiatry wikipedia , lookup
Dissociative identity disorder wikipedia , lookup
PREMENSTRUAL DYSPHORIC DISORDER AND THE CONTROVERSY OVER
DIAGNOSIS AND TREATMENT
By
KATIE SOREY
A dissertation/thesis submitted in partial fulfillment of
the requirements for the degree of
MASTERS OF NURSING
WASHINGTON STATE UNIVERSITY - SPOKANE, WA
College of Nursing
AUGUST 2011
Washington State University Spokane
Riverpoint Campus Library
Academic Center, Suite 211
PO Box 1495
Spokane, WA 99210-1495
To the Faculty of Washington State University:
The members of the Committee appointed to examine the master's project of
KATIE SOREY find it satisfactory and recommend that it be ac.cepted.
ii
PREMENSTRUAL DYSPHORIC DISORDER AND THE CONTROVERSY OVER
DIAGNOSIS AND TREATMENT
Abstract
by Katie Sorey, BSN
Washington State University
August 2011
Chair: Lorna Schumann
Premenstrual dysphoric. disorder has received great attention and c.ontroversy
since it was first adapted into the DSM IV in 1994. Since that time, treatment options
have stolen the spotlight, and limited focus has occurred on the actual disorder. The
diagnosis of premenstrual dysphoric disorder (PMDD), risks and benefits of the
diagnosis, and alternative treatment modalities used in a clinical setting will be reviewed
in this manuscript. The most alarming risk of the diagnosis includes a misdiagnosis and
the possibility of covering up an underlying condition. The major benefit of correct
diagnosis is likely improvement of health related quality of life through symptom control
and management.
A major problem is that accurate diagnostic screening tools are not being utilized
properly and effectively in the clinical setting. The treatment ofPMDD is diverse and
complicated. If the appropriate diagnostic measures are not taken an underlying medical
condition, including a psychiatric diagnosis may be missed. In the clinical setting this is
important, because approximately 5-8% of the female population is affected by
premenstrual dysphoric disorder, which is proven to have a significant effect on lifestyle,
work function, relationships, and social interaction. By appropriately diagnosing this
iii
disorder, and using evidence based practice to treat, the symptoms can be controlled and
burdens on activities of daily living can be lifted.
Keywords: Premenstrual dysphoric disorder, underlying psychiatric conditions,
misdiagnosis, premenstrual syndrome
iv
TABLE OF CONTENTS
Page
iii
ABSTRACT
INTRODUCTION
1
Search Strategies
2
Theoretical Framework
3
LITERATURE REVIEW
Pathophysiology
3
Diagnostic Criteria
4
Assessment ofPMDD
5
Non-pharmacological Treatments
7
Pharmacological Treatments
9
SIGNIFICANCE OR IMPLICATIONS FOR PRACTICE
Summary
12
13
REFERENCES
14
APPENDIX
A. DAILY SYMPTOM REPORT
16
B. DAILY RECORD OF SEVERITY OF PROBLEMS
17
v
Running Head: PREMENSTRUAL DYSPHORIC DISORDER CONTROVERSY
1
Premenstrual Dysphoric Disorder and the Controversy over Diagnosis and Treatment
Introduction
Premenstrual dysphoric disorder was formalized into the Diagnostic and Statistical
Manual of Mental Disorders, or DSM-IV in 1994. PMDD is stated to affect 5-8% of tIle
female population (Pearlstein & Steiner, 2008). Premenstrual dysphoric disorder is
defined as a psychiatric disorder with biological, psychological, and sociocultural
components (Dipiro et aI., 2008). PMDD is costly to society and the diagnosis and
treatment have been controversial.
Premenstrual dysphoric disorder places a high burden on quality of life as well as
cost to society. A cross-sectional study was conducted to compare women at risk for
PMDD with other chronic conditions such as hypertension, type 2 diabetes, depression,
and back pain. The study population consisted of 971 multiethnic women. The results
show that women at risk for PMDD report a lower functioning and well-being in all
physical and mental health domains (Yang et aI., 2008). The burden ofPMDD was
reported highest in general pain and social functioning. The conclusion of this study
suggests that PMDD places a substantial burden on both physical and mental health
aspects that can affect health related quality of life more than type 2 diabetes,
hypertension, osteoarthritis, rheumatoid arthritis, and are somewhat comparable to
depression (Yang et aI., 2008). The study's limitation is the retrospective nature of data
collection. Also, the validity of online data collection is also questionable.
Another burden present is the high ec·onomic· indirect cost. In 2005, a quantifiable
self- study collected data from 374 women that correlated indirect costs, such as missed
work or decreased productivity, to premenstrual symptoms that totaled approximately
PREMENSTRUAL DYSPHORIC DISORDER CONTROVERSY
2
$4,300 annually (Borenstein, Chiou, Dean, Wong, & Wade, 2005). Other burdens can
include decrease in effectiveness at work or school, a disturbed marital relationship,
difficulty parenting without distraction, and increased doctor visits for symptom control
(Pearlstein & Steiner, 2008). Due to the fact that the quantifiable data was reported by the
participants the accuracy is questionable.
In 1994, controversy sparked on the diagnosis of premenstrual dysphoric disorder,
when it was added into the Diagnostic and Statistical Manual of Mental Disorders, or DSM
IV
(Che~
2008). "Women's health activists argued that the diagnosis pathologized the
menstrual cycle and would stigmatize many women by wrongly labeling them mentally
ill, and put them in jeopardy of discrimination at the workplace or in child custody
battles" (Chen, 2008). Today, controversy surrounds the diagnosis ofPMDD, because
experts argue that PMDD may cover up an existing psychiatric condition. PMDD should
generally not be diagnosed when an underlying psychiatric disorder is present because
many of these conditions can be exacerbated by premenstrual symptoms (Pearlstein &
Steiner, 2008).
There is thought that with dietary and lifestyle changes medication may not be
needed to treat symptoms ofPMDD. The question that presents and should be asked is: Is
the diagnosis ofPMDD over used, and could it be managed efficiently with dietary,
lifestyle, and non-pharmacological agents? The purpose of this literature review is to
identify the appropriate methods of assessment and diagnosis of premenstrual dysphoric
disorder and identify alternative methods of symptom management.
Search Strategies
Search strategies used to obtain research literature correlating to PMDD included
PREMENSTRUAL DYSPHORIC DISORDER CONTROVERSY
3
the use of CINAHL, Medscape, and PubMed search engines. The keywords searched
included PMDD, controversy, diagnosis, and treatment. With these keywords
approximately four pages of articles resulted in each search engine. Of these articles the
most applicable, scholarly, and peer reviewed journals were utilized. Integrated in this
literature review are seventeen articles that summarize the most recent and clinical
applicable data.
Theoretical Framework
Symptoms ofPMDD including depression can directly and indirectly impact a
patient's appraisal and outlook of their situation. In tum, the patient's appraisal is
impacted by personality factors, social support, and coping skills. These variables
determine the health outcome for the patient. Health outcomes would include medical
treatment, inability to function to carry out employment or other activities of daily living,
health related quality of life, and overall mood. Therefore, the structural framework will
incorporate symptoms of PMDD, as well symptom management, and their impact on
health outcomes.
Literature Review
Pathophysiology
The pathophysiology of PMDD is closely linked to an active hypothalamic.
pituitary- gonadal axis (HPG). Somatic and physical symptoms are thought to be brought
on by changes in the ovarian cycle (Steiner et aI., 2006). The etiology ofPMDD is still
being investigated. An allelic variation on the estrogen receptor alpha gene in women
with PMDD may be the source of abnormal estrogen signaling during the luteal phase
PREMENSTRUAL DYSPHORIC DISORDER CONTROVERSY
4
that leads to premenstrual affective, cognitive, and somatic symptoms (Pearlstein &
Steiner, 2008).
In a 2008 cross-sectional and prospective experimental study, that included a two
month self assessment and one month hormonal evaluation, it was identified that serum
concentration of free estradiol (E2), percent free E2, and sex hormone-binding globulin
(SHBG) are markedly different in women with PMDD, as opposed to women without
PMDD (Thys-Jacobs, McMahon, & Bilezikian, 2008). During the luteal phase, free E2
was significantly lower in the PMDD group when compared with controls. "Acute
changes in ovarian function or even relatively lower estrogen concentrations during the
luteal phase of the menstrual cycle may influence serotonergic metabolism and
neurotransmitter reuptake, both thought to mediate mood and emotion" (Thys-Jacobs,
McMahon, & Bilezikian, 2008, p. 99). In both follicular and luteal phases, SHBG was
higher in women with PMDD. '''Higher SHBG concentrations as noted in the PMDD
group may limit the bioavailability ofE2 to the brain, liver, and other tissues, and
ultimately affect mood" (Thys-Jacobs, McMahon, & Bilezikian, 2008, p. 100).
Conversely, levels ofLH, progesterone, E2, peak E2, and free E2 were not different
between the two groups. Therefore, appropriate labs to monitor in patients with PMDD
would include luteal phase estradiol, percent free E2, and SHBG. Limitations in this
study include a limited eight day monitoring of hormone levels, which may indicate that
certain trends may have been missed.
Diagnostic Criteria
According to the American Psychiatric Association, confirmation of the diagnosis
must be obtained by daily ratings for two consecutive menstrual cycles. Of the daily
PREMENSTRUAL DYSPHORIC DISORDER CONTROVERSY
5
information that is gathered, five or more symptoms must have occurred in the majority
of the cycles in the past year. These symptoms are broken up into core symptoms and
other symptoms (Wysocki, 2008). Core symptoms include a markedly depressed mood,
anxiety, affective lability, persistent anger or irritability, decrease in interest in usual
activities including work, school, friends, or hobbies, difficulty concentrating, insomnia,
change in appetite, and the sense of being overwhelmed. Other symptoms include
physical symptoms such as breast tenderness, swelling, weight gain, and joint or muscle
pain (Wysocki, 2008). For the diagnosis ofPMDD there needs to be at least one
symptom that is a core symptom. Symptoms must present in the last week of the luteal
phase, ease after a few days of menses, and resolve in the week post-menses. Also,
symptoms must be interfering with daily life. This can include relationships, work,
school, or other activities (Wysocki, 2008).
Assessment of PMDD
Assessment information for PMDD that can be useful in practice includes either
the Daily Record of Severity of Problems or the Penn Daily Symptom Report
(APPENDIX A & B). These are scoring methods that can be used to record daily ratings
of symptoms (Pearlstein & Steiner, 2008). These reports compare a patient's
premenstrual symptoms with post menses symptoms, and are used over a consecutive
two-month time frame to aid in the diagnosis ofPMDD. These tools also help rule out
differential diagnoses in the process. PMDD symptoms should increase from 30-50%
from the follicular phase to the luteal phase (Wysocki, 2008). The follicular phase is the
first half of the menstrual cycle that ranges from 10-14 days. It begins on the first day of
the menstrual bleed (Wysocki, 2008). During this phase there should be a resolution or
PREMENSTRUAL DYSPHORIC DISORDER CONTROVERSY
6
reduction in symptoms after the onset of menses."Ratings that demonstrate follicular
symptoms with increase symptom severity in the premenstrual phase suggest the
premenstrual exacerbation of an underlying disorder rather than PMDD" (First &
Tasman, 2010, p. 304). Common Axis 1 disorders that may be premenstrually
exacerbated include depression, anxiety, bipolar I, posttraumatic stress disorder, eating
disorders, and substance abuse disorders (First & Tasman, 2010).
In 2004, a self reported study was conducted to analyze 433 women to determine
if their depressive states were exacerbated premenses. The results indicated that women
who reported premenstrual exacerbation of symptoms had a prolonged duration of their
current depressive episode (Komstein et aI., 2005). The women who experienced
premenstrual exacerbation of symptoms also noted more somatic disturbance and
psychomotor dysfunction (Komstein et aI., 2005). If recorded symptoms are largely
confined to the premenstrual phase with relative absence during the follicular phase, then
the clinician should assess premenstrual function impairment (First & Tasman, 2010).
The limitation to this study is that retrospective rating was used, and it is argued that, in
the participants, the actual rates of premenstrual exacerbation (PME) may be somewhat
lower than those found in this study. "On the other hand, it is also possible that the lower
rate of PME· reported by women at the very times it was oc.c.urring is a function of altered
cognition or perception associated with premenstrual mood changes" (Komstein et aI.,
2005, p. 8).
Another important factor in the assessment ofPMDD is to order laboratory tests
to exclude differential diagnoses. These would include thyroid and glucose testing to rule
PREMENSTRUAL DYSPHORIC DISORDER CONTROVERSY
7
out conditions that may exhibit similar symptoms. A provider may also incorporate the
testing of luteal phase estradiol, percent free E2, and SHBG.
Non-pharmacological Treatments
Treatment for PMDD is comprised of collaboration between psychosocial
interventions, lifestyle change and modification, and pharmacological therapies. Experts
recommend that during the first two cycles, while the patient is gathering symptom
information, lifestyle changes be put into practice (Steiner et aI., 2006). An example of a
lifestyle change is alteration of diet, which includes the limitation of caffeine. Reducing
caffeine intake can decrease irritability.
A 2007 cross-sectional analysis by Gold et aI., reported that increasing caffeine
intake in a population of 3302 multiethnic, midlife women was associated with reporting
of premenstrual anxiety and mood changes, but the association was not monotonic (Gold
et aI., 2007). This study also indicated that greater fat intake was associated with less
premenstrual craving and bloating, possibly reflecting ingestion of comfort food to self
treat PMS symptoms (Gold et aI., 2007). Limitations of the study included the use of
statistical comparisons, therefore, some of the observed associations may have occurred
by chance or represent markers for other uncontrolled factors. Also, the symptoms
re-called by participants may lac·k accuracy (Gold et aI., 2007).
Increasing carbohydrate intake premenstrually has been shown to improve mood,
carbohydrate craving, and short term memory by elevating the serotonin level in the brain
(Steiner et aI., 2006). A randomized trial conducted in 2001, shows that a carbohydrate
rich beverage, PMS Escape, reduced PMS mood symptoms in one third of the 53
participants (Freeman, Stout, Endic.ott, & Spiers, 2002). The limitation to the study is that
PREMENSTRUAL DYSPHORIC DISORDER CONTROVERSY
8
there is no significant group difference in demographic, physical characteristics, or
baseline daily symptom rating (DSR).
Vitamin intake is beneficial in treating premenstrual symptoms. Studies have
shown that Calcium 600 mg twice daily reduces emotional and physical symptoms of
PMDD. A double blind, randomized, placebo-controlled study conducted in 1998,
reveals that 1200 mg! day of calcium carbonate decreases all core PMS symptoms during
the luteal phase (Thys-Jacobs, Starkey, Berstein, & Tian, 1998). Of the 466 women
analyzed, 48% reported reduction in symptoms by the third treatment cycle. This occurs
most likely by the reduction of neuromuscular irritability and vascular reactivity (Thys
Jacobs, Starkey, Berstein, & Tian, 1998). The limitation to the study is that it investigated
women with PMS and not specifically premenstrual dysphoric disorder.
Natural remedies and supplements have also been evaluated in the treatment of
PMDD. In a 2006 biopharmaceutical scientific study, c-haste berry was proven as
effective in treating PMS symptoms. In this study two different vitex agnus-castus
extracts were analyzed for receptor binding and functional assays. Chaste berry or vitex
agnus-castus (VAC) has been proven to be clinically effective by acting on the opiate
pathway that plays a role in pain perception, mood, appetite, and other functions
(Webster, Lu, Chen, Farsworth, & Wang, 2006). "VAC may improve symptoms ofPMS
by activating opiate receptors to reverse the loss of opiate tonic inhibition or directly
activating analgesic and mood regulatory pathways" (Webster, Lu, Chen, Farsworth, &
Wang, 2006, p. 219). The limitation to this study is that it was evaluated for the treatment
ofPMS not specifically PMDD.
PREMENSTRUAL DYSPHORIC DISORDER CONTROVERSY
9
Education and psychosocial support information should also be given to the
patient in the beginning stages. Peer support, cognitive behavioral modifications,
relaxation exercises, stress reducing activities, and counseling may all be appropriate
interventions for the patient. A randomized trial, funded by the National Institute of
Health, studied 134 women in 1999 (Taylor, 1999). This study analyzed the use of
nonpharmacological approaches including self-monitoring, personal choice, self
regulation, and self/environmental modification with women diagnosed with severe
premenstrual symptoms. The results indicated that with these methods PMS severity was
reduced by 75% and premenstrual depression was reduced by 30-540/0. The most
improvement was found after 3 months but continued to show effectiveness long-term
(Taylor, 1999). The limitation to this study is the limited number of participants and that
it focuses on PMS instead ofPMDD.
Pharmacological Treatments
Pharmacological interventions may be considered, if the above methods have not
improved symptoms and if the appropriate assessment criteria is met in order to confirm
the diagnosis ofPMDD. The United States Food and Drug Administration (FDA) has
approved treatment ofPMDD with three selective serotonin reuptake inhibitors (SSRIs)
including Fluoxetine (Prozac), Sertraline (Zoloft), and controlled released Paroxetine
(Paxil CR). Also, one combined oral contraceptive, Ethinyl Estradiol/Drospirenone
(YAZ) has been approved by the FDA for treatment ofPMDD. Agents used off label
include gonadotropin-releasing honnone agonists, anxiolytics, and hormonal
interventions (Wysocki, 2008).
PREMENSTRUAL DYSPHORIC DISORDER CONTROVERSY
11
SSRIs interact with only one receptor so they have the advantage of fewer
associated side effects. However, side effects do include reduced libido, dysorgasmia,
nausea, weight gain, sweating, and headache. When using SSRIs in young adults and
adolescents, it is extremely important to monitor the risk of suicidal thinking and
behavior. Education is crucial with this matter. When treating an adolescent, consulting
with a child psychologist would he critical prior to treating them with SSRIs (Claman &
Miller, 2006). Also, following up with any abnormal lab values would be imperative to
rule out an underlying medical condition, such as anemia, autoimmune disorders,
endocrine and thyroid disorders (hyperprolactinemia, hypothyroidism, diabetes mellitus),
chronic fatigue syndrome, endometriosis, and psychiatric disorders (Claman & Miller,
2006). Further research acknowledging long term effects with the use of SSRls for the
treatment ofPMDD is necessary. Research regarding the use ofSSRls in the adolescent
population, diagnosed with PMDD, would be informative and applicable in the clinical
realm.
The combined oral contraceptive approved by the FDA for the treatment of
PMDD is YAZ. "It contains 3mg of progestin drospirenone and 20 mcg of ethinyl
estradiol (DRSP/EE)" (Wysocki, 2008, p. 28). Studies have shown that YAZ is effective
in reducing mood, behavioral, and physical symptoms associated with PMDD. A double
blind, random clinical trial conducted in 2005, resulted in a 37.4 symptom decrease as
recorded on the Daily Record of Severity of Problems after a 24/4 regimen of
drospirenone 3 mg and ethinyl estradiol 20 mcg was given for three treatment cycles
(Yonkers et aI., 2005). The study population consisted of 450 women diagnosed with
PREMENSTRUAL DYSPHORIC DISORDER CONTROVERSY
12
premenstrual dysphoric disorder. Oral contraceptive agents can potentially change the
characteristics of a menstrual cycle, and therefore, can limit the accuracy of the study.
Taking oral contraceptives can cause adverse effects including breakthrough
bleeding, nausea, and breast pain (Wysocki, 2008). "The creation of a reliable and well
tolerated coe with an additional benefit of treating premenstrual disorders may be a
welcomed alternative for women suffering from PMDD, who are dissatisfied with the
side-effect profile of SSRIs or fail to respond to SSRIs" (Rapkin, McDonald, & Wilner,
2007, p. 408).
Significance or Implications for Practice
The diagnosis of premenstrual dysphoric disorder has significant implication for
practice, because it has been proven that PMDD can dramatically influence health related
quality of life and be a burden financially, emotionally, and physically if not diagnosed
and treated. The appropriate methods of assessment include either the Daily Record of
Severity of Problems or the Penn Daily Symptom Report (APPENDIX A & B). During
the two full cycles in which that information is being gathered, the first and primary
method of treatment should be lifestyle and diet modification, while ruling out any
differentials. Once the follow-up interview has been completed, previous methods have
not improved symptoms, and the patient meets diagnostic. criteria they should be
considered for pharmacological treatment options. These options should begin with an
SSRI or the combined oral contraceptive, YAZ, depending on their symptoms and
treatment desires. Each patient should be treated individually and assessed thoroughly,
because treatment should not be the same for everyone.
PREMENSTRUAL DYSPHORIC DISORDER CONTROVERSY
13
Summary
Five to eight percent of the female population struggle with premenstrual
dysphoric disorder and exhibit physical, social, and emotional burdens from this
condition. With correct assessment by health care providers including the use of daily
symptom reports over two consecutive months' menstrual cycles, this diagnosis can be
correctly identified. The first line pharmacological treatment for the disorder is an SSRI.
The second line of treatment is either YAZ or an additional SSRI. Changes in lifestyle
and diet can also be made to achieve relief in symptoms and should be a primary
intervention. The biggest concern for health care providers is to rule out differential
diagnoses that may be covered up or exacerbated by premenstrual symptoms.
PREMENSTRUAL DYSPHORIC DISORDER CONTROVERSY
14
References
Borenstein, J., Chiou, C., Dean, B., Wong, l., & Wade, S. Estimating direct and indirect
costs of premenstrual syndrome. Journal ofOccupational & Environmental
Medicine. 2005, 47(1), 26-33.
Chen, I. (2008). A class of science and politics over PMS. The New }Tork Times.
Retrieved March 25, 2011 at http://www.nytimes.com/ref/health/healthguide/esn
pms-ess.html
Claman, F., & Miller, T. Premenstrual syndrome and premenstrual dysphoric disorder in
adolescence. Journal ofPediatric Health Care. 2006, 20(5), 329-333.
Dipiro, l., et ala (2008) Pharmacotherapy: a pathophysiologic approach. McGraw-Hill
Companies, Inc. New York.
First, M., & Tasman, A. (2010). Clinical guide to the diagnosis and treatment ofmental
disorders. West Sussex, UK: John Wiley & Sons.
Freeman, E., DeRubeis, R., & Rickels, K. Reliability and validity of a daily diary for
premenstrual syndrome. Psychiatry Research. 1996,65,97-106.
Freeman, E., Stout, A., Endicott, J., & Spiers, P. Treatment of premenstrual syndrome
with a carbohydrate-rich beverage. International Journal ofGynecology &
Obstetrics. 2002, 77, 253-254.
Gold, E., et al. Diet and lifestyle factors associated with premenstrual symptoms in a
racially diverse community sample: Study of women's health across the nation
(SWAN). Journal of Women's Health. 2007, 16(5),641-655.
Komstein, S., et aI. Self reported premenstrual exacerbation of depressive symptoms in
patients seeking treatment for major depression. Psychological Medicine. 2005,
35, 1-10.
Pearlstein, T., & Steiner, M. Premenstrual dysphoric disorder: Burden of illness and
treatment update. Journal ofPsychiatry & Neuroscience. 2008, 33(4), 291-301.
Rapkin, A., McDonald, M., & Wilner, S. Ethinyl estradiol/ drospirenone for the treatment
of the emotional and physical symptoms of premenstrual dysphoric disorder.
Women's Health. 2007, 3(4), 395-408.
Steiner, M., et ala Expert guidelines for the treatme·nt of severe PMSS, PMDD,
and comorbidities: the role ofSSRI's. Journal a/Women's Health. 2006,15(1),
57-68.
PREMENSTRUAL DYSPHORIC DISORDER CONTROVERSY
15
Steiner, M., et ale Luteal phase administration of paroxetine for the treatment of
premenstrual dysphoric disorder. Journal ofClinical Psychiatry. 2008, 69(6), 991
-998.
Taylor, D. Effectiveness of professional-peer group treatment: Symptom management for
women with PMS. Research in Nursing and Health. 1999, 22(6), 496-511.
Thys-Jacobs, S., McMahon, D., & Bilezikian, J. Differences in free estradiol and sex
honnone-binding globulin in women with and without premenstrual dysphoric
disorder. Journal of(~linical Endocrinology and Metabolism. 2008, 93(1), 96
102.
Thys-Jacobs, S., Starkey, P., Bernstein, D., & Tian, J. Calcium carbonate and the
premenstrual syndrome: Effects on premenstrual and menstrual symptoms.
American Journal ofObstetrics and Gynecology. 1998, 179, 444-452.
Webster, D., Lu, J., Chen, S., Farsworth, N., Wang, J. Activation of the opiate receptor
by Vitex agnus-castus methanol extracts: Implication for its use in PMS. Journal
ofEthnopharmacology. 2006, 106, 216-221.
Wysocki, S. (2008). Clinical challenges in women's health in the 21 st century: A practice
handbookfor nurse practitioners. Cranbury, NJ: NP Communications.
Yang, M., et ale Burden of premenstrual dysphoric disorder on health-related quality of
life. Journal of Women's Health. 2008, 17(1), 113-121.
Yonkers, K., et ale Efficacy of a new low-dose oral contraceptive with drospirenone in
premenstrual dysphoric disorder. Obstetrics & Gynecology. 2005, 106(3), 492
501.
PREMENSTRUAL DYSPHORIC DISORDER CONTROVERSY
16
APPENDIX A
Daily Symptom Report
2.1--" ~- _ ..._ ... _..
j.
~-
f-----. ... _.....
.
.....~ --
··-l·~
~
. __.~_. -l-..
I
4 I
1
5
i
I
I
Severity scoring for each symptom:
0= No symptom
1= Minimal or slightly apparent to you
2 = Moderate, awareness of symptom but does not affect your daily routine
3 = A lot, continuously bothered by the symptom and/or symptoms interferes with your
daily routine
4 = Severe, symptom is overwhelming and/or unable to carry out your daily routine
Freeman, E., DeRubeis, R., & Rickels, K. Reliability and validity of a daily diary for
premenstrual syndrome. Psychiatry Research. 1996, 65, 97.
17
PREMENSTRUAL DYSPHORIC DISORDER CONTROVERSY
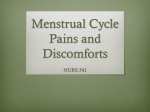
Appendix B
l\1ed'icClj)(~
wwwmedscapc com
OAllY RECORO OF SEVERITY OF PROBlEMS
Please print and use as many sheets as you need for at
least two FUll months of ratings.
Nome or ""'rob
MOOlh/Y'.XJr
r<xh '",eOl"g nore ,h'! cl.<>g'ee 10 whichyo'J e~j>(l.ie"ced each 01 'he prQiJ.!lm" lis.ed below P,,' on "x" in the box which cOHespo1\OS '0 the
~,,·,e·';ly:
I . not 0' 011, 2· ",iM;moL 3 . mild, A . nlodemre. 5 ·se,·ere, 6 . ex'.eme.
~~'n ra',
01
12
• 011 ·;'IYIr:·:! (t:1I~_L-.... 'j.-..rJ
.
... , .
_...
f~~t tit'~re,~.
wd, "dO"H1't
~o'!"!t '~0fH"}.,'.' {}oj
'.,:)f
-~hJC'~
f4!:.s WQ"hle':o$ rJ!
eJi'!'r
'2
~t:J {ltll"Ov'. ,~.,~-=- "~"f'le..d IJ$}- t~
"(tfr od~tJ~
Hod mood 1W>09' I' n 'c'drlcnly foo!
,ng lod or 'CGr~!) cr ....'(1~ ..~n';.:rl·.1} t()
,(rr-e-(t.~ 0'" i~,~
wl!.ff)
I~I~)' ~;Jn
<.
.s
Hoa lo~" IltltJ~ot:-~t
t..... IJfi.,
l{'~liX.I.
\I~UQ,) G(k"t~q..
In
to(fl.d ... I-."bb.(nt
'r,
7
rtt. ier7-.orfj C. !;rt-O
01 ~J'}~v-r'd C~
~jj'l:C."'Clftj"lCP:9i'
; i3
~
dd
CA
"J
1('Ic.f'-"iJ~d 0Ff.n.'lhfr ':1' "y.,.",Oh"
h,gQ c.!a .. :tI~l'i
\"X \pQ"C;,f1r,
~'~! ~..o(C, tool.: nap~, r.o:.md ,t n;;t.'d ~
g<! \lP ""her: ltl~ded.
~f!fllng
'10
l00d:
Fa
''0
*' !'-,o':
r(.Jbi
\.1.0'~p- ~ \toy,f'l9 {I~lc't;1
o"w~~i,".,{1
V' j~h ,,xII'"
ur
(.zn.'rc;
~(l~
In 4.0-;>
: t f'~:.Jd bteot' f~rrd"r,.It's.!. b''f:!>(Ht lwelr:r-rq_
oo~ \-tJf:jQ !'\, wti"'.ghr ;a~.
h4,.ndOot;I..,. IGo·n! C),
1r.\I.v:lt)
r.orr..
Of
l)('hi?' pbY~'('Ql \y/'tlp.!(I"I1 ~
A' ...... C'·
,~ht1oQi. ".om~
(11 1';:"\))1 o·~O',i!
r,UIJ~ '.~~<;
.utI
or.n. '30.1,/ rout, ~,
~ p'(~1('1Yi~ H{)~i
01 ptoo',Jd\"It'\ty
l.o4x·"v
Q{
1:-.<2HIC~n:::-
.A.! :C""..a~ .;I~tC'
u! ~he ,
L.nIJ~d GVQ:do ~'q
fobl~rnl n~e-d cl"C'.:e-
1"'1 or
J~\~ pi; "Ip:1ht'ITl
~" h.,.hh;.)~ ..,,- ',(l.;u.~~\ q(f)w,l.... '
At J~'H'
l")(,v
d shit f",-,bl(!;'1\.fo ""'~N ~i'O«"""1]
. i"'t<r -~(l'..J .....'ri'l rmoltOrnh1t:h ',., ,I~I .).J~;('f)-
~
-
.
,
-
Source J Pe-d at, Heall" Care @ 2000 Mosby, 1m;
Claman, F, & Miller, T., Premenstrual syndrome and premenstrual dysphoric disorder in
adolescence. Journal ofPediatric Health Care, 2006; 20(5): 329-333.