Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Molecular mimicry wikipedia , lookup
Immunocontraception wikipedia , lookup
Psychoneuroimmunology wikipedia , lookup
Cancer immunotherapy wikipedia , lookup
Innate immune system wikipedia , lookup
Polyclonal B cell response wikipedia , lookup
Drosophila melanogaster wikipedia , lookup
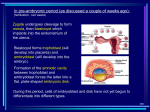
Harvard-MIT Division of Health Sciences and Technology HST.071: Human Reproductive Biology GESTATIONAL TROPHOBLASTIC DISEASE Complete Hydatidiform Mole Partial Hydatidiform Mole Partial Hydatidiform Mole Gestational Trophoblastic Disease Gestational Trophoblastic Disease PLACENTAL METABOLISM Proto-oncogenes tumor suppressor genes (p53) hormone receptors enzymes involved in steroid synthesis hypothalamic releasing hormones (ACTH related peptides) alpha interferon, other cytokines PLACENTAL METABOLISM Steroids synthesized by ovary also proteins in high concentration in human semen ovarian follicular fluid hCG can be found in very small amounts in normal tissue pituitary gland after menopause PLACENTAL METABOLISM 12 weeks on the trophoblast in contact with maternal circulation placental proteins in high levels in maternal blood steroid hormones in equal or higher levels in fetus prior to 12 weeks there is much extraplacental trophoblast (chorion) PLACENTAL METABOLISM Site of origin of many molecules unclear prior to 6 weeks hCG and hPL may be cytotrophoblast syncytiotrophoblast is source of most of the hormones produced (relaxin, inhibin, hCG) steroid and hCG secretion begins at 7 days post fertilization immunohistochemistry is inaccurate PLACENTAL METABOLISM Trophoblast is a syncytium (multiple nuclei) Invasive cells are the cytotrophoblast unlike tumors which also secrete proteins Trophoblast is a transfer tissue analogous to gut, kidney, lung no secretions by above organs however above exchange to out side of body (not 2 circulations) PLACENTAL METABOLISM Trophoblast is a male organ maternal genome is required for development of the fetus paternal pronucleus associated with trophoblast paternal haploid set may be imprinted on the trophoblast and determine which genes become active only other major site of placental protein synthesis is male reproductive tract differential methylation by trophoblast PLACENTAL SIGNALING TGF-beta and IGF2 hCG PAF (or EDPAF) [endothelial derived platelet activating factor] embryonic proteases estrogen and progesterone interferon embryo derived histamine releasing substances plasma protein C prostaglandins embryo derived beta-inhibin PROGESTERONE Increases blood volume stimulates endometrial secretion acts as immunosuppressant stimulates protein synthesis inhibits phospholipase C affects estrogen receptor distribution activates pinopod formation promotes fibronectin synthesis stimulates decidual cells IMPLANTATION After ovulation glands become tortuous spiral arteries form endometrium thickens pinopods, microvilli, apical protrusions present at 20-23 days implantation occurs during this time pinopods absorb molecules and fluid from lumen increase apposition of embryo and endometrium reduce potential cavity IMMUNOLOGY OF PLACENTA Hemochorial placenta in contact with maternal immune system transplanted embryo alone vs trophoblast only components of MHC selectively absent from T Ab to beta2 and HLA-A2 stained cells within the villi but not surface layers of T no class II on T but present on stromal cells HLA molecules unique (Ellison 1986) - HLA-G resistance to NK cells T does not express A and B but does express Rh(D) IMPLANTATION Ovum captured in distal portion of tube fertilization occurs enters uterus 4 days after ovulation cleavage occurs during these 4 days but no change in size (no cell growth) - 150um inner cell mass --> embryo trophoblast ---> placenta cell growth then begins IMPLANTATION Implantation occurs 7-8 days after ovulation Embryo “targets” hypo epithelial vessels on surface of endometrium surface is made receptive for the embryo immediate human delayed facultative (rat, red kangaroo only during stress) facultative (Alaska fur seal, mink, bear always) free floating morula/blastocyst with min. met. act. Light cycle control duration of delay IMPLANTATION Invasion between uterine epithelium (intrusive penetration) ferret, guinea pig, rhesus monkey replace epithelial cells (displacement penetration) mouse, rat fuse with epithelial cells (fusion penetration ) rabbits Human mode unknown but probably intrusive attaches to epithelium and heads for decidua cytotrophoblasts fuse to form syncytium penetration continues for 4 days stroma undergoes changes (not just displaced) COMPARATIVE PLACENTATION ATTACHMENT INTERFACE - describe the placenta CHORIONIC PLATE (fetal unit) capillary endothelium mesodermal connective tissue trophoblast epithelium EPITHELIOCHORIAL preserves maternal epithelium/endothelium ENDOTHELIOCHORIAL only maternal endothelium preserved HEMOCHORIAL maternal blood comes into contact with trophoblast classified by the number of layers of trophoblast between maternal blood and fetal endothelium humans are hemomonochorial IMMUNOLOGY Human trophoblast DOES NOT EXPRESS classical Class I MHC antigens HLA-A, B, and C highly polymorphic cell surface Non-Classical Class I genes HLA-E, F, and G HLA-G expressed first trimester extravillous cytotrophoblast term chorioamnion first trimester villous mesenchyme Villous trophoblast has more variable expression of these genes TROPHOBLAST RESISTANCE HLA-G may restrict antigen presentation Trophoblast resistance to: Antibody cytotoxic T cells natural killer cells (NK) macrophages decidua-associated large granular lymphocytes (LGL) lack of “target” for NK and LGL Trophoblast secretion of immune regulators interferons (IFN’s) cytokines (IL-10) IFN activity seen in all species IMMUNE MODULATORS Enhanced class 1 (IFN-α and IFN-β) villous syncytiotrophoblast and extravillous trophoblast suppress immune effector cell proliferation and function ? Expression of cell surface antigen of trophoblast Decreased class II (IFN-gamma) pro-inflammatory Enhanced IL-10 decreased IFN-γ decreased TNF-α decreased IL-2 Bias maternal immune system at interface away from cell mediated immunity HUMAN DECIDUAL FACTORS Colony stimulating factors (CSF-1, GM-CSF, IL-3) increase trophoblast growth Epidermal growth factors (EGF, TGF-α) increase hCG secretion choriocarcinoma normal cell lines Transforming growth factor-β inhibit or stimulate depending on target cell low expression during proliferative phase increased during secretory phase greater increase during early pregnancy ADHESION MOLECULES Integrins cell to cell adhesion receptors cell-to-cell matrix reactions 21 different types anchor cells to specific locations transmit information to cells immunologic homing metastatic spread healing embryologic development heterodimers composed of α and β subunits ligand specificity a function of αβ heterodimer may bind to several ligands ligand may bind to several heterodimers ADHESION MOLECULES Integrins expression constitutively expressed phasic and hormonally regulated infertility ? Related to reduced endometrial expression of β3 defect in embryonic expression of β1 causes involution of inner cell mass but preserves trophoblast polarity distribution of the integrins either promotes or retards attachment switching early trophoblast exhibits α5β1 but later changes to α1β1 may regulate invasiveness COMPLETE MOLE Rare in western nation (1:1000-1500) Much more common in Asia High incidence in Hawaiians independent of birthplace Unrelated to paternal age or race Recurrence is rare but incidence rises steeply after repeats Maternal age a fact (<20 and >40) COMPLETE MOLE clinical findings Vaginal Bleeding Molar vesicles Excess uterine enlargement beyond dates Excess hCG with nausea, emesis, pre-eclampsia Thyroid storm Embolization of placental elements RECURRENT TROPHOBLASTIC DISEASE Trophoblastic invasion beyond the placental site Does not convert to malignancy Spontaneous resolution possible Malignant transformation (choriocarcinoma) Metastases, elevated hCG In uterus or lungs, kidneys, other sites Placental site tumor COMPLETE MOLE Gross genomic abnormality Early loss of embryo Metamorphosis of placenta Early development must be near normal Must achieve morula, blastula, implantation Usual start with first generation villi during week 5 (LMP) Trophoblast hyperplasia overwhelms orderly development of trophoblast bilayer COMPLETE MOLE Stubby polygonal structures Cauliflower appearance More cellular stroma More mucoid material and edema Absent or scant villous capillaries Capillaries devoid of blood (like in early fetal demise) Edema leads to cistern formation COMPLETE MOLE Large grape-like villus with avascular wall made of cell poor connective tissue Inner edge takes on appearance of synovium rather than epithelium Seen only in CHM and PHM not in trisomies Molar fluid contain trophoblastic hormones and procoagulant substances Antigenically same as in a pregnancy Maternal HL-A antibodies engendered by villous mesenchyme (fetal) as in normal pregnancy Complete Hydatidiform Mole Villous hydrops Trophoblast hyperplasia Cistern formation Blood vessels lacking Mounds of mitotic cytotrophoblast Lacy proliferation of syncytiotrophoblast Extravillous trophoblast Cytologic atypia Diploid Nuclear DNA androgenically derived Partial Hydatidiform Mole Focal trophoblast hyperplasia Mounds of syncytiotrophoblast Nuclear atypia infrequent Villi vessels contain nucleated RBS and often fetal tissue found Triploid Extra haploid DNA is paternal PARTIAL MOLE Incidence of invasion is low < 5% and perhaps much smaller Live fetus with triploidy has high RTD rate Anomalous high hCG Visualized by MRI and U/S No embolic phenomenon as a rule Some pulmonary metastases have been seen on MRI Respond to chemotherapy Choriocarcinoma not related to PHM COMPLETE MOLE embryo Embryo dies early (4-6 weeks MA) C-R length < 5.5 mm Embryonic disk survives till day 14 Provides the extraembryonic mesenchyme that makes the placenta Occasionally we see later survival of a fetus but this is rare Fetal nucleated red cells noted in the mole PARTIAL MOLE Incidence 1-2% in humans – Triploidy Majority of triploids are diandric Theoretical 50% of early abortuses are chromosomally abnormal 15% are triploid 80% diandric This would yield 6.6% of PHM in abortuses Not found in actual practice Poor technique for examination PARTIAL MOLE No association Age Race Geography Bland condition free of sequelae Common features Trophoblastic hyperplasia Villous swelling PARTIAL MOLE Common features with CHM Early embryonic death Undue uterine enlargement High hCG levels Hyperemesis Pre-eclampsia Residual disease Thyrotoxicosis PARTIAL MOLE embryology Early stages develop along normal lines Pathologic modifications occur (week 5 LMP) Placental features seen later Fetus dies later Rarely seen before 6-7 weeks PARTIAL MOLE embryology Trophoblastic hyperplasia confined to syncytiotrophoblast Villous fluid accumulation and cisterns form later Morphologic “checkerboard” pattern of normal and abnormal villi Trophoblastic inclusions Sharp angle scalloping of villous outlines Fetal demise at 8-9 weeks Larger fetuses show congenital anomalies COMPLETE MOLE genetics Compound error of fertilization Empty egg Possible extrusion of both haploid sets in the first or second polar body Fertilized by a haploid sperm This doubles to give 46 chromosomes Needs to be a 23X sperm lest we get a 46YY non-viable cell Diploid sperm ? Polyspermic fertilizationheterozygote 20-25% of CHM COMPLETE MOLE genetics Homozygosity Lethal genes Early clinically occult destruction of zygotes Early demise of embryo proper Absence of maternal chromosomes Presence of purely paternal ones Murine egg experiment Male and female pronucleusnormal Female - female pronucleuslong survival embryo Male – male pronucleusexuberant trophoblast PATERNAL MOLE genetics two sperm penetrate egg Triploid zygote (69 chromosomes) Possible diploid sperm fertilization Meiosis error in spermatogenesis XXX:XXY:XYY should be 1:2:1 XYY do not survive therefore above ratio not found CHM is PATERNAL DOMINANCE PHM has MATERNAL CONTRIBUTION