Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Monoclonal antibody wikipedia , lookup
Adaptive immune system wikipedia , lookup
Lymphopoiesis wikipedia , lookup
Innate immune system wikipedia , lookup
Cancer immunotherapy wikipedia , lookup
Molecular mimicry wikipedia , lookup
Immunosuppressive drug wikipedia , lookup
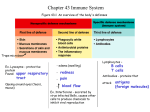
FLOW CYTOMETRY An immunofluorescent method that mutually complements the fluorescent microscopy Detection and analysis of different cells or particles travelling at high velocity in flow Detects fluorescence intensity and scattered light of the labeled cells Can investigate enormous number of cells in a short period of time ADVANTAGES OF FLOW CYTOMETRY Most cells in the immune system can be found in free or loosely adherent form. They can be easily suspensed and labeled by fluorescent antigen specific antibodies, and then they can be examined cell by cell The cells’ light scatter and immunofluorescent properties can be analyzed statistically (e.g. percentages of different cell populations) Rare cell populations can be identified and examined (e.g. antigen specific lymphocytes) The method provide qualitative and quantitative data – it can detect the presence of different antigens in the cell, and the expression levels of these antigens. Changes in the expression of certain molecules can be followed after different treatment of the specimen. (e.g. cell activation, disease progression) Benchtop flow cytometer Sorter - flow cytometer (FACS station) LIGHT SCATTER AND FLUORESCENCE Forward angle light scatter sensor (FSC, FALS) Laser Can be loosely considered as a representation of the particle size Side light scatter (SSC) and fluorescence detectors SSC represents the granularity of the cells Multicolor staining can be used to identify cell sub-populations (autofluorescence – presence of piridins and flavins) IMMUNOPHENOTYPING BY FACS Example: Measurement of CD4+ (helper) and CD8+ (cytotoxic) T cell ratio (e.g. monitoring AIDS progression) Labeling: Th FITC labeled anti-CD4 antibody(α-CD4-FITC) PE labeled anti-CD8 antibody (α-CD8-PE) NK Tc Lymphocytes in the peripheral blood sample Fluorescent microscopy B high velocity flow stream detecting CD4-FITC labeled (TH) cell (in cuvette or stream in air) signal processing unit CD8 PE detector screen increasing light intensity a dot representing a CD4+ CD8- cell CD4 FITC microscopy: detecting the PE labeled cell (CD8-PE) CD8 PE detector signal processing unit increasing light intensity CD4 FITC detecting the unlabeled cell (e.g. B cell) by autofluorescence CD8 PE detector Signal processing unit increasing light intensity microscopy: dim (autofluorescent) cell CD4 FITC CD8 PE 18% 44% 0% quadrant statistics CD4 38% FITC GRAPHICAL REPRESENTATIONS 1. dot-plot contourplot densityplot GRAPHICAL REPRESENTATIONS 2. Histogramm Numeral intensity values: ~7 ~ 1300 homogenous cell population is normally distributed (Gaussian) Different cell types - characteristic light scattering granulocytes side light scattering (SSC) (e.g. granulated) monocytes lymphocytes forward light scattering (FSC) („size”) EXAMINATION OF PERIPHERAL BLOOD BY HAEMATOLOGY AUTOMATS Measured parameters: peroxydase staining (the presence of myeloperoxydase, x – axis) light scatter (high on large granular cells, y – axis) 1 (Noise) 2 Nucleated Red Blood Cells 3 Platelet Clumps 4 Lymphocytes and Basophils 5 Large Unstained Cells (LUC) 6 Monocytes 7 Neutrophils 8 Eosinophils Only the major cell types can be identified CHARACTERIZATION OF IMMUNE CELLS USING CELL SURFACE MARKERS Cell types, differentiation stages can be identified using a combination of cell surface markers. Used in diagnostics: - ratio of different cell types - altered expression of cell surface markers Examples: - Inflammatory processes – increased neutrophil numbers - HIV progression – decrease of CD4+ T cell count CD4+ : CD8+ = 1.6 Normal CD4+ T cell count = 600 – 1400/l AIDS = CD4+ T cell count <200/l - increase of CD5+ B cells – typical for some B cell leukemias CD antigen cell type function ligand CD3 T cells TCR signaling - CD4 helper T cells, (monocytes, pDC) T cell co-receptor, (HIV receptor) MHC- II, HIV CD5 T cells, (B cell subset: B1) adhesion, activation signals CD72 CD8 cytotoxic T cells, (NK, T cells) T cell co-receptor MHC I CD14 monocytes, macrophages, some granulocytes LPS binding LPS, LBP CD19 B cells part of CR2, B cell coreceptor C3d, C3b CD28 T cells co-stimulatory signals to T cells (B7-1, B7-2) CD80, CD86 CD34 hematopoietic progenitor cell adhesion CD62L (L-selectin) CD56 NK cell, (T and B cell subset) homoadhesion (N-CAM isoform) APC: DC, B, monocyte, macrophage co-stimulatory signals CD80, CD86 (B7-1, -2) CD28, CD152 Investigation of the presence or absence of Bruton’s tyrosine kinase (BTK) by flow cytometry Futatani T et al. Blood 1998;91:595-602 Detection of intracellular cytokines by flow cytometry cytokine specific antibody with fluorescent labelling - the cell membrane should be permeabilized (detergent) - the cells should be fixed previously avoiding the decomposition of the cells (e.g. aldehyde fixation) - optionally the cells could be labelled first with a cell type specific antibody (e.g. CD4) cytokines The result: You can determine which cell type has produced the cytokines! Sensitive, relatively easy method, rare cell populations can be readily studied. Multiple colours are available for detection of more cytokines or cell surface markers The cell cycle can be examined by a fluorescent dye G2 G0 M that intercalates stoechiometrically into double stranded DNA (e.g. propidium iodide, PI) DNA analysis G1 G0 G1 s cell number G2 M s 0 200 400 600 800 1000 4N 2N DNA content Distribution of a normal cycling cell-population by DNA content (flow cytometry) Methods for determinating the B/T cell proliferation 3H-labeled thymidine incorporation – measures the increasing DNA content by β decomposition, and does not answer the numbers of cell division, and the dividing cell number thymidine-analog bromodeoxyuridin (BrdU) can be administered to experimental animals, or cell cultures, and the proliferating cells can be detected by labelling with BrdU specific antibody (microscopy, FACS) Carboxyfluorescein diacetate succinimidyl ester (CFSE) fluorescent stain can be used to tracking the cell divisions by flow cytometry: Tracking the cell divisions „Cell tracer” dye enter the cell, and trapped there. The apolar CFSE can bind covalently to the cellular proteins. Later the stain can only be diluted by the cell divisions: distributed equally between the two daughter cells – the fluorescence intensity decreases to the half also. cell divisions: 8 7 6 5 4 3 2 1 0 T cell antigen specificity Identifying the antigen specific T cells The efficiency of an immunization can be evaluated by the increase of the antigen specific cell number antigen specific T cell T cell clones with the same T cell receptor immunization If you can identify the specificity of the T cell receptors then you can monitor the increase of the antigen specific T cells’ number Labelled MHC-peptide complex can be used to identify the matching (specific) T cell receptor ..but the MHC binds the TCR with low affinity MHC T cell receptors T cell The interaction between one MHC molecule and one TCR is not strong enough for labelling The multimerized MHC-peptide complex can have enough avidity MHC multimer technics One part of the pentamer peptide MHC molecule self assembling coiled-coil-domain fluorescent label The pentamer Binding of the MHC pentamer to the T-cell MHC pentamer The MHC-peptide oligomer can bind the specific T-cell receptors with high avidity The number of the antigen-specific T cells can be evaluated by MHC multimers. So the efficiency of an immunization or a therapy can be estimated. T cell receptors peptide specific T cell Click here to watch the animation EBV BZLF-1 (RAKFKQLL/ HLA-B*0801) specific T cells (90-95% of the human population are carrier) Tetramer (pentamer) tests The number of microbe specific T cells can be increased in the body because of the persistent (e.g. herpesviruses) or repeated infections CMV specific T cells in healthy HLA-A2 donor Influenza epitope (GILGFVFTL/ HLA-A0201) specific T cells in a healthy donor allele sequence Tumour (associated) epitope A*0201 GVLVGVALI Carcinogenic Embryonic Antigen (CEA) 694-702 A*0201 LLGRNSFEV p53 261-269 A*0201 LLLLTVLTV MUC-1 12-20 MHC-peptid pentamers for detecting antigen specific T cells A*0201 RLLQETELV HER-2/neu 689-697 A*0201 RMFPNAPYL Wilm's Tumour (WT1) 126-134 A*0201 SLLMWITQV NY-ESO-1 157-165 A*0201 STAPPVHNV MUC-1 950-958 allele sequence A*0201 VISNDVCAQV Prostate Specific Antigen-1 (PSA-1) 154-163 A*0201 CLGGLLTMV EBV LMP-2 426-434 A*0201 VLQELNVTV Leukocyte Proteinase-3 (Wegener's autoantigen) 169-177 A*0201 GLCTLVAML EBV BMLF-1 259-267 A*0201 VLYRYGSFSV gp100 (pmel17) 476-485 A*1101 IVTDFSVIK EBV EBNA-4 416-424 A*0201 YLEPGPVTA gp100 (pmel17) 280-288 A*2402 TYGPVFMCL EBV LMP-2 419-427 A*0201 YLSGANLNL Carcinogenic Embryonic Antigen (CEA) 571-579 B*0702 RPPIFIRRL EBV EBNA-3A 247-255 A*0201 KVLEYVIKV MAGEA1 278-286 B*0801 FLRGRAYGL EBV EBNA-3A 193-201 A*0201 KVAELVHFL MAGEA3 112-120 B*0801 RAKFKQLL EBV BZLF-1 190-197 A*0201 KTWGQYWQV gp100 (pmel17) 154-162 B*3501 HPVGEADYFEY EBV EBNA-1 407-417 A*0201 HLSTAFARV G250 (renal cell carcinoma) 217-225 A*0201 ILAKFLHWL Telomerase 540-548 allele sequence Influenza A epitope A*0201 ILHNGAYSL HER-2/neu 435-443 A*0101 CTELKLSDY Influenza A (PR8) NP 44-52 A*0201 IMDQVPFSV gp100 (pmel17) 209-217 A*0201 GILGFVFTL Influenza A MP 58-66 A*0201 KIFGSLAFL HER-2/neu 348-356 A*0301 ILRGSVAHK Influenza A (PR8) NP 265-274 A*0201 LMLGEFLKL Survivin 96-104 A*0201 ALQPGTALL Prostate Stem Cell Antigen (PSCA) 14-22 allele sequence A*0201 CMTWNQMNL Wilm's Tumour (WT1) 235-243 A*0201 ILKEPVHGV HIV-1 RT 476-484 A*0201 ELAGIGILTV MelanA / MART 26-35 A*0201 KLTPLCVTL HIV-1 env gp120 90-98 A*0201 FLTPKKLQCV Prostate Specific Antigen-1 (PSA-1) 141-150 A*0201 SLYNTVATL HIV-1 gag p17 76-84 A*0201 GLYDGMEHL MAGEA-10 254-262 A*0201 TLNAWVKVV HIV-1 gag p24 19-27 A*0301 KQSSKALQR bcr-abl 210 kD fusion protein 21-29 A*0301 QVPLRPMTYK HIV-1 nef 73-82 A*0301 ATGFKQSSK bcr-abl 210 kD fusion protein 259-269 A*0301 RLRPGGKKK HIV-1 gag p17 19-27 A*0301 ALLAVGATK gp100 (pmel17) 17-25 A*2402 RYLKDQQLL HIV-1 gag gp41 67-75 A*2402 VYGFVRACL Telomerase reverse transcriptase (hTRT) 461-469 B*0702 IPRRIRQGL HIV-1 env gp120 848-856 A*2402 TYLPTNASL HER-2/neu 63-71 B*0702 TPGPGVRYPL HIV-1 nef 128-137 A*2402 TYACFVSNL Carcinogenic Embryonic Antigen (CEA) 652-660 B*0801 FLKEKGGL HIV-1 nef 90-97 A*2402 TFPDLESEF MAGEA3 97-105 B*0801 GEIYKRWII HIV-1 gag p24 261-269 A*2402 EYLQLVFGI MAGEA2 156-164 B*2705 KRWIILGLNK HIV-1 gag p24 265-274 A*2402 CMTWNQMNL Wilm's Tumour (WT1) 235-243 H-2Kd AMQMLKETI HIV-1 gag p24 199-207 A*2402 AFLPWHRLF Tyrosinase 188-196 B*0801 GFKQSSKAL bcr-abl 210 kD fusion protein 19-27 EBV epitope HIV epitope Case study (from the ’90ies) Helen Burns was the second child born to her parents. She thrived until 6 months of age when she developed pneumonia in both lungs, accompanied by a severe cough and fever. Blood and sputum cultures for bacteria were negative but a tracheal aspirate revealed the presence of abundant Pneumocystis jirovecii. She was treated successfully with the anti-Pneumocystis drug pentamidine and seemed to recover fully. As her pneumonia was caused by the opportunistic pathogen Pneumocystis jirovecii, Helen was suspected to have severe combined immunodeficiency. What kind of laboratory test should be performed to confirm or rule out the diagnosis of severe combined immunodeficiency? A blood sample was taken and her peripheral blood mononuclear cells were stimulated with phytohemagglutinin (PHA) to test for T cells function by 3H-thymidine incorporation into DNA. A normal T-cell proliferative response was obtained, with her T cells incorporating 114,050 counts/min of 3H-thymidine (normal control 75,000 counts/min). Helen had received routine immunizations with orally administrated polio vaccine and DPT (diphtheria, pertussis, and tetanus) vaccine when she was 2 months old. However, in further tests, her T cells failed to respond to tetanus toxoid in vitro, although they responded normally in the 3H-thymidine incorporation assay when stimulated with allogeneic B cells (6730 counts/min incorporated compared with 783 counts/min for unstimulated cells). When it was found that Helen's T cells could not respond to a specific antigenic stimulus, her serum immunoglobulins were measured and found to be very low. IgG levels: IgA levels: IgM levels: 96 mg/dl (normal: 600-1400 g/dl) 6 mg/dl (normal: 60-380 mg/dl) 30 mg/dl (normal: 40-345 mg/dl) Helen's white blood cell count was elevated at 20,000 cells/μl (normal range 4000-7000/μl). Of these, 82% were neutrophils (normal range: 10-33%), 10% lymphocytes (n.r: 20-40%), 6% monocytes (n.r: 2-10%), and 2% eosinophils (n.r: 1-6%). The calculated number of 2000 lymphocytes/μl is low for her age (normal >3000 μl-1). Of her lymphocytes, 7% were B cells (CD20+) (normal 10-12%) 57% reacted with antibody to the T cell marker CD3. At 388 cells/μl her number of CD8+ T cells was lower than the normal range (5001700/μl), and the number of CD4+ T cells (288/μl) was much lower than the normal (her CD4+ T-cell count would be expected to be twice her CD8+ T-cell count: 1400-4300). The presence of substantial numbers of T cells, and thus a normal response to PHA, ruled out a diagnosis of sever combined immunodeficiency. Helen's paediatrician referred her to the Children's Hospital for consideration for a bone marrow transplant, despite the lack of diagnosis. When an attempt was made to HLA type Helen, her parents and her healthy 4-year-old brother, a DR type count not be obtained from Helen's white blood cells. A long-term culture of her B cells was made by transforming them with Epstein-Barr virus and the transformed B cells were then examined for expression of MHC class I and class II molecules with fluorescent-tagged antibodies. It was found that her B cells did not express HLA-DQ or HLA-DR molecules and a diagnosis of MHC class II deficiency was established. Detection of MHC class II molecules by fluorescent antibody. Helen’s transformed B-cell line was examined by using a fluorescent antibody to HLA-DQ and –DR. Helen (left panels) expressed approximately 1℅ of the amount of MHC class II molecules compared with a transformed B-cell line from a normal control (right panels). Cells from a patient with class II histocompatibility deficiency Immunofluorescence of normal EBV-transformed cells Transformed B cells Transformed B cells Transformed B cells Transformed B cells As her brother did not have the same HLA type as Helen, it was decided to use her mother as a bone marrow donor. The maternal bone marrow was depleted of T cells to diminish the chance of graft-versus-host disease developing and was administered to Helen by transfusion. The graft was successful and immune function was restored. Discussion and questions 1. Why did Helen lack CD4 T cells in her blood? The maturation of CD4 T cells in the thymus depends on the interaction of thymocytes with MHC class II molecules on thymic epithelial cells. When the MHC class II genes are deleted genetically in mice, the mice also exhibit a deficiency of CD4 T lymphocytes. 2. Why did Helen have low level of immunoglobulins in her blood? The polyclonal expansion of B lymphocytes and their maturation to immunoglobulin-secreting plasma cells require cytokines from CD4 T helper cells, such as IL-4. Helen’s hypogammaglobulinemia is thus a consequence of her deficiency of CD4 T lymphocytes. 3. In SCID , lymphocytes fail to respond to mitogenic stimuli. Although Helen was first thought to have SCID, this diagnosis was eliminated by her normal response to PHA and an allogenic stimulus. How do you explain these findings? Helens’ T cells, although decreased in number, are normal and are not affected by the defect. They are capable of normal responses to nonspecific mitogens and to an allogenic stimulus in which the antigen is presented by the MHC molecules on the surface of the (nondefective) allogeneic cells and thus does not require to be processed and presented by the defective cells. However, the failure of her lymphocytes to respond to tetanus toxin in vitro resulted from the fact that, in this situation, there were no cells that could present antigen on MHC class II molecules to the CD4 T cells. 4. If a skin graft were to be placed on Helen’s forearm do you think she would reject the graft? Yes. Helen’s T cells would be capable of recognizing the foreign MHC molecules on the grafted skin cells and would reject the graft.