Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
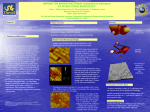
Medical Technology SA Volume 26 No. 1 | June 2012 Peer reviewed ORIGINAL ARTICLE COLLAGEN IN ODONTOGENIC TUMOURS: A HISTOCHEMICAL- AND IMMUNOHISTOCHEMICAL STUDY OF 19 CASES J Hangelbroek (NHD Med Tech), EJ Raubenheimer (MChD, PhD, DSc), R Vorster (NHD Med Tech), SP Ngwenya (MDent) Unit 2: Pathology, School of Oral Health Sciences, Medunsa Campus, University of Limpopo, South Africa Correspondence to: EJ Raubenheimer | tel: +27 12 521 4838 | fax: +27 12 521 4274 | email: [email protected] Abstract This study investigated the collagen content of odontogenic tumours. Wax blocks of 19 odontogenic tumours (ameloblastoma n=3, adenomatoid odontogenic tumour n=3, ameloblastic fibroma n=3, ameloblastic fibro-odontoma and ameloblastic fibro-dentinoma n=4, odontogenic myxoma n=3 and odontogenic fibroma n=3) were sectioned and stained by the H&E-, Picrosirius-, Reticulin-, Masson Trichrome methods and the immunoperoxidase technique for collagen type IV. The distribution of collagen types I-IV was recorded for each tumour. The basement membrane zones of ameloblastomas showed perpendicular oriented collagen type I fibres which anastomosed with the stromal collagen. The collagen content correlated with the shapes of the epithelial components in ameloblastomas, adenomatoid odontogenic tumours, ameloblastic fibromas and odontogenic fibromas. Formation of collagen was found to be the first indication of stromal induction. In odontogenic myxomas, coarse type I collagen fibres were intersected at obtuse angles by delicate type III fibres. Except for around blood vessels, no collagen type IV was found in odontogenic tumours. The distribution of collagen is unique for each odontogenic tumour type. Keywords Collagen, odontogenic tumours, histochemistry, immunohistochemistry INTRODUCTION Odontogenic tumours arise from the epithelium- and/or ectomesenchyme from which teeth and their supporting structures originate. The epithelial component gives rise to dental enamel and the ectomesenchyme to the remainder of the tooth, periodontal ligament and alveolar bone. During embryogenesis complex interactions between these tissues result in the orderly formation of a tooth and its supporting structures. Pathological proliferations with varying levels of induction between the remnants of these primordial tissues may lead to the development of complex tumours which differ in microscopic appearance and biological behaviour. The World Health Organization (WHO) classification, which has recently been refined, categorizes odontogenic tumours into those of odontogenic epithelial origin, odontogenic ectomesenchymal origin and a third group comprised of a mixture of odontogenic epithelium and odontogenic ectomesenchyme [1]. In several odontogenic tumours the deposition of basement membrane material, dental hard tissue (enamel, dentin and cementum), bone and fibrous connective tissue occur and an accurate diagnosis depends on identification of these tissue types. The organic component of most of the mineralized odontogenic tissues is collagen. In pathological proliferations, microscopic distinction between cementum, bone and dentin may be difficult and distinction often depends on the associations- and spatial arrangement of these mineralized deposits. Collagen is the most important structural component of human connective tissue. At least 10 distinct collagen types have been described [2]. Collagen types I, II and III consists of a helix of 3 coiled polypeptide chains and represent the most important structural collagens. Collagen type I is typically found in the 28 www.smltsa.org.za | ISSN 1011 5528 dermis of the skin and type II in bone and cartilage where their most important function is to provide strength to the tissue. Collagen type III is found in reticulin fibres around blood vessels and the viscera where their flexibility allows movement, expansion and contraction [2]. Collagen types I-III are deposited by fibroblasts and other cells of mesenchymal origin. Collagen type IV is synthesized by cells of epithelial- or endothelial origin, often as a component of basement membranes. Their reticular distribution facilitates a supportive function [3]. Studies on collagen distribution and typing in odontogenic tumours are infrequent in the literature. The purpose of this study was to record the distribution of collagen in odontogenic tumours of epithelial-, ectomesenchymal- and mixed epithelial and ectomesenchymal origin (keratocystic odontogenic tumours were excluded from this study). MATERIALS AND METHODS Wax blocks of 19 cases representative of the epithelial-, ectomesenchymal- and mixed epithelial ectomesenchymal categories of odontogenic tumours were retrieved from the archives of our laboratory (Table 1). Although odontogenic keratocysts are classified as keratocystic odontogenic tumours in the recent WHO classification [1], we did not include examples in this study. Five- 3 micron sections were prepared and stained with haematoxilin and eosin, Picrosirius-4, Gomori’s reticulin- and the Masson Trichrome techniques and the Pasqual modification of the immunoperoxidase technique for Collagen Type IV (Dako monoclonal anti-human collagen IV M0785). All sections were viewed by conventional light microscopy and the Picrosirius stained sections by employing high intensity polarized light. The distribution of the collagen types was recorded. Areas of inflammation were not analyzed. Collagen type I is reported Medical Technology SA Volume 26 No. 1 | June 2012 to appear yellow and red with strong birefringence, collagen type II red with weak birefringence and collagen type III, green with weak birefringence in sections stained by the Picrosirius technique and examined by high intensity polarized light [4]. Table 1: Tumour type and numbers examined. TUMOUR TYPE NO. OF CASES Odontogenic Tumours of Epithelial Origin Ameloblastoma 3 Adenomatoid odontogenic tumour 3 Mixed Odontogenic Tumours Ameloblastic fibroma 3 Ameloblastic fibro odontoma 2 Ameloblastic fibro dentinoma 2 Odontogenic tumours of Ectomesenchymal Origin Odontogenic myxoma 3 Odontogenic fibroma 3 Reticulin stains are reported to be indiscriminately positive for collagen types I, II and III [5]. RESULTS In all odontogenic tumours the capsule consisted of Type I collagen. No collagen Type IV was found as a product of any tumour in the study, except for positive staining of the basement membranes of blood vessels within and around the tumours. As expected, collagen deposits in the ectomesenchymal- and mixed categories of odontogenic tumours were more extensive than in those of epithelial origin. In ameloblastomas, argyrophilic collagen type I fibres radiated from the basal area of the ameloblasts perpendicular through the epithelial basement membrane zone into the surrounding coarse stromal collagen. Delicate type III fibres were present between the type I fibres (Figures 1A and 1B). Areas of plexiform change in ameloblastomas showed dense collagen type I fibres between and linear to the plexiform strands of ameloblastic epithelium. The shape of the plexiform strands generally correlated with the direction and volume of the collagen bundles in the connective tissue stroma. At the periphery of the solid epithelial nodules in adenomatoid odontogenic tumours, foci showing accumulations of delicate wavy collagen fibres correlated with basement membrane- like deposits surrounding the anastomosing chords of epithelium seen in reticulin stained sections (Figure 2). Calcifications had a tendency of occurring in areas where these delicate fibres were found. The central spaces of the rosette- and duct like structures in the solid epithelial nodules contained varying densities of entangled collagen type I fibres. Figure 1A: Collagen distribution in the basement membrane zone of ameloblastomas. Collagen type I fibres pass perpendicular through the basement membrane zone (arrows). Note the delicate type III fibres between the type I fibres (Picrosirius stain viewed with high intensity polarized light, magnification X400). In the ameloblastic fibromas, irregularly distributed volumes of collagen were present around the epithelial follicles. In the zones characterized by dense woven collagen, thick fibres radiated into the ectomesenchymal stroma and anastomosed with a more delicate fibre network around individual plump mesenchymal cells. Further away from the epithelial follicle, fibres associated with less plump mesenchymal cells, followed a course parallel to the layer of ameloblasts of the follicle (Figure 3A). The density of the fibres around the epithelial follicles was generally found to impact on the direction of enlargement- and shape of the epithelial follicle (Figure 3B). Figure 1B: Delicate argyrophylic fibres passing from the basal region of the ameloblastic epithelium (A) through the basement membrane zone (arrows) into the connective tissue (C) (Reticulin stain, magnification X400). Figure 2: Adenomatoid odontogenic tumour. Flattened epithelial chords surrounded by abundant delicate fibres in the peripheral zones of the tumour (arrows) (Reticulin stain, magnification X40). ISSN 1011 5528 | www.smltsa.org.za 29 Medical Technology SA Volume 26 No. 1 | June 2012 Figure 3A: Ameloblastic fibroma. Note the epithelial follicle (E), dense array of delicate fibres in the basement membrane zone (arrow), radiating coarse fibers merging with the fibre network around plump ectomesenchymal cells and parallel arrays of fibres in the peripheral connective tissue (CT) (Reticulin stain, X200). Figure 3B: Epithelial follicle surrounded eccentrically by dense radiating collagen Type I fibres that restrict expansion in the associated part of the follicle (black arrows). The white arrows indicate the direction of expansion of the follicle towards a zone unrestricted by collagen (Picrosirius stain viewed with high intensity polarized light, magnification X400). Figure 4A: Ameloblastic fibro-odontoma. Homogenization of collagen adjacent to the epithelial follicle (ameloblast indicated by black arrow) with ectomesenchymal cells incorporated in lacunae (bold white arrows). Note the linear arrangement of plump ectomesenchymal cells on the surface of the deposit (delicate white arrows) (Reticulin stain, X200). Figure 4B: Epithelial basement membrane zone (between the white arrows), mature dentin with a globular appearance (asterisk) and more recent deposited dentin (black arrow). Note the odontoblastic tubules in the latter (Masson trichrome stain, tissue decalcified, X200). Figure 5: Odontogenic fibroma. Note the collagen bundles running parallel with the orientation of the dormant epithelial rests (Masson Trichrome stain, magnification X 200). 30 www.smltsa.org.za | ISSN 1011 5528 The biopsy samples of the mixed epithelial and ectomesenchymal category with induction of dental hard tissue formation (ameloblastic fibro-odontoma and ameloblastic fibro-dentinoma) were decalcified due to their mineralized content. The earliest sign of induction of mineralized tissue was demonstrable by employing the reticulin staining method which showed homogenization of fibres which enveloped plump ectomesenchymal cells in lacunae close to the epithelial follicle. In these areas the mineralized tissue resembled bone. In other foci, a linear arrangement of plump ectomesenchymal cells on the surface of the area where mineralized tissue formation occurred was noted (Figure 4A). In areas of more advanced tubular dentin formation, odontoblastic tubules were present. Tubular dentin adjacent to the epithelial follicle stained red and the more recently deposited dentin stained blue by the Masson Trichrome technique. The transition between the red and blue areas was sharp (Figure 4B). The outlines of enamel rods (which remain after demineralization) stain red with the Masson Trichrome Medical Technology SA Volume 26 No. 1 | June 2012 Figure 6A: Odontogenic myxoma. Thick type I collagen bundles exhibiting birefringence intersecting at obtuse angles to the delicate type III collagen which shows birefringence (arrows) (Picrosirius stain viewed with high intensity polarized light, X100). Figure 6B: Calcifications surrounded by radiating thick collagen bundles. The core of the acellular calcification was torn from the block during sectioning. (Masson Trichrome stain, magnification X200). technique, black with Reticulin stains and were non birefringent when stained by the Picrosirius method and viewed with high intensity polarized light. bres blue. The argyrophilia of the delicate reticulin fibres makes the Reticulin technique appropriate for their identification unlike the Masson Trichrome technique which stains the coarser fibres blue and fails to demonstrate the delicate reticulin fibres. Sections stained with the Picrosirius technique are viewed with high intensity polarized light making differentiation between the three most common collagen types (I, II and III) possible. At least six tumours in each of the major categories of odontogenic tumours (epithelial, mixed and ectomesenchymal) were included in the study. The odontogenic tumours in the ectomesenchymal group (odontogenic fibroma and odontogenic myxoma) differed in the quality of the ectomesenchymal component. In odontogenic fibromas, mature collagen type I fibres (yellow with strong birefringence) staining blue with the Masson Trichrome technique (Figure 5) and black and wavy with Reticulin stains, were present. The fibres ran roughly parallel to the inactive epithelial strands. Foci of mineralization were surrounded by concentric thick type I collagen bundles. Collagen in the myxoid interstitial tissue in odontogenic myxomas varied in quantity between the cases examined. In general long, coarse and wavy collagen type I fibres were oriented roughly parallel to each other and at obtuse angles to delicate and shorter collagen type III fibres (Figure 6A). Acellular calcifications in the stroma were surrounded by thick radiating type I collagen fibres (Figure 6B). The dormant odontogenic epithelial remnants failed to show a structured basement membrane zone. DISCUSSION Reports on the collagen fibre content of odontogenic tumours are infrequent in the literature. In a recent study on the collagen in the connective tissue walls of odontogenic cysts, employing only the Picrosirius staining technique, it was demonstrated that differences exist in the birefringent nature of collagen in the walls of inflamed- (dentigerous- and radicular cysts) versus non inflamed cysts (dentigerous- and odontogenic keratocysts) [6] . For this reason, areas of inflammation were not examined in our study. In order to avoid the shift in colour during polarization when viewing sections of different thicknesses [7], meticulous care was taken to prepare all sections at a thickness of 3 microns. Our study exploited several routine histochemical methods and immuno-histochemistry for collagen type IV to highlight- and type collagen in routine embedded wax blocks of several odontogenic tumours. The techniques included Reticulin stains which exploit the argyrophilic characteristic of collagen and in particular the delicate reticulin fibers and the colourful Masson Trichrome technique which stains course collagen fi- The capsules of all odontogenic tumours contained mainly type I collagen. Type IV collagen was not found in any tumour except for positivity in the basement membranes of blood vessels. The collagen fibres in the basement membranes of ameloblasts in ameloblastomas were found to be spatially organized with thick type I collagen passing perpendicularly through the basement membrane zone and merging with the collagen in the capsule and fibrous septa between the epithelial follicles. The Picrosirius staining technique showed delicate fibres with the staining characteristics for collagen type III between the coarse type I fibres. The organized arrangement of the collagen in the basement membranes of ameloblastomas may be helpful in distinguishing ameloblastomas from other odontogenic lesions with inactive epithelium. The lack of incorporation of plump ectomesenchymal cells adjacent to the basement membrane zone distinguishes ameloblastomas from ameloblastic fibromas in which induction of ectomesenchymal cells are present. The volume and direction of the collagen fibres deposited between the ameloblastic follicles had a bearing on the shape of the epithelial follicle, with plexiform growth patterns exhibiting denser collagen between the epithelium. Although the study did not include a case of desmoplastic ameloblastoma, we propose that extreme collagenization may be the reason for the flattened and atrophic morphology of the chords of odontogenic epithelium characteristic of this variant of ameloblastoma. Further research is indicated in order to determine whether the structure of the basement membrane zone of the desmoplastic ameloblastoma follows the description of the ameloblastomas reported in this study. ISSN 1011 5528 | www.smltsa.org.za 31 Medical Technology SA Volume 26 No. 1 | June 2012 In a paper on the collagen fibre component of adenomatoid odontogenic tumours, El Labban (1992) [8] describe a layer of fine filaments running perpendicular to the epithelial basal lamina, similar to that seen during induction of dentin formation. Stromal calcifications in these tumours mainly involve fine fibrils resembling amyloid, an observation supported by our study. The absence of an organized collagen fibre arrangement (as in ameloblastomas) in the basement membrane zones close to the epithelium in adenomatoid odontogenic tumours was noteworthy. The shape of the narrow anastomosing epithelial strands (which are reported to be present mainly at the periphery of adenomatoid odontogenic tumors [9]) was found to be the result of accumulation of collagen which appeared to restrict spatial enlargement of the epithelium. teodentin” is recommended. Although structurally similar, the term “cementum” should be reserved for mineralized deposits on the surface of a tooth root only. In our study odontoblastic tubules were apparent only in areas where formation of hard tissue was at a more advanced stage. Linear arrangement of plump ectomesenchymal cells on the surface of homogenized collagen, as demonstrated in our study, may be the first indication of tubular dentin formation as the arrangement of the cells mimics those of odontoblasts in the pulp of a tooth. The distinct difference in the colour- and sharp transition between recently formed- and more mature tubular dentin as demonstrated by the Masson Trichrome staining technique cannot be explained satisfactorily, except that it may reflect a chemical difference between the two dentin types. The fibres in the basement membrane zone of ameloblastic fibromas resembled those described in ameloblastomas. Adjacent to the basement membrane zone further differentiation of the ectomesenchyme was present. Collagen fibres surrounded individual plump ectomesenchymal cells, mimicking the first step in induction of mineralized tissue deposition. Due to the formation of collagen and subsequent expansion of the extracellular space, the cells in this zone were plump and it appeared less cellular than in the surrounding connective tissue. Collagen in the surrounding connective tissue was oriented in parallel bundles and the ectomesenchymal cells were inactive- appearing and compressed in greater density. Early signs of mineralized tissue induction, as described in ameloblastic fibro-odontomas, were not present. The role of collagen in determining the shape of the epithelial follicles in ameloblastic fibromas was noteworthy. Growth and enlargement of the epithelial follicles were generally found to be restricted in areas of dense collagen deposits, leading to enlargement of the epithelial follicle along ectomesenchymal planes of lesser resistance. The situation is analogous to the inflation of a balloon (epithelial follicle) in a closed hand, where the balloon will enlarge through the spaces between the fingers. This study suggests that although differences in the mitotic rate of the epithelium may play a role as a determinant of the shape of the follicle, the varying density of surrounding collagen undoubtedly determine the planes of enlargement of the follicle. This study is the first to propose that follicular, plexiform or multi-lobular shapes of the odontogenic epithelial follicles in odontogenic tumours are influenced by the density and spatial arrangement of collagen in the ectomesenchymal tissue around the follicles. Odontogenic fibromas are described microscopically as proliferations of varying cellularity with dispersed delicate collagen fibers in a fibromyxoid background and scattered groups of inactive appearing strands of odontogenic epithelium. In our study the epithelium lacked the delicate arrangement of fibres described for ameloblastomas and this feature may be helpful in distinguishing these two tumour types. Metaplastic dysplastic dentin, cementum or osteoid may be present [1]. The thick collagen fibres were suggested to distinguish central odontogenic fibromas from the connective tissue of dilated tooth follicles [11]. In our study odontogenic fibromas showed thick and wavy type I collagen bundles which were oriented roughly parallel to the inactive odontogenic epithelial strands. The epithelial basement membrane zones lacked the organized spatial arrangement of collagen observed in ameloblastomas. Foci of mineralization were surrounded by concentric collagen bundles in an unstructured way. These mineralized deposits, unlike those in odontogenic myxomas, could therefore be regarded as dystrophic in nature. With the aid of ultrastructural investigations, Josephsen, Larsson and Fejerskov (1980) [10] demonstrated a rim of finely filamentous meshwork separating the epithelium from the connective tissue in ameloblastic fibro-odontomas. This meshwork was demonstrated in this study to consist of two layers. The centrifugal fibres close to the ameloblasts showed the spatial arrangement described in the basement membrane zone of ameloblastomas and ameloblastic fibromas. The second layer showed the same morphology as in ameloblastic fibromas (plump ectomesenchymal cells surrounded by collagen), with foci of hard tissue deposits. The earliest sign of dental hard tissue depositioning was seen adjacent to the epithelial basement membrane zone as an area of homogenization of fibers around plump ectomesenchymal cells. In situations where ectomesenchymal cells are located within lacunae in a mineralized matrix and formation of odontoblastic tubules cannot be demonstrated, the term “os- 32 www.smltsa.org.za | ISSN 1011 5528 Odontogenic myxomas are characterized microscopically by randomly arranged stellate, spindle shaped and round cells with centrally placed nuclei with long pale cytoplasmic extensions dispersed in abundant mucoid or myxoid stroma [1]. Only a few collagen fibres are present and unlike odontogenic fibromas, odontogenic epithelial remnants are scarce. In a study by Simes (1975) [12] the stroma of odontogenic myxomas showed collagen bundles and smaller fibres similar to myxomas elsewhere in the body. Our study showed a varying quantity of collagen in odontogenic myxomas with thick type I collagen fibres that run roughly parallel. Tumours with an increase in collagen are generally referred to as fibromyxomas (or myxofibromas) [1]. There are no clear criteria reported in the literature for applying the latter terminologies and for this reason we recommend the use thereof to be suspended. More delicate collagen type III fibres intersect at obtuse angles to the main fibre type. This feature may be helpful in distinguishing peripheral odontogenic myxomas from oedematous irritation fibromas, a diagnostic pitfall which probably contributes to the low number of peripheral odontogenic myxomas recorded in the literature [13, 14]. Unlike the dystrophic calcifications identified in odontogenic fibromas, the structured arrangement of the collagen around the acellular calcifications in the stroma of odontogenic myxomas resembles Sharpey’s fibres radiating from acellular dental cementum. As cementum is defined by its location on the root surface of a tooth, the term “cementoid” is suggested for these deposits. Medical Technology SA Volume 26 No. 1 | June 2012 Acknowledgement The study was performed with the aid of a grant provided by the Department of Education and Training in 2010. REFERENCES 1. Philipsen HP, Reichart PA, Slootweg PJ et al. Odontogenic tumours. In: Barnes L, Eveson JW, Reichardt P, Sidranski D, eds. Pathology and Genetics: Head and Neck Tumours. Lyon: IARC Press, 2005; 283-381. 2. Poe FM, Dorling J, Nicholls AC, Web J. Molecular abnormalities of collagen: a review. J R Soc Med 1983; 76: 1050-62. 3. Stanley JR, Woodley DT, Katz SI, Martin GR. Structure and function of basement membrane. J Invest Dermatol 1982; 79 (suppl 1): 69s-79s. 4. Junqueira LU, Figueiredo MTA, Torloni H, Montes GS. Differential histological diagnosis of osteoid. A study on human osteosarcoma collagen by the histochemical Picrosirius- polarization method. J Pathol 1986; 148: 189-96. 5. HangelbroekJ, Vorster RJ, Raubenheimer EJ. The distribution of collagens types I-IV in pleomorphic adenoma. Med Tech SA 2008; 22(1): 3-4. 6. Vij R, Vij H, Rao NN. Evaluation of collagen in connective tissue walls of odontogenic cysts – a histochemical study. J Oral Pathol Med 2011; 40: 257-62 7. Junqueira LC, Montes GS, Sanchez EM. The influence of tissue section thickness on the study of collagen by the Picrosirius- polarization method. Histochemistry 1982;74:153-6. 8. El Labban NG. The nature of eosinophilic and laminated masses in the adenomatoid odontogenic tumor: a histochemical and ultrastructural study. J Oral Pathol Med 1992; 21(2): 75-81. 9. Neville BW, Damm DD, Allen CM, Bouquot JE. Oral and Maxillofacial Pathology. Philadelphia: Saunders, 2002: 621-3. 10. Josephsen K, Larsson A, Fejerskov O. Ultrastructural features of the epithelial-mesenchymal interface in an ameloblastic fibroodontoma. Scand J Dent Res 1980; 88(2): 79-95. 11. Hirschberg A, Buchner A, Dayan D. The central odontogenic fibroma and the hyperplastic dental follicle: study with Picrosirius red and polarizing microscopy. J Oral Pathol Med 1996; 25(3): 125-7. 12. Simes RJ, Barros RE, Klein-Szanto AJ, Cabrini RL. Ultrastructure of an odontogenic myxoma. Oral Surg Oral Med Oral Pathol 1975; 39(4): 640-6. 13. Perotti V, Rubini C, Fioroni M, Piattelli A. Soft tissue myxoma: a report of an unusual case located on the gingiva. J Clin Periodontol 2006; 33(1): 76-8. 14. Raubenheimer EJ, Noffke CEE. Peripheral odontogenic myxoma: A review of the literature and report of two cases. J Maxillofac Oral Surg 2011; In print. MEDICAL TECHNOLOGY SA Subscription Form Members of the Society receive the journal as part of their annual subscription. Non-members may only subscribe to the journal using this form. South African subscribers fees (Africa and overseas subscribers on application): R65.00 (for one issue); R120.00 (for two issues) I wish to subscribe to one (1) or two (2) issues of the journal. Surname: ................................................................................................. Initials: .................... Title: ............................ HPCSA No: ........................................................................................................................................................................ Postal Address: ................................................................................................................................................................... ............................................................................................................................................. Code: .................................. Daytime Contact Tel: ........................................................... Email Address: .................................................................... Please make payment/cheque payable to: The Society of Medical Laboratory Technologists of South Africa (SMLTSA) Payment by direct deposit: Standard Bank | Thibault Square 020909 (branch code) | 070950504 (account no.) Post completed form & a copy of the deposit slip as proof of payment to: The Administrative Office SMLTSA PO Box 505 | Howard Place 7450 Tel: +27 21 531 1231 | Fax: +27 21 531 1233 Signed: .................................................................................................................. Date: ................................................ ISSN 1011 5528 | www.smltsa.org.za 33