Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Major histocompatibility complex wikipedia , lookup
Monoclonal antibody wikipedia , lookup
Immune system wikipedia , lookup
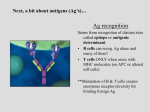
Lymphopoiesis wikipedia , lookup
Psychoneuroimmunology wikipedia , lookup
Molecular mimicry wikipedia , lookup
Adaptive immune system wikipedia , lookup
Cancer immunotherapy wikipedia , lookup
Immunosuppressive drug wikipedia , lookup
Innate immune system wikipedia , lookup
Immuno Exam 2 LECTURE 11 1. Activation of T cells requires what? A: Recognition of Ag displayed by APC 2. What are the two functions of the adaptive immune response? A: Help innate cells be better at clearing pathogen and set up a memory response and establish that response in certain tissue 3. What is the most potent APC? A: Dendritic cells 4. What are the other two forms of APC? A: Macrophages and B cells 5. Describe signal 1 in T cell activation. A: An immature (non-activated) APC has a microbial/viral peptide bound to its MHC class I. The T cell receptor (TCR) binds to the MHC class I. This sends a signal to the T cell. The presence of PAMP and/or an innate cytokine (“danger molecule”) promotes costimulatory molecule expression by APC 6. Describe Signal 2 in T cell activation. A: The costimulatory molecule, B7/CD80/CD86, on the APC binds with CD28 on the T cell. 7. Describe Signal 3 in T cell activation. A: The presence of a pathogen or innate cytokines induces cytokine production by APC, which go and bind to cytokine receptor on T cell, thus activating the T cell 8. What is the purpose of signals 1 and 2? What is the purpose of signal 3? A: Create proliferation; required for T cell survival and differentiation into active effector cells 9. What is the “Signal 3” that leads to Th2 production? What is Th2 cells function? A: IL-4; Initiate Ig production/Helminth immunity 10. What is the “Signal 3” that leads to Th1 production? What is Th1 cells function? A: IL-12; activate macrophages/intracellular microbe immunity 11. What is the “Signal 3” that leads to Th17 production? What is Th17 cells function? A: IL-6 + TGF-B; extracellular bacteria and fungi immunity 12. What are MHCs of humans termed? A: Human Leukocyte Antigens (HLA) 13. What is the function of MHC Class I molecules? A: Present peptide Ags to activate CD8+ T cells 14. What are the MHC Class I designations? A: HLA-A, HLA-B, and HLA-C 15. These genes encode regions of the…alpha or beta chain? A: alpha 16. The alpha chain combines with what for all MHC Class I molecules? A: β2-microglobulin 17. What are the “Non-classical” MHC Class Ib molecules? A: HLA-E, HLA-F, HLA-G 18. What is the function of HLA-E? A: Binds peptides as HLA Class I. Also, engages NK cells and can either inhibit by interaction with NKG2A/NKG2B or stimulate by interaction with NKG2C. 19. What is the function of HLA-F? Where is it found? A: Binds a restrictive set of Ags. Localized to the ER and Golgi with limited surface expression 20. What is the function of HLA-G? A: It is an inhibitory molecule that prevents mother immune cells from killing fetus 21. What are the “Non-classical” MHC Class Ic molecules? A: MICA and MICB 22. Where are they found? How do they function? A: They are found only in stressed cells. They override the inhibitory signal from MHC I in NK cells resulting in activation. 23. What does MIC lack that the other MHC Class I have? A: β2-microglobulin 24. What is the function of MHC Class II molecules? A: Present peptide Ags to activate CD4+ T cells 25. What are MHC Class II molecules designation? A: HLA-DP, HLA-DQ, HLA-DR, HLA-DM, HLA-DO 26. HLA Class II molecules consist of what chains? A: One alpha and one beta 27. What chains does HLA-DP consist of? Which chain shows higher polymorphism? A: Single alpha (DPA1) and beta (DPB1) chain genes; DPB1 28. What chains does HLA-DQ consist of? What degree of polymorphism do they show? A: Two pair of genes for both alpha & beta chains (DQA1, DQA2; DQB1, DQB2); moderately polymorphic 29. What chains does HLA-DR consist of? What degree of polymorphism do they show? A: Single alpha chain gene (DRA) – ALL DR molecules have this chain and Multiple beta chain genes (DRB1-9); DRA—low polymorphism, DRB—high polymorphism 30. What chain can lead to many autoimmune diseases? A: DRB 31. What kind of dominance does MHC genes inherited by parents show? A: Co-dominance 32. What chromosome possesses all the MHC genes? A: chromosome 6 33. What are the cells that express MHC Class II? A: Professional APCs, macrophages, and B cells 34. What are the cells that express MHC Class I? A: All nucleated cells 35. What is MHC restriction? Where does this occur in development? A: T cells recognize specific Ags only when displayed on self MHC molecules; imprinted in T cells during thymic development 36. Which MHC Class is closed ended? How many amino acids does it recognize? A: Class I; 8-11 amino acids 37. Which MHC Class is open ended? How many amino acids does it recognize? A: Class II; 10-30 38. List some MHC/Peptide binding characteristics. A: Bind only one peptide at a time Peptides acquired during intracellular assembly There is a broad specificity There is a very slow off-rate Stable expression requires a peptide MHC molecules bind ONLY peptides 39. Describe the MHC Class I production pathway. A: Viral proteins are ubiquinateddegraded into peptides by proteasomepeptides transported from cytosol to ERTAP directs cytosolic peptides into ERERAP trim cytosolic peptides to fit into MHC Class Iassembly of peptide class I complexes in ERcomplexes sent to golgi where packagedReleased in exocytic vesicle to be bound to cell membrane 40. The MHC Class II production pathway occurs only in what cells? A: Professional APCs 41. Describe the MHC Class II production pathway. A: Protein antigen endocytosedprocessing of internalized proteins in endosomal/lysosomal vesiclesMHC Class II produced in ER and stabilized by Ii (invariant chain)sent to golgi where packaged and released in an exocytic vesicleHLA-DM degrades invariant chain and CLIP to allow peptide bindingAssociation of processed peptides with MHC Class II molecules in vesiclesvesicle binds with membrane for expression of peptide-MHC complex 42. What is the importance of HLA-DM in the MHC Class II pathway? A: It allows for the removal of Ii and CLIP and stabilizes MHC Class II for peptide binding 43. What is cross-presentation? A: Taking exogenous pathogens and bringing them into DC and breaking them down for CD8+ T cells 44. How do monocytes and lymphocytes cross present Ags? Describe the mechanism A: Using HLA-F; Cell surface MHC I (without peptide) captures exogenous AgHLA-F stabilizes Ag capture MHC I-Ag & HLA-F internalized in endosome which fuses w/ lysosomeAg is trimmed to peptide, which binds to MHC Class I HLA-F transfers β2microglobulin to MHC I-peptide complexMHC-peptide shuttled to surface for Ag display 45. What is cross-dressing? A: DC can pass of entire MHC-I molecule to LN resident DC, which leads to memory of immunity against that Ag 46. CD8+ T cells bind to what chain of MHC I molecules during Ag presentation? CD4+ T cells bind to what chain of MHC II molecules during Ag presentation? A: alpha-3; beta-2 LECTURE 12 1. B lymphocytes lead to what form of immunity? A: Humoral 2. T lymphocytes lead to what form of immunity? A: Cell-mediated 3. Where do B cells develop? A: In the bone marrow 4. B cells develop where in the bone marrow? A: On the surface of bone marrow stromal cells 5. What cytokine is the survival factor for B cells? A: IL-7 6. What regions do the heavy chain consists of? A: V, D, and J 7. What regions do the light chain consists of? A: V and J 8. What is the process of heavy chain BCR development? A: The early pro-B cell undergoes D-J rearrangement Successful D-J triggers V arrangement in the late pro-B cell. (V-DJ rearrangement) VDJ rearrangement is successful, which leads to Pre-B cell to express a partial BCR 9. What enzyme leads to the DNA excision and RNA splicing in gene rearrangement of heavy chain? A: VDJ recombinase 10. What is the process of light chain BCR development? A: Light chain genes activated leading to V-J rearrangement in small pre-B cells Successful light chain rearrangement of VJ results in BCR expression (m heavy chain, k or l light chain) IgM expressed on surface 11. What is the major characteristic of mature B cells? A: They coexpress IgD and IgM 12. Coexpression of IgD and IgM are made possible by what? A: mRNA alternate splicing 13. 85% of BCR light chain is what? 15%? A: kappa; lambda 14. Successful rearrangements maintain what receptor expression? What happens if they lose this expression? A: IL-7; apoptosis 15. What is allelic exclusion? A: The process in which one of the two genes for which an individual is heterozygous is expressed, while the other gene is excluded 16. BCR diversity is generated by what? A: Recombinase 17. Where are Recombination Recognition Sequences (RRS) located? A: 3’ end of V gene segments 5’ end of D gene segments 3’ end of D gene segments 5’ end of J gene segments 18. What is a heptamer and what is its function? A: It is a highly conserved stretch of 7 nucleotides adjacent the coding sequence; enhances binding of RAG recombinase to RRS and specifies site of DNA cleavage 19. What is a nonamer? A: The binding site to anchor RAG to DNA 20. What is the function of the spacer? A: Provide efficient V(D)J recombination by properly aligning the heptamer and nonamer 21. The beta chain refers to what in the BCR/TCR? Alpha chain? A: heavy chain; light chain 22. What are the two enzymes involved in junctional diversity and what do they do? A: TdT—terminal deoxynucleotidyl transferase: adds N-nucleotide to H chain; Polm—DNA polymerase mu: adds N-nucleotides to L chain 23. What do surviving B cells express that traffic them to secondary lymphoid organs? A: CXCR5 24. Where do T cells develop TCR? A: Thymus 25. What chain first undergoes rearrangement in TCR? Describe TCR rearrangement. A: beta; DJ rearrangement occurssuccess triggers V-DJ rearrangementconstant (C2) region is spliced to rearranged VDJ following transcriptionPre-TCR expressedalpha chain rearrangement promotedTCR is expressed on T cell surface 26. Describe the selection process that follows TCR rearrangement. A: TCR upregulates CD4 and CD8weak or no binding to CTEC MHC leads to apoptosis, however moderate to strong binding to CTEC MHC allows the T cell to live 27. What occurs to the surviving T cells? A: They will then express either CD4 or CD8. In the MTEC they encounter dendritic cells that present self-antigen. Tight binding of the T cell leads to apoptosis, moderate binding allows the T cell to live. Naïve mature T cells exit the thymus and move to the periphery. 28. True or False. T cells with successful gamma/delta rearrangement usually express their function TCR and remain DN T cells? A: True 29. Surviving T cells express what and traffic to the secondary lymphoid organ? A: CCR7 LECTURE 13/14 1. What is the goal of cell-mediated immunity? A: To eliminate intracellular pathogens 2. What phosphorylates tyrosines in the immunoreceptor tyrosine-based activation motif (ITAM)? A: Lymphocyte-specific protein tyrosine kinase (Lck) 3. What releases Lck from CD4/8? A: Ag recognition 4. Phopshorylated ITAMs recruit what molecule? What is this molecules function? A: ZAP-70; it binds to phosphotyrosines and phosphorylates adaptor proteins, including LAT (linker for activation of T cells) 5. Phosphorylated LAT activates what pathway and what molecule? A: Ras pathway and Phospholipase C (PLC) 6. PLC activates what two mechanisms? A: IP3, which increases Ca2+ in the cytosol and Protein Kinase C (PKC) 7. What is the function of PKC in cell-mediated immunity? A: It phosphorylates IkB, which releases NF-kB that moves into the nucleus and promotes production IL-2 8. What is the function of glucocorticoids? A: Block NF-kB activation, inhibit Lck action, and suppress TCR calcium signaling 9. How does NF of activated T cells (NFAT) lead to IL-2 production? A: Calcium ions bind to calmodulinCalmodulin activates calcineurinCalcineurin removes phosphate from NFATNFAT migrates to nucleus to promote IL-2 production 10. What is the function of cyclosporine? A: To inhibit calcineurin activity 11. Why is cyclosporine used in transplant patients? A: To inhibit the activation of T cells against the new organ 12. What is the function of the Ras/Rac-MAPK (AP-1) pathway? A: c-Fos and c-Jun form transcription factor AP-1 (activating protein-1), which enhances transcription of several genes – Differentiation (cytokines) – – Proliferation Apoptosis (Fas ligand) 13. What does stimulation of T cells by IL-2 leads to? A: Clonal expansion, survival, and differentiation 14. What happens in clonal expansion? A: T cells proliferate about 100,000-fold 15. What happens for survival? A: IL-2 induces expression of anti-apoptotic proteins, BcI, and increases gene expression of CD25 (IL-2 receptor) 16. How does IL-2 lead to differentiation? A: IL-2 promotes gene expression of CD40 ligand and cytokine recpetors for Th1 and Th2. 17. What is the function of CD69? A: It stabilizes the T cell-DC engagement to ensure signal 3 acquisition. It is an activation marker of the adaptive immunity 18. What is the function of CD40 ligand? A: It is critical for the development of antibody responses 19. What is the function of CTLA-4? A: It is released 3 days after T cell activation to regulate expansion 20. How does CTLA-4 function? A: It has a greater affinity for CD28, than CD80/86 does. It strips the phosphate groups off and shuts down proliferation. 21. What are the three groups of adhesion molecules employed by trafficking T cells to infiltrate tissue? How do each function? A: Selectin ligand—found on the T cell and binds to selectin molecules on injured tissue epithelium Chemokine receptors—bind chemokines on proteoglycans that are released from the damaged tissue Integrins—bind to integrin receptors on damaged tissue epithelium 22. What do T cells “spit out”, once adhered to tissue epithelium, in order to get to damaged tissue area? A: ECM proteases 23. Th1 cells develop with what cytokine’s help? A: IL-12 24. Th2 cells develop with which cytokine’s help? A: IL-4 25. Th17 cells develop with which cytokines’ help? A: TGF-B and IL-6 26. Where does IL-4 come from in the lymphoid organs for Th2 development? A: Activated Basophils 27. What are the Th1 cell effector functions? A: Th1 cellIFNγmacrophage activation/IgG productionfight intracellular microbes 28. How does IFNγ enhance macrophage function? A: IFNγ increases ROS/NO productions, inflammatory cytokines, and increase MHC Class I expression of infected cell. It also promotes IgG production, which can opsonize microbe and be recognized by NK cells for cell death 29. What are the Th2 cell effector functions? A: Th2 cellIL-4, IL-5, IL-13Mast cell/eosinophil activation, IgE production, “alternative” macrophage activationFight helminthic parasites/wound healing 30. How do IL-4, IL-5, and IL-13 enhance function? A: IL-4 initiates antibody (IgG and IgE) production, IL-4/IL-13 stimulates GIT mucus secretions and peristalsis (diarrhea), IL-5 enhances eosinophil function, and IL-4/IL-13 promote wound healing by activating alternative macrophages 31. What are the Th17 cell effector functions? A: Th17IL-17 and IL-22neutrophilic/monocytic inflammationfight against extracellular bacteria and fungi 32. What is IL-17 function? A: It promotes inflammation and recruits neutrophils to infection 33. What is IL-22 function? A: It promotes increased barrier function 34. What protects CD8 T cells from killing itself by release of perforin/granzyme? A: serglycin 35. CD8 T cells kill by two methods…what are they? A: Perforin/granzyme and Fas Ligand interacting with Fas on infected cell 36. What are the two death receptor pathways? A: FasL-Fas and TNF-TNFR 37. What molecule can out compete caspase-8 and block apoptosis in the FasL-Fas death pathway? A: c-FLIP 38. Describe the two Complex of TNF-TNFR pathway. A: Complex I—TNF binds to TNFRTRADD+TRAF2+RIP1 bind to TNFRpromotes cFLIP/initiates NF-kB activationblocks apoptosis/inflammation; Complex II—Activated TNFR1 is endocytosedTRADD/TRAF2/RIP1 complex dissociates TNFR TRADD/TRAF2/RIP1 recruits FADD and caspase-8 (complex II) apoptotic machinery activated (provided that the levels of cFLIP are low enough to remove inhibition) 39. Promotion of what cytokines in the mitochondrial death pathway induces anti-apoptotic BcI-2 protein expression? A: IL-2, IL-7 and growth factors 40. What is BcI-2 proteins function? A: Bind Bim, which prevents Bax and Bak oligomerization (apoptosis) 41. Development of CD8+ T cell responses depends on what cytokine? A: IL-2 42. Where are central memory T cells located? Effector memory T cells? A: Remain in lymph node; traffic to tissues 43. What cytokine drives expansion of memory T cells? Survival? A: IL-15; IL-7 44. Describe the relationship of the levels of IL-7R, IL-2R, and IL-15R as naïve, activated, and memory maturation. A: Naive Activated Memory IL-7Rhi IL-7Rlo IL-7Rhi IL-2Rlo IL-2Rhi IL-2Rlo mid hi IL-15R IL-15R IL-15Rhi LECTURE 15 1. What is the goal of humoral immunity? A: eliminate extracellular pathogens and neutralize toxins 2. Antigen flows in to lymph nodes from tissue via what mechanism? A: afferent lymphatics 3. What are the two types of B cells? A: B-1 cells and B-2 cells 4. What are the two types of B-2 cells? Where are they found? A: Follicular B cells and Marginal Zone B cells; Spleen 5. What are follicular B cells activated by? A: Thymus-dependent antigen 6. What are marginal zone cells activated by? A: They are thymus-independent antigens (polysaccharide, lipids, etc.) 7. Where are B-1 cells found? A: Mucosal tissue and peritoneal cavity 8. What are B-1 cells activated by? A: Polysaccharides, lipids, etc. (thymus-independent) 9. What are the transcription factors that result from BCR ligation signaling? A: NFAT, NF-kB, AP-1 10. What does syk (in B cells) correspond to in T cells? A: ZAP-70 11. What is the functional response induced by antigen-mediated cross-linking of the BCR complex? A: Proliferation and anti-apoptotic factors 12. What is the response of activation of B-lymphocytes? A: expression of antigen presentation machinery; MHC Class I and II and B7 (CD80/CD86) 13. What follows the expression of antigen presentation machinery? A: Expression of cytokine receptors—IL-2R, IL-4R, IL-5R, and IL-21R 14. What chemokine is expressed that directs migration of B cell to T cell zone? A: CCR7 and down regulation of CXCR5 15. CXCR5+ naïve Th cells also express what? Where do these cells congregate? A: CXCL13; interfollicular zone (area just outside the paracortex side of the follicle) 16. What activates Pre-TFH cells? A: Resident DC 17. What does activation of T cell lead to? A: CD40 ligand expression and cytokine secretion 18. What is the purpose of CD40 ligand? A: It gives the antibody response 19. What cytokines do Pre-TFH cells secrete? A: IL-2, IL-4, and IL-5 20. Where do activated Pre-TFH cells engage activated B cells? A: The interfollicular zone 21. How do Pre-TFH cells induce/assist in B cell proliferation? A: Secretion of cytokines and binding of CD40L 22. What does a defective CD40L expression result in? A: X-linked hyper-IgM syndrome 23. What is the function of Activation Induced Deaminase (AID)? A: It is required for Ig class-switch recombination and somatic hypermutation 24. What is somatic hypermutation? A: A high rate of mutations that occur in the variable region of both heavy and light Ig chains, which leads to selection of high-affinity B cells 25. What are the 3 major functions of Bcl-6? A: It differentiates Th into TFH cells It stabilizes CD40L and CXCR5 expression It induces production of IL-21 and IL-21R expression (autocrine) 26. What is the function of IL-21/IL-21R? A: It co-stimulates mature T and B cell proliferation and differentiation and also potentiate NK cytolytic functions, inducing NK terminal differentiation 27. Where do B cells and TFH cells migrate once they are activated? A: B cell zone and germinal centers 28. What occurs in the dark zone of germinal centers? A: TFH IL-21 promotes robust proliferation and surface BCR diminish, thus forming centroblasts 29. What are centrocytes? A: They represent centroblasts that have completed somatic hypermutation and now express a BCR 30. What occurs in the basal light zone of germinal centers? A: Centrocytes engage FDC, which leads to affinity maturation 31. What must occur for centrocytes to avoid apoptosis? A: Their BCR and CD21 must bind with high affinity to what the FDC is presenting. 32. What make up CD21 ligands? A: cleaved C3 fragments of complement 33. What happens to the surviving centrocytes? A: They engaged TFH cells and differentiate into plasma cells 34. What signals promote proliferation and differentiation of B cells into plasma cells? A: CD40 and IL-21 35. When are short-lived plasma cells formed? What is their fate? A: They are formed during initial TFH cell and B cell interaction in the interfollicular zone; they undergo apoptosis as plasmablasts (precursor of long-lived PC) are generated 36. What is the function of memory B cells? Do they produce antibodies? A: They serve as a reservoir for memory B cell responses/long-lived plasma cells. They can differentiate into Ig-producing plasmablasts upon Ag encounter; No antibody production 37. Where are long-lived plasma cells found? A: Inflamed/infected tissue or bone marrow 38. What do long-lived PC do in inflamed tissue? A: They secrete high levels of Ig at Ag source site and undergo apoptosis as Ag decreases 39. What do long-lived PC do in bone marrow? A: They never leave the marrow and constantly secrete low levels of Ig. 40. What plasma cells are the most important in vaccination? A: Bone marrow long-lived PC 41. Which Ig are monomers? A: IgG, IgE, IgD 42. Which Ig is a dimer? A: IgA 43. Which Ig is a pentamer? A: IgM 44. Which cytokines proliferate centroblast to centrocytes? A: Il-2, IL-4, IL-5 45. IFN-γ leads to differentiation of centrocyte into plasma cells that secrete which Ig? A: IgG1, IgG2, IgG3 46. TGF-β leads to differentiation of centrocyte into plasma cells that secrete which Ig? A: IgA 47. IL-2, IL-4, and IL-5 lead to differentiation of centrocyte into plasma cells that secrete which Ig? A: IgM 48. IL-4 leads to differentiation of centrocyte into plasma cells that secrete which Ig? A: IgE and IgG4 49. What is isotype switching? A: The switching of the C region of the heavy chain 50. What are 4 important reasons of isotype switching? A: Response against nonprotein Ag Neutralization of virus and toxins Prevent mucosal colonization Eliminate parasitic helminthes 51. What is the process of IgMIgG1 isotype switch? A: There are switch (S) regions between each of the C regions genesCD40 activates AIDspecific cytokines and CD40 direct AID to selected S regions (SM and SG1)DNA in the S regions is nickedA loop is formed between the two nicked DNA regions Loop cleaved off and IgG1 is produced 52. Can isotype switch be reversed? A: No 53. What are immune complexes (IC) composed of? A: Secreted Ig bound to Ag 54. How is Ig production regulated? A: IC are captured on B cells by FcR to activate phosphatase to remove phosphates from BCR signaling proteins 55. What three ways can antibodies neutralize microbes? A: Antibodies prevent the binding of microbes to cells and thus block the ability of the microbes to infect host cells. Antibodies inhibit the spread of microbes from an infected cell to an adjacent uninfected cell. Antibodies block the binding of toxins to cells and thus inhibit the pathologic effects of the toxins. 56. What is the purpose of antibody opsonization of microbes? A: Enhance phagocytosis 57. What cells demonstrate antibody-dependent cell cytotoxicity (ADCC)? What antibody do each use? A: NK cells—IgG and eosinophils—IgE 58. What is the function of IgG1-3? A: Neutralization, opsonization, complement activation, ADCC, cross placenta 59. What is the function of IgG4? A: Opsonization, ADCC, cross placenta 60. What is the most common serum Ig? A: IgG1 61. Which IgG are the best at opsonization? A: IgG1 and IgG3 62. What is the first Ig made in newborns? A: IgM 63. What is the function of IgA? A: Mucosal immunity and neutralization 64. What does the J chain of IgA do? A: Provides structural stability and aids in translocation 64. Where does the secretory piece of IgA come from? What is its function? A: Poly-Ig receptor on the basolateral surface; it protects the IgA from proteolysis 65. What is the function of IgM? A: Complement activation, agglutination of microbes, opsonization 66. What are two important characteristics of IgM? A: It is first Ig synthesized by B cells and the first BCR expressed on naïve mature B cells 67. What is the function of IgE? A: Immunity to parasites and allergic responses LECTURE 16 1. What does induction mean? A: First detection 2. What is effector? A: Response to induction 3. What are the top two worldwide deaths annually from mucosal infections? A: Acute resp infections (4 million) and HIV (2.9 million) 4. What is the MALT? A: Mucosa-associate lymphoid tissue. It is highly specialized immune system that protects mucosal surfaces 5. What are the components (7) of the MALT? A: Gastrointestinal tract (GALT) Bronchial tree (BALT) Nasopharyngeal area (NALT) Mammary gland Salivary and lacrimal glands Genitourinary organs Inner ear 6. What are the scattered lymphoid cells of the MALT? Organized lymphoid tissues? A: Intraepithelial lymphocytes; Peyer’s patch 7. What is the effector site of the gut? A: Lamina propria 8. What cytokine predominates in the Peyer’s patch? A: TGF-β 9. What is Waldeyer’s ring? A: An interrupted circle of protective lymphoid tissue at the upper ends of the respiratory and alimentary tracts 10. What is the structure of mucosal immunity? A: External environmentcontinuous epithelial cell layer sitting on a basement membraneloose connective tissue (lamina propria)dense connective tissue that connects mucosa with smooth muscle (submucosa) 11. What is found in the lamina propria? A: Blood vessels, lymphatic vessels, and MALT 12. When can commensals become lethal? A: If they cross the mucosal barrier and enter the circulation or traverse the intestinal wall 13. True or false. The GALT is an integral part in only innate defense. A: False, innate and adaptive 14. How is the GALT an integral part of innate defense? A: Produces chemokines, cytokines, and defensins 15. How is the GALT an integral part of adaptive defense? A: Antigen uptake and transfer by M cells to DC Uptake and secretion of IgA Produce growth factors for IELs 16. What are mucins comprised of and what is their function? A: They contain oligosaccharides and glycoproteins; They prevent microbial contact with epithelial cell layer, serve as a matrix to capture and concentrate secreted defensins, she to bind to bacterial pili, large amounts can form a glycocalyx to prevent attachment 17. What cytokines induce mucin synthesis? A: IL-1, IL-6, TNF, Type I IFNs and PMN elastase 18. What part of the GALT immunity are mucins, defensins, and TLRs? A: innate 19. What are defensins? A: Small peptides that inhibit membrane synthesis 20. What cells produce defensins in the small intestine? A: Paneth cells found in crypts 21. What cells produce defensins in the large intestine? A: Intestinal epithelial cells 22. Which TLRs do intestinal epithelial cells express? A: TLR 2, 4-7, and 9 23. Signaling through TLRs leads to what function? A: Increased tight junction expression and proliferation of enterocytes 24. What TLR is mainly expressed on the basolateral surface of the intestinal epithelia? Why? A: TLR4 so that if any commensals find their way through the epithelium and into the lamina propria, they can bind them and signal a response. Don’t want them on lumen side because that would lead to constant inflammation because of all the commensal and other bacteria in the gut 25. What cytokine dominates in the GALT? A: TGF-β 26. What cell is vital in the adaptive response of the GALT? A: Microfold (M) cells 27. Where are M cells located? A: The region that overlies the Peyer’s patches and other GALT structures 28. What are M cells function? A: the transcellular transport of various substances from the lumen of the intestine across the epithelial barrier to underlying APC. 29. Describe the process of M cell transcytosis. A: M cell takes up antigen by endocytosis/phagocytosisantigen is transported across the M cell in vesicles and released at the basal surfaceantigen is bound by DC, which activates T cells 30. What are the two types of DC in the gut? A: CD103- CD11b+ DC and CD103+ DC 31. What is the function of CD103- CD11b+ DC? A: They can extend dendrites into the gut lumen and sample Ags Increased levels of bacterial ATP in gut lumen promotes IL-1, IL-6, IL-12, and TGF-β production 32. What is the result of the microbial antigens and cytokine release by CD103- DC? A: Th1 and Th17 cell differentiation 33. What is the function of CD103+ DC? A: TSLP secreted by enterocytes upon NLR signaling 34. What production by CD103+ does TSLP promote? A: TGF-β, IL-10 and retinoic acid 35. What are the functions of those cytokines in the gut? A: Needed to make Treg cells 36. What is Foxp3+? A: Transcription factor for Treg cells 37. What is the result of microbial response on CD103+? A: Th2 and Treg cell differentiation 38. What are the two types of GALT T lymphocytes? A: Lamina propria T cells and IEL T cells 39. What type of T cells predominate in lamina propria? What do they secrete? A: CD4 γδ+ cells; secrete IFN-γ, IL-5, and IL-10 40. What types of T cells predominate in IEL? What is their function? A: CD8 γδ+ cells; responds to low levels of Ag with perforin and granzyme and modulate the kinetics of epithelial cell renewal 41. Which GALT T cells are the cells that promote chronic inflammation of IBD? A: Lamina propria T cells 42. How do T cells enter Peyer’s patches from the blood vessels? A: They are directed by homing receptors CCR7 and L-selectin 43. How do T cells become activated in Peyer’s patches? A: They encounter antigen presented by DC 44. How do T cells return to the gut? A: They drain from the mucosa via mesenteric lymph nodes to the thoracic duct and enter the bloodstream. Their homing receptors guide them to where they belong in the gut 45. What must an activated T cell be expressing in order to home to the lamina propria and intestinal epithelium of the small intestine? A: CCR9 and α4:β7 integrin 46. Epithelial cells expressing MIC-A and MIC-B have undergone what signal? A: Stress signal as a result of infection, damage, or toxic peptides 47. What is it on IELs that binds to MIC-A,B and activate the IEL? A: NKG2D 48. What method does the IEL kill the stressed cell? A: perforin/granzyme pathway 49. What must be present to signal differentiation of naïve T cells to T regs? A: TGF-β 50. What cytokines lead to an isotype switching of and an increase in IgA? A: IL-10 and TGF-β 51. What is the dominant class of Ig in MALT? A: IgA 52. What is the structure of IgA in blood? In MALT? A: monomer; dimer 53. What are the mechanisms of protection by IgA? A: Inhibition of adherence Virus neutralization Neutralization of enzymes and toxins Immune exclusion and inhibition of antigen absorption 54. What does humoral response mean? A: Immune response of PC producing Igs to fight microbes 55. What are the three methods of activity by IgA? A: Secreted IgA on the gut surface binds and neutralizes pathogens and toxins IgA binds and neutralizes antigens in endosomes IgA exports toxins and pathogens from lamina propria while being excreted to lumen LECTURE 18 1. What are the settings requiring artificial immunity? A: Patients with defective humoral immunity Exposure to a disease will likely cause complications Not adequate time between exposure and active immunization to protect Effects of a current infection can improve with immunization 2. What is the difference between passive and active artificial adaptive immunity? A: Passive is transferring of Ig to assist with the opsonization/neutralization of a pathogen. Active is providing a vaccination (active or inactive) of the antigen to allow the body to build antibodies to fight the antigen if encountered 3. What is the immunization schedule of DTaP? A: First dose—2 months old, second dose—4 months old, third dose—6 months old, fourth dose—15-18 months old, fifth dose—4-6 years old 4. What is the immunization schedule of MMR? A: First dose—12-15 months and second dose—4-6 years old 5. What delays the measles vaccine until 12-15 months of age? A: Interference from maternal Ig binding to Ags 6. Why were multiple immunizations of polio vaccine used? A: To ensure adequate immunity generated against the three strains of the poliovirus 7. What is the “Herd immunity” idea? A: That if the majority of a population is immune to an agent, then the chance of a susceptible individual contacting an infected person is very low. 8. What is thought to account for outbreaks of agents for which vaccines are available? A: A decrease in herd immunity 9. What happened in the measles outbreak of the 1980s? A: 88% of the people who fell ill were unvaccinated. Of those who had been vaccinated they only received 1 vaccine. This led to recommendation for children to receive 2 MMR vaccinations 10. What are the strategies of vaccine development? Describe. A: Safety—vaccine must not cause illness or death Protection—vaccine must protect against illness resulting from live pathogen exposure at point of entry Sustained protection—protection must last several years to life of vaccine Induce neutralizing Ig—effective protection from some pathogens requires preexisting Ig at time of exposure Induce CMI—more effective elimination of pathogen, Ig production and memory formation Other—low cost, stability/storage, administration route, few side effects, manufacturer cost 11. What are live, attenuated vaccines? A: Microbes are cultured to lose the ability to cause significant disease but retain capacity for transient growth in host. Microbes are grown for prolonged periods under abnormal culture conditions and adapts to growth in other host cells and much less in human cells. 12. What was the discovery Jenner made from cowpox? A: He found that some agents provide crossreactive protection from related pathogens. During the smallpox epidemic, he saw that women who milked cows that had cowpox did not obtain the smallpox virus. They only obtained small skin lesions from cowpox. Thus he determined that there was a relationship between the cowpox and building immunity to smallpox. 13. What are the diseases that can be vaccinated using live, attenuated vaccines? A: measles, mumps, rubella, polio, rotovirus, TB, varicella, and yellow fever 14. What are some disadvantages of live, attenuated viruses? A: Requires refrigeration May mutate to virulent form (reversion) Immunosuppressed patients cannot receive 15. What are some advantages of live, attenuated viruses? A: Strong immune response Lifelong memory Few doses (due to transient growth) 16. What are inactivated or killed vaccines? A: They are from microbes that are inactivated by chemical treatment (previously heat) so the pathogen can induce immunity but has no capacity to replicate in the host 17. What are the diseases that can be vaccinated by inactivated or killed vaccines? A: cholera, hep A, influenza, plague, polio, rabies 18. What are the advantages of killed vaccines? A: No refrigeration required No threat of reversion Safe for immunosuppressed patients 19. What are the disadvantages of killed vaccines? A: Weaker immune response Several doses to induce effective immunity 20. What are the forms of subunit (acellular) vaccines? A: Toxoids, capsular polysaccharides, recombinant proteins 21. What does vaccination of toxoids lead to? What are example vaccines? A: Neutralization of Ig; diphtheria and tetanus 22. What does vaccination of capsular polysaccharides lead to? What are example vaccines? A: Opsonization of Ig; Streptococcus pneumonia and Neisseria meningitides 23. What is used as part of the recombinant protein vaccination? A: Expressed Ags 24. What does vaccination with recombinant proteins lead to? What is an example vaccine? A: Neutralizing and/or opsonizing Ig; Hep B virus vaccine 25. What are the diseases that can be vaccinated by acellular vaccines? A: Diphtheria, tetanus, Hep B, Pertussis, Strep. Pneumonia 26. What are the disadvantages of acellular vaccines? A: Require adjuvant for immune response and they are difficult to produce 27. What are the advantages of acellular vaccines? A: Immune system targeted to recognize toxin Specific Ags used so low chance of adverse reactions Safe for immunosuppressed patients 28. What are adjuvants? A: They are substances that enhance the immunogenicity of Ags. They often contain aluminum salts, which bind to the toxoid to stimulate Ig response 29. What is responsible for increase Ag uptake and processing, MHC Class II, CD40 and CD86 (B7)? A: Aluminum salts 30. What immune cells do most adjuvants act on to mature? A: APCs 31. What are conjugate vaccines? A: Polysaccharides that are conjugated to protein carriers to provide a good antibody response. 32. True or False. Conjugate vaccines induce B cell memory and T cell memory responses. A: False, no T cell memory response 33. Describe how the conjugate vaccine works. A: The BCR is specific for the polysaccharide region of the conjugatethe conjugate is internalized and processedpeptides from the protein component are presented to the T cellT cell provides help to the B cell by CD40L binding to CD40the B cell produces antibodies against the polysaccharide region of the pathogen 34. What are DNA vaccines? A: Proteins expressed in vivo from bacterial plasmids encoding proteins for gene therapy 35. How are DNA vaccines delivered? A: Gene gun 36. What do DNA vaccines include? A: One microbe gene that includes cytokine genes, which activate APC and improve immunogenicity of Ags 37. How are most vaccines given? A: IM injection 38. What are the disadvantages of injections? A: Painful and expensive Unpopular with the recipient Mass vaccination by injection is tedious Injection may not be most effective way of stimulating an appropriate response as it does not mimic the usual route of entry 39. What administration has become the main focus of delivery? A: Nasal or oral mucosal administration LECTURE 19 1. What does test for the presence of antigens lead to? A: Diagnosis of disease 2. What does testing for the presence of antibodies or cells lead to? A: Determining how well the body is responding to disease 3. What correlates with an increased number of neutrophils? A: bacterial infection 4. What correlates with an increased number of lymphocytes? A: intracellular infections such as viruses 5. What correlates with IgM presence? A: Recent exposure to the immunogen 6. What correlates with IgG presence? A: Patient exposed to immunogen days to months ago 7. What is the purpose of serology? A: To detect, identify and quantitate Ag in clinical samples, and to evaluate the Ig response to infection. 8. What are the two methods of serology? A: Immunoassays for Cell-Associated Ags and Immunoassays for Ig and soluble Ags 9. What are immunoassays for cell-associated Ags? A: Immunofluorescence (IF), Enzyme Immunoassay (EIA), Flow Cytometry (FC) 10. What are immunoassays for Ig and soluble Ags? A: Immunoprecipitation (IP), Enzyme-Linked Immunosorbent assay (ELISA), Radioimmmunoassay (RIA), and agglutination 11. IF and EIA use what type of light to excite the fluorochromes? A: UV light 12. What is the difference between direct and indirect IF/EIA? A: Direct results from fluorochromes, bound directly to Ig, binding to Ags. Indirect results from secondary Ig labeled with fluorochromes bind to Ig that is bound to Ags. 13. What excites fluorochromes in FC? A: Laser 14. What does FC use to compare separate molecules detected? A: dot plots 15. What method is used to sort cells into fluorescent and non-fluorescent? A: Fluorescence Activated Cell Sorting (FACS) 16. What is FSC and what does it determine? What is SSC and what does it determine? A: Forward scatter—size of cells; Side scatter—density of cells 17. What strategies are used to analyze FC data? A: Gating strategies 18. Describe the steps of gating in FC. A: Isolate the population of cell of interest o Draw a box (gate) around the desired cells Exclude unwanted cells (dead) o Draw gate around desired cells (alive) Select for specialized cell (CD3+) o Draw gate around desired specialized cell Examine specific cell population in the specialized cell sample o Draw gate around each to look at specific cell population 19. What is used to bind to phospholipid membrane of apoptotic/dead cells in FC? A: Aqua dye 20. What cells represent the 42.4%? What cells represent the 24.1%? A: CD8-CD3+; CD8+CD3+ 21. Describe the process of immunoprecipitation. A: Protein in solution in test tubeadd Ig against protein of interestIg binds to protein of interestAdding a protein A or G binds to antibody making it insolublecentrifugeremove supernatant (solution) and keep pellet 22. What is an ELISA? A: It is a procedure used to detect Ags or Igs. Ags or Igs are attached to a solid surface (plastic plates) and a test sample is added. An enzyme system is then attached to the Ag-Ig complex for detection. 23. What does an indirect ELISA detect? A: Antibodies 24. Describe the Indirect ELISA. A: Coat plate with purified Agwash away unbound Agadd blocking agent to bind up free siteswash away unbound blocking agentadd patient samplewash away unbound Igadd enzyme conjugated Igs specific for Fc region of primary Igwash away unbound enzyme-Ig complexadd substratecolor formationmeasure absorbance (concentration) 25. What does a direct ELISA detect? A: Antigens 26. Describe the Direct ELISA. A: Coat plate with purified Igwash away unbound Igadd blocking agent to bind up free siteswash away unbound blocking agent add patient samplewash away unbound AgAdd enzyme-conjugated Ig to make a “sandwich”wash away unbound enzymeIgadd substrateNegative controls omit unknown Ag (Positive), Positive controls use known Ags 27. How does an indirect agglutination work? A: It detects patient serum (Ig) against cell Ags attached to latex beads, or Igs may be attached to beads to test for presence of Ag.





























![[11] No. of printed pages :04](http://s1.studyres.com/store/data/007988662_1-961bf8618b5025cca8d341deaebfcd3c-150x150.png)