Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
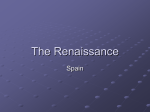
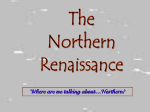
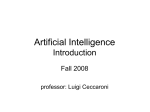
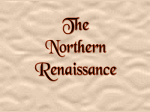
Physiopathology of Malnutrition • CALORIC EQUILIBRIUM : Meal energy stored into High Energy Phosphates , Fat and Glycogen • Stores are mobilized daily during : – fasting – Increased energy expenditure (cold, activity, disease) – NO STORES = reduction of nutrients demand, no chances to meet extra demands and reduction of activities down to MAX ADAPTATION Luigi Greco - Faculty of Medicine of the University of Gulu Hypothetical Model for the Coupling of Starvation to the Compensatory Response That Serves to Restore Lost Weight Schwartz, M. W. et al. N Engl J Med 1997;336:1802-1811 Luigi Greco - Faculty of Medicine of the University of Gulu Hypothetical Model for the Interaction of Insulin and Leptin with Hypothalamic Neuropeptide Y and Corticotropin-Releasing Hormone (CRH), Neuropeptides That Can Stimulate the Hypothalamic-Pituitary-Adrenal Axis Schwartz, M. W. et al. N Engl J Med 1997;336:1802-1811 Luigi Greco - Faculty of Medicine of the University of Gulu Model to Explain the Differences between Neuroendocrine Responses during Active Weight Loss and Those during the Maintenance of Stable, Reduced Weight in an Obese Person Schwartz, M. W. et al. N Engl J Med 1997;336:1802-1811 Luigi Greco - Faculty of Medicine of the University of Gulu Adaptation to Restriction of Calories and/or Proteins • Adaptation to the lowest metabolic equilibrium : – – – – Susceptibility to infections, overall fragility to offenses Functional alterations correlate with protein depletion Hormonal-mediated adaptation Fat mobilization from adipose tissue Luigi Greco - Faculty of Medicine of the University of Gulu Hormonal Adaptive Mechanism Hormone Stimulus Results Insulin Glucose Amino acids Protein synthesis (muscle) Growth Growth Hormone Glucose Amino acids Lipogenesis Protein synthesis (body) Glucose Amino acids Growth Lipolysis Urea synthesis Protein turnover (viscera) Glucocortucoids Thyroid Hormones Neoglucogenesis Lipolysis metabolism Energy homeostasis Protein turnover Calorie depriv Protein depriv Decreased Decreased Variable, generally normal Increased Increased Variable, generally normal Decreased Decreased Energy PY Y Nucleo arcuato GHrelin a Luigi Greco - Faculty PY of Medicine of the University of Gulu Y Initial Phase of PCM • • • • Decreased physical activity Lower basale energy expenditure Decreased fat body mass and then lean body mass Muscle catabolism release amino acids Progression of PCM Decreased lean body mass (non fatty mass) Energy expenditure adequate to the lean body mass Faster decrease of lean body mass (no feed back) Luigi Greco - Faculty of Medicine of the University of Gulu Protein Deficit • Decrease in the protein • Synthesis (altered amino acid proportions) • Catabolism (altered Free Amino Acid Pool) • • • • • • Catabolism >>> Synthesis (Anabolism) Stop to any growth process No renewal of tissue (skin, intestinal mucosa, hairs ) Decreased protein turnover Altered distribution of proteins Albumin lower in tissue = oedema Luigi Greco - Faculty of Medicine of the University of Gulu COMMON COMPLICATIONS • INFECTIONS – Less Immunoglobulins – Impaired Cell-mediated immunity – Impaired tissues barrier protection – – – – EFFECTS : Increased energy demand Anorexia Tissue catabolism and destruction Luigi Greco - Faculty of Medicine of the University of Gulu ADAPTATION TO PCM • • • • • • • Sparing of body proteins Decreased body protein mass Decreased oxygen consumption Decreased demand of energy Reduction of total body K Decreased Hemoglobin : less O2 Slower cardiac activity : hypotension Luigi Greco - Faculty of Medicine of the University of Gulu Physiological Consequences • KIDNEY : decreased filtration, low urea • Increased Na retention and total body water • MUSCLE : wasting, reduced strenght, reduced capacity to purchase and eat food • INTESTINE : impaired absorption • Diarrhoea and malabsorption (fat, CH, proteins) • CNS : Depression Luigi Greco - Faculty of Medicine of the University of Gulu Severe Calorie Deficiency • • • • • • • Hypoglicemia Hypotermia Impaired Circulatory function Impaired Renal function Acidosis Tissue breakdown and complication Coma and death Luigi Greco - Faculty of Medicine of the University of Gulu Progressive Fatal Malnutrition • LIVER : inability to synthetize – – – – – – – Albumin Clotting factors Transport Proteins Haemorragic diathesis Fatty Liver Stress proteins and Cortisol Jaundice Luigi Greco - Faculty of Medicine of the University of Gulu Luigi Greco - Faculty of Medicine of the University of Gulu