Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
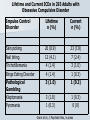
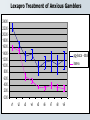
Neurobiology and Pharmacological Treatment of Pathological Gambling Jon E. Grant, JD, MD, MPH Associate Professor University of Minnesota School of Medicine Minneapolis, MN Disclosure Information I have the following financial relationships to disclose: – Grant/Research support from: Forest Pharmaceuticals, GlaxoSmithKline I will discuss the following off-label use and/or investigational use in my presentation: – All medications used to treat impulse disorders are off-label and include - SSRIs, lithium, antiepileptics, opioid antagonists, stimulants, antipsychotics, calcium channel blockers, muscle relaxants, antiemetics Impulse Control Disorders Pathological gambling Kleptomania Compulsive sexual behavior Compulsive buying Pyromania Compulsive Internet use Trichotillomania Intermittent Explosive Disorder Core Features of Impulse Control Disorders Repetitive or compulsive engagement in a behavior despite adverse consequences Diminished control over the problematic behavior An appetitive urge or craving state prior to engagement in the problematic behavior A hedonic quality during the performance of the problematic behavior. Common Core Qualities of Behavioral Addictions Tolerance Withdrawal Repeated unsuccessful attempts to cut back or stop Impairment in major areas of life functioning Motivational Neural Circuits Multiple brain structures underlying motivated behaviors. Motivated behavior involves integrating information regarding internal state (e.g., hunger, sexual desire, pain), environmental factors (e.g., resource or reproductive opportunities, the presence of danger), and personal experiences (e.g., recollections of events deemed similar in nature). The ventral striatum receives input from the ventral tegmental area and prefrontal cortex and has direct access to and influence on motor output structures. Hypothalamic and septal nuclei provide information about nutrient ingestion, aggression and reproductive drive Amygdala - affective information Hippocampus - contextual memory data. Neurochemistry of Impulsivity SEROTONIN Impulsivity Glutamate Dopamine Norepinephrine Role of Serotonin Decreased serotonin associated with adult risk-taking behaviors - alcoholism and pathological gambling. Blunted serotonergic responses in the ventromedial prefrontal cortex - in individuals with impulsive aggression Implicated in disadvantageous decisionmaking - adults with gambling or drug addictions Role of Dopamine Dopamine release into the nucleus accumbens - translates motivated drive into action - a “go” signal Dopamine release associated with rewards and reinforcing Dopamine release - maximal when reward is most uncertain, suggesting it plays a central role in guiding behavior during risk-taking situations. Biochemistry - Norepinephrine Norephinephrine (NE) - an important component in the mediation of arousal, attention and sensation-seeking in PG PG had higher CSF levels of MHPG and higher urine levels of NE. Correlations found between scores of extraversion (Eysenck Personality Questionnaire) and CSF MHPG, Plasma MHPG, urine VMA and the sum of NE and NE metabolites Biochemistry – Opioid System The endogenous opioid system influences the experiencing of pleasure. Opioids modulate mesolimbic DA pathways via disinhibition of γaminobutyric acid input in the ventral tegmental area. Gambling or related behaviors have been associated with elevated blood levels of the endogenous opioid β-endorphin. Neuroimaging Ventromedial prefrontal cortex (vmPFC) implicated in decision-making circuitry in risk-reward assessment Decreased activation in vmPFC in PG subjects during gambling cues performance of the Stroop Color-Word Interference Task and simulated gambling. Responsiveness of the vmPFC to serotonergic drug challenges (m-CPP, fenfluramine) - blunted in impulsive aggression and alcohol dependence Left vmPFC Implicated During Stroop Performance In ICDs R PG Control (Potenza et al, (Potenza et al, 2003, Am J 2003, Am J Psychiatry) Psychiatry) L PG - Control Bipolar - Cont (Potenza et al, (Blumberg et al 2003, Am J 2003, Arch Gen Psychiatry) Psychiatry) Pathological Gambling Source: Look Magazine, March, 1963 Characteristics Age: usually begins in early adulthood Gender: 32% female, 68% male Males tend to start at an earlier age Telescoping phenomenon Mean time: 16 hours per week Amount Lost: 45% of gross annual income Triggers: – Advertisements, Boredom, Stress Personal Consequences Lying to friends/family Borrowing money Credit cards Attempted suicide Alcohol and other drug problems Psychiatric conditions including major depression and anxiety disorders 44% 30% 64% 24% 50% 40-60% Compulsive Disorder? Impulsive Disorder? Both? Lifetime and Current ICDs in 293 Adults with Obsessive Compulsive Disorder Impulse Control Disorder Lifetime n (%) Current n (%) Skin picking 26 (8.9) 23 (7.8) Nail biting 12 (4.1) 7 (2.4) Trichotillomania 4 (1.4) 3 (1.0) Binge Eating Disorder 4 (1.4) 1 (0.3) Pathological Gambling Kleptomania 3 (1.0) 1 (0.3) 3 (1.0) 1 (0.3) Pyromania 1 (0.3) 0 (0) Grant et al., J Psychiatr Res, in press Impulsive-Compulsive Impulsivity = predisposition to rapid reactions to stimuli without regard for negative consequences Compulsivity = repetitive behaviors with the goal of reducing/preventing anxiety or distress, not for pleasure or gratification May occur simultaneously or at different times within the same disorder Co-Occurring Disorders in PG 70 60 50 40 30 20 10 0 SUDs Affective Anxiety ICDs Gambling Urges and Nicotine Use 7 6 5 4 Gambling Urge Intensity 3 2 1 0 Never Used Prior Use Current Use Problem Gambling and Compulsive Sexual Behavior: Unrecognized Co-Occurring Disorders 225 Pathological Gamblers 27 (12%) current co-morbid CSB 44 (19.5%) lifetime CSB CSB - most common co-morbid impulse control disorder Rates of CSB 3X in study of psychiatric patients (12%-19.5% compared to 4.4%) Clinical Characteristics Age of onset: CSB preceded PG for 70.3% PG with CSB were significantly more often male than PG alone PG with CSB significantly more often had at least one ICD than PG alone (61.4% vs. 27.1%) PG + CSB subjects more likely (82%)than PG subjects (65%) to smoke PG + CSB score higher on Eysenck impulsivity scale than PG subjects or CSB subjects Impulse Control Disorders in Gay/Bisexual Men Compared to Heterosexual Men with Pathological Gambling MIDI Diagnosis Gay/Bisexual (n = 22) Heterosexual (n = 83) Lifetime Current Lifetime Current 5 (22.7) 4 (18.2) 12 (14.5) 10 (12.0) Compulsive sexual behavior, n (%) 13 (59.1) ‡ 11 (50.0) ‡ 14 (16.9) 8 (9.6) Kleptomania, n (%) 1 (4.5) 0 (0) 3 (3.6) 2 (2.4) Trichotillomania, n (%) 0 (0) 0 (0) 2 (2.4) 2 (2.4) Pyromania, n (%) 0 (0) 0 (0) 1 (1.2) 0 (0) 18 (81.8) † 15 (68.2) † 37 (44.6) 29 (34.9) Compulsive buying, n (%) Any MIDI diagnosis, n (%) Short-Term Single-Blind Fluvoxamine Treatment of PG Mean PG Y-BOCS Score PG Y-BOCS Gambling Behavior Score 14 12 10 Rx response (N = 10) Responders (n=7) Nonresponders (n=3) 8 6 4 2 0 Baseline 1 2 3 5 7 8 Treatment Week Hollander et al, Am J Psychiatry 1998;155:1781-1783 Percentage of Patients Achieving Response (PG-CGII Score of 1 or 2) During Treatment with Paroxetine or Placebo 70 Paroxetine (N=34) Percentage of Patients 60 Placebo (N=37) 50 40 30 20 10 0 1 2 4 6 8 10 12 Week 59% response rate in the paroxetine group 49% rate in the placebo group 45 completers (Grant et al. 2003) 16 Subtyping Look at family history, comorbidities Anxiety reduction/affective/obsessional Pleasure/urge General impulsivity/need for stimulation Anxiety/Depressive/Obsessionality SRI medictaions Anxiolytics CBT Lexapro Treatment of Anxious Gamblers 24.00 22.00 20.00 18.00 16.00 14.00 12.00 10.00 8.00 6.00 4.00 2.00 0.00 pg-ybocs - total ham-a v1 v2 v3 v4 v5 v6 v7 v8 v9 Pleasure/Urge Relapse prevention techniques Naltrexone Acamprosate Baclofen Isradipine Ondansetron Opioid Antagonists The mu-opioid system: underlies urge regulation through the processing of reward, pleasure and pain, at least in part via modulation of dopamine neurons in mesolimbic pathway through GABA interneurons. linked to physiological responses during Pachinko. Nalmefene 16 weeks Randomized 25mg, 207 15 50mg, 100mg, placebo subjects centers N-Acetyl Cysteine Amino acid and antioxidant Lack of significant side effects Levels of glutamate within the nucleus accumbens mediate reward-seeking behavior NAC potentially modulates brain glutamate transmission Stimulates inhibitory metabotropic glutamate receptors, and thereby reducing synaptic release of glutamate and dopamine. Restores extracellular glutamate concentration in the nucleus accumbens Appears to block reinstitution of compulsive behaviors and decrease cravings. Open-Label Study 27 men and women aged 18 to 75 with a primary diagnosis of pathological gambling Required to have a score of 16 or greater on the Yale Brown Obsessive Compulsive Scale Modified for Pathological Gambling (PG-YBOCS) Stable dose of other psychotropics 8 weeks Dosing schedule: – 600mg/day x 2 weeks – 1200mg/day x 2 weeks – 1800mg/day x 2 weeks Those who responded were randomized for 6 additional weeks to double-blind medication 25 20 15 Baseline Endpoint 10 5 0 PG-YBOCS Total Score Urge/Thought Score 100 90 80 70 60 50 40 30 20 10 0 Active Placebo Week 0 Week 2 Week 4 Week 6 Impulsivity Attentional – consider stimulants Impulsive – anti-epileptics or lithium Lithium carbonate SR – Double-blind study – Bipolar spectrum disorders – 29 completers – 83% responders – mean dose 1170mg/day Bipolar Spectrum Pathological Gamblers PG-YBOCS Total Score Over Time Mean PG Y-BOCS Score 28 24 20 * 16 Placebo Lithium * 12 * 8 4 0 0 1 2 3 4 5 6 7 8 9 10 Week * p<.05 Hollander et al, 2002 Other potential medications Topiramate Acamprosate Baclofen Isradipine Antabuse Heterogeneity of Impulse Control Disorders Anxiety driven Affective Impulse driven driven Urges/cravings driven Conclusions Subtyping based on clinical characteristics, comorbidity, and family history Different medications for different subtypes May also apply to psychotherapeutic interventions Acknowledgments