Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Lymphopoiesis wikipedia , lookup
Hospital-acquired infection wikipedia , lookup
Polyclonal B cell response wikipedia , lookup
Hygiene hypothesis wikipedia , lookup
Molecular mimicry wikipedia , lookup
Innate immune system wikipedia , lookup
Monoclonal antibody wikipedia , lookup
Psychoneuroimmunology wikipedia , lookup
Cancer immunotherapy wikipedia , lookup
Management of multiple sclerosis wikipedia , lookup
Adoptive cell transfer wikipedia , lookup
Multiple sclerosis research wikipedia , lookup
X-linked severe combined immunodeficiency wikipedia , lookup
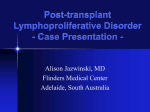
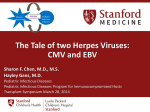
ANATOMIC PATHOLOGY Review Article Posttransplantation Lymphoproliferative Disorders FIONA E. CRAIG, M.D., MARGARET L. GULLEY, M.D., AND PETER M. BANKS, M.D. ficiency,18"23 PTLDs are unique in regard to potential resolution with diminished immunosuppression. '-8 Eradication of such invasive, often pleomorphic proliferations by restitution of immune competency also raises profound questions about the definition of lymphoid neoplasia. In this review article the difficulties that may be encountered in making the diagnosis of PTLD are presented, as is a pathogenetic model to explain the unique characteristics of this disorder and a summary of available therapeutic options. Posttransplantation lymphoproliferative disorders (PTLDs) currently affect approximately 2% of all organ allograft recipients.1 This problem has increased in magnitude in recent years both because of newly available powerful immunosuppressive agents and the steady increase in the number of organs transplanted.2 In 1990 more than 20,000 allogeneic organ transplants were performed in the United States.23 Although individual pathologists are unlikely to acquire a broad experience with PTLDs, they are likely to encounter occasional cases in the course of their routine practice. Furthermore, because PTLDs may occur months or even years after transplantation,4"7 the challenge of diagnosis is not confined to pathologists in health care facilities directly engaged in organ transplantation. It is essential that posttransplantation proliferative disorders be recognized early, because they can often be cured with appropriate therapy.1,8 Without accurate diagnosis and appropriate treatment, these disorders are potentially rapidly fatal.9"12 The pathologist with little experience with PTLDs will often render an erroneous diagnosis of lymphoma, applying the criteria for the diagnosis of conventional lymphomas occurring in nonimmunocompromised patients. Lymphoproliferative disorders occurring in association with immunosuppression, however, are unique. They have a predilection for extranodal sites,4,13 a varied morphologic appearance,5 a strong and probably causal association with Epstein-Barr virus (EBV) infection,4,614 frequent absence of immunophenotypic6,15 or genotypic6,'6''7 evidence of monoclonality, and a poor response to the cytolytic chemotherapeutic or irradiation regimens used for lymphoma.6,9"12,18 Although these features are shared to some extent by tumors occurring in patients with either congenital or acquired immunode- DIAGNOSIS The incidence of PTLD varies with the organ transplanted and with the nature and severity of the accompanying immunosuppressive regimen.7,20,24 Posttransplantation lymphoproliferative disorders affect approximately 0.6% of patients after bone marrow transplantation,25 1-5% of renal graft recipients,26 and 1.820% of patients after cardiac transplantation.15,16,19"21 The correct and early diagnosis of PTLD is complicated by its wide spectrum of clinical presentations and the difficulty in distinguishing it from other more frequent complications of organ transplantation—allograft rejection and opportunistic infection. The following clinical symptoms and signs aid in the diagnosis of PTLD and carry prognostic implications as well. Clinical Presentation Posttransplantation lymphoproliferative disorder presents at a variable interval after transplantation. The length of this interval apparently is related to the immunosuppressive regimen used.1 Currently most allograft recipients are treated with regimens containing the immunosuppressive drug cyclosporin A (CsA). PosttransDepartment of Pathology, University of Texas Health Science Center plantation lymphoproliferative disorders developing in CsA-treated patients can occur within 1 month of transat San Antonio, San Antonio, Texas. plantation,7 and therefore the initial presentation is easAddress reprint requests to Dr. Banks: Department of Pathology, ily confused with rejection or infection. Similarly, immuUniversity of Texas Health Science Center at San Antonio, 7703 Floyd nosuppression with anti-T-lymphocyte monoclonal Curl Drive, San Antonio, TX 78284-7750. 265 266 ANATOMIC PATHOLOGY Review Article antibodies, e.g., OKT3, also is associated with a high incidence and early onset of PTLDs.27 In patients receiving regimens with neither CsA nor anti-T-lymphocyte monoclonal antibodies, PTLD develops no earlier than several years after transplantation.7 Posttransplantation lymphoproliferative disorder has a mode of presentation that varies with the organ transplanted, the immunosuppressive regimen, and the age of the patient.117'20 Although some patients may be asymptomatic or display localized lymphadenopathy, in others the disease may be widely disseminated and involve multiple organs and lymph node groups.1 The group in which spread has occurred has a poor prognosis, particularly when there is coexistent sepsis.1 Most frequently PTLD is localized regionally to a group of nodal or extranodal tissues.117'20 Patients recognized early in the course of their disease with limited organ involvement may respond to conservative treatment.1 Included in this group of responders are those with an infectious mononucleosis-like syndrome characterized by fever, pharyngitis, and cervical lymphadenopathy.4'619 Typically such patients are young (mean age, 23 years),4 present within the first 9 months of immunosuppression, and are receiving CsA. This mode of presentation contrasts with that in older patients (mean age, 48 years), in whom PTLD arises later after transplantation.20 Although older patients typically have symptoms of a localized tumor mass in the setting of less immunosuppression, they respond poorly to therapy.20 Posttransplantation lymphoproliferative disease in patients treated with CsA-containing regimens has a distinct predilection for the gastrointestinal tract.713,28 Patients with disease confined to this system often do well despite multifocal distribution of their disease and the frequent complication of visceral perforation.8 Other sites of localized organ involvement have included the lung, kidney, prostate, and engrafted organ.14 Although primary central nervous system disease is relatively common in patients receiving treatment protocols lacking CsA, inclusion of CsA in the treatment protocol usually restricts involvement of the central nervous system to patients with advanced multiorgan dissemination of PTLD.7-19 Pathologic Diagnosis The diagnosis of PTLD typically involves both the clinical and anatomic pathology laboratories. Microbial detection methods are important in excluding opportunistic infections and may be used to document the presence of EBV.18 Epstein-Barr virus has been identified in virtually all cases of PTLD using genetic techniques; culture and serologic studies, however, are less sensitive in detecting EBV. Although serologic studies are some- times successfully applied to demonstrate primary infection1,29 or reactivation of EBV infection,24 they are not entirely reliable because a serologic response may be absent or abnormal in immunosuppressed patients.4'6'18 Histologic analysis of tissue biopsies is required to establish the diagnosis of PTLD. Although the results of immunohistochemical and gene rearrangement studies may have some prognostic bearing, they are of little value in primarily establishing the diagnosis. Accurate interpretation of paraffin-embedded tissue sections provides the clinicians with critical information needed for immediate treatment of the patient. The histologic diagnosis of PTLD is made difficult by its wide spectrum of morphologic appearances. This spectrum has prompted the subdivision of PTLD into various categories (Table 1). Although we recommend the simplified morphologic and empiric classifications of PTLD, the most frequently used classification is that proposed by Frizzera and co-workers in 1981.5 The authors of this landmark study recognized that PTLDs exhibit a range of histologic appearances, and proposed that these morphologic features are predictive both with regard to the presence of clonality and to biologic behavior. They presented a model in which the disorders progressed consistently from polymorphic, polyclonal, benign lymphoid proliferations to monomorphic, monoclonal malignant disorders.30 The two ends of this histologic spectrum are defined by diseases that have histologic counterparts in nonimmunocompromised patients—nonspecific reactive hyperplasia manifests histologic features resembling those seen in infectious mononucleosis, whereas immunoblastic sarcoma was defined as a morphologically uniform proliferation of atypical immunoblasts. Frizzera proposed also that there are two intervening distinct phases of PTLD: polymorphic diffuse B-cell hyperplasia and polymorphic B-cell lymphoma. These lymphoid proliferations share a polymorphic cellular composition and the capacity for tissue invasion; however, polymorphic B-cell lymphoma was defined as neoplastic because of the presence of extensive necrosis and large, atypical, sometimes multinucleated immunoblasts. Although this classification illustrates the range of histologic appearances encountered in PTLDs and emphasizes the invasive potential of these disorders, subsequent investigation has raised doubts about its scientific validity and prognostic utility.1 PTLDs do not appear to follow such a predictable progression, and the criteria proposed to define malignancy (cellular atypia and necrosis) neither correlate with demonstration of monoclonality nor predict which patients will have progressive disease despite reduced immunosuppression.29 Therefore, we have elected to use a simpler morphologic classification. We acknowledge A.J.C.P. • March 1993 CRAIG, GULLEY, AND BANKS Posttransplantation Lymphoproliferative Disorders 267 TABLE 1. CLASSIFICATION SYSTEMS FOR LYMPHOPROLIFERATIVE DISORDERS OCCURRING AFTER TRANSPLANTATION Genotypic* Morphologic, Proposed by Frizzera1 Simplified Morphologic lgH EBV c-myc - - - Polymorphic diffuse B-cell hyperplasia Polymorphic diffuse B-cell lymphoma Polymorphic PTLD Immunoblastic sarcoma Monomorphic PTLD Usually responds spontaneously + 1 + 1 Typical reactive hyperplasia 1 1+ + Nonspecific reactive hyperplasia Empirical - + + + Responds frequently to reduced immunosuppression Responds less frequently to reduced immunosuppression lgH = clonal immunoglobulin H gene rearrangement: EBV = clonal cpisomal Epstcin-Barr virus genome: c-myc = c-myc rearrangement: PTLD = posttransplantation lymphoprolifera- tive disorders: + = clonal gene rearrangement: * Modified from Locker and Nalesnik.32 that transplant recipients develop typical follicular and/ or paracortical lymph node hyperplasia, and classify atypical lymphoid hyperplasia as PTLD.1 This noncommital term was adopted to avoid implications in regard to the neoplastic nature of a condition that defies such assessment by histologic, immunophenotypic, or even genetic probe analysis.829 Histomorphologic studies yield only one distinction that may be of prognostic significance—specifically, monomorphism.1 Posttransplantation lymphoproliferative disorders composed of a monomorphic population of immunoblasts is more likely to progress despite a reduction in immunosuppression than is a polymorphic PTLD.1 Therefore we do not advocate use of the classification proposed by Frizzera, and recommend only two morphologic categories: polymorphic PTLD and monomorphic PTLD.1 The only truly reliable predictor of good outcome, however, appears to be empirical—a favorable response to reduced immunosuppression.1'7'8 In summary, transplant recipients may develop typical lymphoid hyperplasia that resembles that seen in nonimmunocompromised patients and resolves spontaneously. Atypical lymphoid proliferations (PTLDs) often display microscopic features such as cellular atypia and invasion which, if occurring in an immunocompetent patient, would be diagnostic of malignancy. In the setting of reversible immunosuppression, however, the diagnosis of malignant lymphoma should be avoided. The polymorphous nature of PTLD is useful in distinguishing it from the infiltrate of small lymphocytes that characterize rejection. Many PTLDs display a polytypical mixture of lightchain expression by immunohistochemical analysis despite morphologic and clinical features that are suggestive of lymphoma.815 Southern-blot analysis for immunoglobulin heavy- and light-chain gene rearrangement in PTLDs has revealed polyclonal, oligoclonal, and monoclonal lesions,15 and even the presence of different individual clones in biopsy specimens taken from different sites in the same patient.16'31 The method of Activation/immortalization of B cells by EBV ^ , FRV * * absence ofclonal gene rearrangement. m " * * * QJL Jfe Apoptosis/immune cytolysis Latent infection/immune control of EBV infection Maturation Immunosuppression/loss of immune control Apoptosts/immune cytolysis Genetic event Oncogene activation/tumor suppressor gene inactivation »i*# • • ! • • • * • « Ancillary Studies Lymphoma in immunocompetent patients is invariably monoclonal, therefore immunophenotypic and genotypic analyses often are used to confirm the diagnosis. Similar analysis has not proved as useful in PTLDs. • • • CTL a Cytotoxic T lymphocyte * = EBV = Epstein-Barr virus CsA o Cyclosporin A FIG. 1. Hypothetical schema of the pathogenesis of posttransplantation lymphoproliferative disorders. Vol. 9 9 - N o . 3 268 ANATOMIC PATHOLOGY Review Article FIG. 2. Section of lymph node from an immunocompetent patient with acute infectious mononucleosis (case 1). There is effacement of the architecture and extensive necrosis (hematoxylin and eosin, original magnification X250). genotypic analysis is extremely sensitive and can detect small monoclonal populations within even an extensive polyclonal background. Therefore the results may not correlate with immunohistochemical evidence for polyclonality.1517'25 The demonstration of neither immunoglobulin light-chain restriction8 nor clonal immunoglobulin gene rearrangement, however, accurately predicts the patient response to therapy.1'21 Although polymorphic, polyclonal tumors appear to resolve more frequently than monoclonal, monomorphic tumors,19'21'24'29 this observation is of limited value in the treatment of an individual patient.6 Furthermore, the lesion analyzed is not necessarily representative of lymphoid proliferation in other sites.16 A critical analysis of FIG. 3. Perivascular clusters of viable lymphoid cells, including large bizarre-appearing immunoblasts resembling Reed-Sternberg cells in case 1 (hematoxylin and eosin, original magnification X630). # A.J.C.P. • March 1993 CRAIG, GULLEY, AND BANKS 269 Posttransplantation Lymphoproliferative Disorders FIG. 4. Polymorphous PTLD developing in a renal transplant recipient (case 2). There is a diffuse effacing polymorphous infiltrate of lymphocytes, including immunoblasts, small cleaved cells, and plasma cells. Several individual necrotic cellsand tingible body macrophages are present. No zones of necrosis are present (hematoxylin and eosin, original magnification X250). genotypic data by Locker and Nalesnik32 has revealed several potential prognostic indicators. These authors ascribed prognostic significance to the intensity of monoclonal bands identified by Southern-blot analysis.32 A strong clonal band indicates a relatively large proportion of cells from one clone and appears to correlate with disease progression despite reduced immunosuppression. By contrast a weak band is less significant. The clonality of PTLD also was demonstrated by structural analysis of the episomal EBV DNA that is present in virtually all cases.32 Employing this technique, PTLDs with varying combinations of EBV and immunoglobulin heavy-chain gene clonality could be identified and compared with their responses to reduced immunosuppressive therapy (Table 1). Although the demonstration of clonal EBV DNA is one ofthe most sensitive methods FIG. 5. Monoclonal, polymorphous PTLD developing in a renal transplant recipient (case 3). Section of the submental lymph node displaying effacement ofthe architecture by a diffuse, polymorphous lymphocytic infiltrate. Numerous tingible body macrophages impart a "starry sky" appearance. There is necrosis of individual cells but only small geographic zones of necrosis (hematoxylin and eosin, original magnification X250). Vol. 99 • No. 3 270 ANATOMIC PATHOLOGY Review Article FIG. 6. The infiltrate contains a mixture of immunoblasts, small cleaved cells, and plasma cells (Case 3). A similar lymphoid infiltrate was identified in the salivary gland (hematoxylin and eosin, original magnification X630). for the detection of a monoclonal proliferation, its prognostic utility remains uncertain. The presence of a clone of lymphocytes containing episomal EBV DNA may be used to separate lymphadenopathy that requires treatment with reduced immunosuppression, i.e., PTLD, from more typical, polyclonal, or EBV-negative lymph node hyperplasia that may resolve spontaneously. An association between disease progression and c-myc oncogene rearrangement has been reported.32 Although the latter observation may provide a clue about the pathogenesis of PTLD and its progression to a true neoplasm, this rearrangement is found in too few cases to be of diagnostic value. The response to an initial reduction in immunosuppression still appears to be the most important indicator of outcome, and therefore immediate assessment of such treatment should not be delayed in deference to any of these ancillary studies. nated with that of the normal tissues, and persists in the same excessive manner after cessation of the stimuli which evoked the change."33 Therefore, PTLD that progresses despite a clinical trial of reduced immunosuppression is probably best considered to be neoplastic, i.e., malignant lymphoma. In all other situations the term PTLD is recommended. The multiple factors involved in the pathogenesis of PTLDs can be simplified into a three-step process that leads to the development of neoplasia14 (Fig. 1). The first step is the activation and immortalization of B lymphocytes by EBV. Step two is a progression of proliferation due to immunosuppression. The resulting rapid and uncontrolled EBV-provoked proliferation greatly increases the chance of a genetic event that irreversibly transforms the lymphocytes into malignant cells (step 3). The mechanisms involved in these three steps follow. PATHOGENESIS Posttransplantation lymphoproliferative disorder includes a spectrum of EBV-related disorders ranging from lymphoid hyperplasia to neoplasia. These disorders result from the interplay of multiple factors that can be regarded as the multiple steps required for the production of a neoplasm. At what point should these proliferations be regarded as neoplastic? In this setting, clonality, invasion, and metastasis are not useful criteria. An appropriate, albeit older, definition of neoplasia is "an abnormal mass of tissue which exceeds and is uncoordi- Step 1 Epstein-Barr virus is a ubiquitous virus with a putative role in the pathogenesis of Burkitt's lymphoma and nasopharyngeal carcinoma.18 Reactivation of latent EBV infection, or less frequently, of primary EBV infection, is strongly associated with the development of PTLD.34 Primary EBV infection is a productive, cytolytic infection.24 Latent infection appears to be a balance between periodic viral shedding from the oral epithelium, secondary B-cell infection, and immune destruction of infected cells by cytotoxic T lymphocytes.418'24 This balance can A.J.C.P. -March 1993 271 CRAIG, GULLEY, AND BANKS Posttransplantation Lymphoproliferative Disorders be disrupted by increased EBV-induced B-cell proliferation and by decreased immune destruction. The EBV proteins, latent membrane-protein-1 and EBV nuclearantigen-2, are important in producing EBV-stimulated B-cell proliferation and immortalization in vitro.35 These proteins are strongly expressed in PTLD and may contribute to the lymphoid proliferation by up-regulating the expression of the autocrine growth factor CD23.35 The expression of these genes also leads to the production of surface antigens, which in a nonimmunocompromised patient would stimulate T-cell cytotoxicity. By contrast, the cells of Burkitt's lymphoma lack B-cell activation antigens (e.g., CD23), adhesion molecules, and EBV-associated latent proteins (e.g., latent membraneprotein- 1 )52636and are therefore invisible to the immune system. Despite the strong expression of surface antigens, the cells of PTLD continue to proliferate, unabated by the immune system. x •« S r* n <s Step 2 The similarity of PTLD to proliferations seen in other acquired and congenital immunodeficiency syndromes, and the regression of the disease after reduction in immunosuppressive therapy both support the central role of immunodeficiency in the pathogenesis of this disorder. The increased incidence of cancer in immunocompromised patients was initially attributed to decreased immune surveillance and impaired recognition and destruction of cancer cells.37 More recent theories, however, center around the role of the immune system in the control of EBV infection.24 Although many immunosuppressive regimens are currently used, the incidence, interval to onset, and nature of PTLD appear to be most dependent on the dose of CsA. This agent prevents allograft rejection in a highly specific way by blocking the activation of alloreactive cytotoxic T lymphocytes through a reduction in interleukin-2 production and interleukin-2 receptor expression. Cyclosporin A also inhibits the activation of EBV-specific cytotoxic T lymphocytes, which confounds the patient's defense against EBV-induced Bcell proliferation. In addition to cell lysis, EBV-infected lymphocytes die by apoptosis. Apoptosis (programmed cell death) is a process of single cell death that involves intrinsic pathways and appears to be independent of the viability of surrounding cells. Apoptosis may, however, be induced by an interaction with cytotoxic T lymphocytes.38 Single cell death is a prominent feature of EBV infection in immunocompetent hosts, and may be construed as a self-sacrifice of infected cells. This process can be disrupted by factors either extrinsic or intrinsic to the cell. Intrinsic mechanisms include the EBV infection of FIG. 7. Southern blot analysis performed on the lymph node (1) and salivary gland (2) from case 3, revealing a monoclonal population of B cells. Restriction enzymes used are indicated above each autoradiogram. Arrowheads indicate the germline bands, and lines indicate clonal rearrangement of the immunoglobulin heavy-chain gene (JH probe, Oncor, Gaithersburg, MD) with the enzymes HindlW and BamHl. The clonal rearrangement is the same for the lymph node and salivary gland. There was also clonal rearrangement of the kappa lightchain gene (Jkappa, Oncor Gaithersburg, MD) and absence of clonal rearrangement of the T-cell receptor beta-chain gene (J/3 1 + 2 probe, Oncor, Gaithersburg, MD). B cells, a phenomenon associated with expression of the protein bcl-2, which plays a role in preventing apoptosis.39 In addition, the EBV genome contains the gene BHRF1, which has sequence homology with the bcl-2 gene and may therefore also inhibit apoptosis, leading to B-cell immortalization.39 Cyclosporin A and EBV may act synergistically to prevent the death of EBV-infected lymphocytes. Cyclosporin A has been reported to induce resistance of EBV-transformed B lymphocytes to immune cytolysis by blocking apoptosis.38 Therefore, although apoptosis may be seen in PTLD, relative suppression of this process may lead to an accumulation of EBV-infected lymphocytes. A similar accumulation of B cells could result from a block in their maturation to plasma cells. Evidence for Vol. 99 • No. 3 272 ANATOMIC PATHOLOGY Review Arth •-^ w as t^ C • 00 o 4-t I/) ITi 0\ X « ft* •"^ « X C3 o 00 1/5 «T) ON X M C « * i w ft. 22k b- BamElW 8.1kb MM ^^flP* wHn BamHlY "JF -,i* FIG. 8. Southern blot autoradiograms indicating the presence of EBV DNA in the lymph node biopsy. The control EBV positive cell lines (Raji, X50-7 and B95.8) are indicated. Left image. Bam HI -digested lymph node DNA from Case 3 probed with the EBV Ba/«HIW fragment. This probe indicates the presence of EBV DNA by hybridizing with the 3.1-kb EBV BamHIW fragment. Cross-hybridization with the 1.8 kb-EBV BamHlY fragment is indicated. Right image.fiamHI-digestedlymph node DNA from Case 3 probed with the Xho\a fragment of EBV that hybridizes with the terminal region of the viral genome. A single band in the patient's sample indicates a monoclonal population of cells containing EBV DNA. the latter mechanism includes the observation that regression of PTLD is accompanied by an apparent B-lymphocyte maturation with concomitant accumulation of plasma cells.1 Step 3 The final step in oncogenesis probably involves the activation of oncogenes or inactivation of tumor suppressor genes. Although translocation and subsequent activation of the c-myc oncogene does not occur as frequently in PTLD as in Burkitt's lymphoma,20 c-myc translocation has been associated with the development of progressive PTLD unresponsive to immunosuppression reduction, i.e., the development of malignant lymphoma.32 Further investigation is required to determine whether other oncogenes or tumor-suppressor genes are involved in the progression of PTLD to unequivocal malignant lymphoma. In summary, PTLD can be considered a defect in the balance between cellular destruction (or maturation) and cellular proliferation. Uncontrolled proliferation of B lymphocytes enhances the likelihood of mutational oncogenesis. TREATMENT Initially PTLD was assumed to be malignant lymphoma, and was treated as such with conventional chemotherapeutic regimens. This approach met with little success.6,8"18 In recent years the emphasis has been on the efficacy of reduction in immunosuppressive therapy.1,8 The success of this strategy indicates that many PTLDs do not represent true neoplasms. Indeed, regression of both polymorphic, polyclonal lesions and monoclonal lesions has been well documented.1 Response to therapy usually is seen within 2 weeks, and may occur within a matter of days.1 In patients with monomorphic and/or monoclonal lesions, some authors recommend that a reduction in immunosuppressive therapy be combined with chemotherapy and/or radiation therapy.1'617 A short trial of reduced immunosuppressive therapy alone, however, is usually acceptable. Patients with tumors localized at presentation or with residual localized A.J.C.P. • March 1993 CRAIG, GULLEY, AND BANKS Posttransplantation Lymphoproliferative Disorders 273 FIG. 9. Polymorphous PTLD. Lymph node section from case 4 displaying a polymorphous infiltrate of lymphoid cells that effaces the architecture. Numerous mitotic figures and areas of necrosis are identified (hematoxylin and eosin, original magnification X250). tumor after a reduction in immunosuppressive therapy may benefit from surgical resection.1,21 With reduced immunosuppressive therapy there is a threat of allograft rejection. Loss of a renal homograft can be managed by dialysis,6 and is therefore preferable to the high mortality associated with uncontrolled PTLD. Such a compromise strategy is not acceptable for patients receiving less expendable homografts (e.g., cardiac or hepatic). Successful treatment of PTLD after orthotopic liver transplantation has been achieved without rejection by using judicious reduction in immunosuppressive therapy.1 The value of antiviral agents in the treatment of PTLD remains controversial. 619,21 In 1982 Hanto and colleagues described a patient with a polyclonal, polymorphic diffuse B-cell hyperplasia who appeared to respond to acyclovir therapy alone.40 Acyclovir administration in this case, however, was simultaneous with reduction in immunosuppressive therapy. Acyclovir acts by preventing viral DNA synthesis, and hence viral replication and shedding.41,42 This antiviral agent has no action against circular, episomal EBV DNA contained within latently infected lymphocytes. Although PTLD is most frequently associated with latent EBV infection, acyclovir may be of value in preventing the ongoing infection of B lymphocytes by virus shed from the oral epithelium. This drug also may inhibit the replication of linear EBV DNA sometimes identified within B lymphocytes containing circular latent viral particles.43 Although the effi- cacy of acyclovir has not been proven, the low incidence of complications associated with its administration has led many groups to advocate its use in combination with reduced immunosuppression. 1 CASE REPORTS Case 1 An 18-year-old man presented in January 1986 with a 2-week history of fever and headaches. On physical examination he was noted to have an enlarged submandibular lymph node. Laboratory investigation revealed a white blood cell count of 20.6 X 109/L with 45% lymphocytes. His symptoms persisted despite antibiotic therapy. A computed tomography scan revealed numerous enlarged thoracic and intraabdominal lymph nodes and splenomegaly. A cervical lymph node biopsy was performed (Figs. 2 and 3). Subsequent serologic studies revealed a positive Mono-latex (Wampole Laboratories, Cranbury, NJ) test. A diagnosis of infectious mononucleosis was made. In situ hybridization studies performed on paraffin-embedded tissue from this case revealed EBV EBER1 small RNA gene expression in approximately 50% of the small and large viable cells. The patient is well 7 years later. This case illustrates some of the histologic changes associated with acute EBV infection in an immunocompetent host. The presence of extensive necrosis with large atypical immunoblasts is not a reliable indicator of neoplastic transformation.* Case 2 A 58-year-old woman received a cadaveric renal transplant in October 1987. The immunosuppression regimen included azathioprine, * This case was kindly provided by Dr. Milka Montiel, University of Texas Health Science Center at San Antonio, Texas. Vol. 99 • No. 3 274 ANATOMIC PATHOLOGY Review Article FIG. 10. Polymorphous mixture of immunoblasts, small cleaved cells, and plasma cells from case 4 (hematoxylin and eosin, original magnification X630). prednisolone, and CsA. Within 2 months fever, diffuse lymphadenopaCase 3 thy, and splenomegaly developed. A lymph node biopsy was perA 44-year-old man received a cadaveric renal transplant in October formed, and revealed a polymorphous PTLD (Fig. 4). Immunohisto1991. The immunosuppressive regimen included azathioprine, CsA, chemical studies performed on paraffin-embedded tissue revealed and prednisolone. On the tenth day after transplantation he also repolyclonal staining for kappa and lambda immunoglobulin light ceived OKT3 for a suspected episode of rejection. Thirty-nine days chains. A diagnosis of polyclonal, polymorphous B-cell hyperplasia later "flulike" symptoms developed. The patient became febrile and was made. The immunosuppression was reduced and acyclovir therapy fullness developed in the neck region. A submandibular gland biopsy commenced. The patient's subsequent course was complicated by Staphylococcus aureus sepsis, bacterial thrombophlebitis, and dissemi- ' and submental lymph node resection were performed, and revealed a monoclonal, polymorphous PTLD (Figs. 5-8). nated intravascular coagulation. She died approximately 80 days after The patient's lymphadenopathy resolved with a reduction in immutransplantation. nosuppression and acyclovir therapy. The renal allograft was rejected. An autopsy examination revealed involvement of the liver, spleen, This case illustrates the problems encountered in defining clonality gastrointestinal tract, bladder, lung, renal allograft, and numerous and the significance of thisfinding.Although paraffin-section immunolymph nodes by a polymorphous lymphoid infiltrate resembling that histochemical studies showed a polyclonal pattern of immunoglobulin seen in the lymph node biopsy. Southern-blot analysis of lymph node light-chain staining, gene-probe analysis identified a clonal population DNA procured at the time of autopsy revealed monoclonal rearrangeof lymphoid cells and a clone of cells containing EBV DNA. This case ment of the immunoglobulin kappa light-chain gene. Autopsy examiis an example of a monoclonal lymphoid proliferation that resolved nation also disclosed a pulmonary, necrotizing granuloma containing with a reduction in immunosuppression.% organisms with an appearance consistent with Hisloplasma capsulation. This case demonstrates the rapid onset of generalized polymorphous PTLD in a renal transplant recipient. Although the initial lymph node Case 4 biopsy was polyclonal by immunophenotype, a genetic probe analysis A 47-year-old man received a renal transplant in October 1991. Imperformed on the autopsy tissue revealed a monoclonal population of munosuppressive therapy included azathioprine, prednisolone, and lymphocytes. In situ hybridization studies revealed EBV EBER RNA CsA. Because of an acute rejection episode the patient also received two in 80% of the cells in this infiltrate. This casefitsthe original concept of courses of OKT3. In January 1992, during the second course of OKT3 EBV-associated posttransplantation lymphoid proliferations with protherapy, the patient developed peripheral and retroperitoneal lymphgression from a polyclonal to a fatal monoclonal disorder. Indicators of adenopathy. Serum protein electrophoresis revealed a monoclonal a poor prognosis include the generalized nature of the disorder and the spike in the gamma region that was characterized as IgM/lambda. A presence of associated pyogenic bacterial and fungal infections.f lymph node biopsy was performed, and revealed a polymorphous PTLD (Figs. 9 and 10). •f This case was kindly provided by Dr. Askar Qalbani, Marian Health Center, Sioux City, Iowa, and Dr. Fred Dick, University of Iowa Medical Center, Iowa City, Iowa. $ This case was kindly provided by Dr. John Metter, Humana Hospital-San Antonio, San Antonio, Texas. AJ.C.P. • March 1993 CRAIG, GULLEY, AND BANKS Posttransplantation Lymphoproliferative Disorders 275 FIG. 11. Immunohistochemical studies performed on paraffin-embedded tissue reveal a predominance of staining with primary antibodies directed against lambda immunoglobulin light chain. Left image. Lambda light chain. Right image. Kappa light chain (original magnification X400). Immunohistochemical studies and genetic-probe analysis performed on the node revealed a monoclonal population of B lymphocytes (Fig. 11). Ten days later the patient underwent a partial small bowel resection for perforation. Examination of sections of the small bowel revealed an abnormal polymorphous infiltrate of immunoblasts and plasma cells. In addition there were mucosal ulceration and fungal organisms suggestive of Candida species. Immunosuppression was reduced, and acyclovir therapy was initiated. Despite rejection of the kidney, the patient's condition improved and the lymphadenopathy resolved. The quantity of the serum monoclonal spike also decreased. This case is an example of PTLD presenting with diffuse lymphadenopathy and perforation of the gastrointestinal tract. Evidence of monoclonality was provided by serum-protein electrophoresis, immunohistochemical staining, and gene-probe analysis performed on the lymph node. Despite these indicators, which were suggestive of a poor prognosis, the patient responded to decreased immunosuppression and acyclovir administration^ CONCLUSION After the original description in 1969 by Penn and associates of the development of malignant lymphoma in five renal transplant recipients,10 dramatic progress has been made in the understanding of the pathogenesis and treatment of PTLDs. These lymphoproliferative disorders have been recognized as being closely related to those occurring in patients with inherited immunodefi- § This case was kindly provided by Dr. John Vago, The Christ Hospital, Cincinnati, Ohio. ciency syndromes24 and in patients with the acquired immunodeficiency syndrome.18 Immunodeficiency-associated lymphoid proliferations share many unusual features, including a predilection for extranodal sites, a varied morphologic appearance, a strong and probably causal association with EBV infection, frequent absence of immunophenotypic or genotypic evidence of monoclonality, and rapid progression with conventional chemotherapy and radiation therapy.20 The most distinctive characteristic of the lymphoid proliferations occurring in transplanted organ recipients is their ability to resolve after diminished immunosuppression.8 It is essential therefore that PTLDs be diagnosed early and treated appropriately. To achieve this, we recommend a simplified morphologic classification of PTLD and an empiric approach to their treatment. In addition to their diagnostic challenge, this fascinating group of iatrogenic disorders may provide insight into the pathogenesis of lymphoid neoplasia in general. REFERENCES 1. Nalesnik MA, Makowka L, Starzl TE. The diagnosis and treatment of posttransplant lymphoproliferative disorders. Curr Prob Surg 1988;25:367-472. 2. First MR. Transplantation in the nineties. Transplantation 1992;53:1-11. 3. Bortin MM, Rimm AA. Increasing utilization of bone marrow transplantation: II. Results of the 1985-1987 survey. Transplantation 1989;48:453-458. Vol. 99 • No. 3 276 ANATOMIC PATHOLOGY Review Article 4. Hanto DW, Frizzera G, Purtilo DT, et al. Clinical spectrum of lymphoproliferative disorders in renal transplant recipients and evidence for the role of Epstein-Barr virus. Cancer Res 1981;41(pt 1):4253-4261. 5. Frizzera G, Hanto DW, Gajl-Peczalska KJ, et al. Polymorphic diffuse B-cell hyperplasias and lymphomas in renal transplant recipients. Cancer Res 1981;41(pt l):4262-4279. 6. Hanto DW, Gajl-Peczalska KJ, Frizzera G, et al. Epstein-Barr virus(EBV) induced polyclonal and monoclonal B-cell lymphoproliferative diseases occurring after renal transplantation: Clinical, pathologic, and virologicfindingsand implications for therapy. Ann Surg 1983; 198:356-369. 7. Penn I. Cancers following cyclosporine therapy. Transplantation Proc 1987; 19(pt 3):2211 -2213. 8. Starzl TE, Nalesnik MA, Porter KA, et al. Reversibility of lymphomas and lymphoproliferative lesions developing under cyclosporin-steroid therapy. Lancet. 1984;1:583-587. 9. Murray JE, Wilson RE, Tilney NL, et al. Five years' experience in renal transplantation with immunosuppressive drugs: Survival, function, complications, and the role of lymphocyte depletion by thoracic duct fistula. Ann Surg 1968; 168:416-435. 10. Penn I, Hammond W, Brettschneider L, Starzl TE. Malignant lymphomas in transplantation patients. Transplantation Proc 1969;1:106-112. 11. Penn I, First MR. Development and incidence of cancer following cyclosporine therapy. Transplantation Proc 1986; 18(Suppl 1):210-215. 12. Matas AJ, Hertel BF, Rosai J, Simmons RL, Najarian JS. Posttransplant malignant lymphoma: Distinctive morphologic features related to its pathogenesis. Am J Med 1976;61:716-720. 13. Castro CJ, KJimo P, Worth A. Multifocal aggressive lymphoma of the gastrointestinal tract in a renal transplant patient treated with cyclosporin A and prednisone. Cancer 1985;55:1665— 1667. 14. Klein G, Purtilo D. Summary: Symposium on Epstein-Barr virusinduced lymphoproliferative diseases in immunodeficient patients. Cancer Res 198 l;41(pt l):4302-4304. 15. Geary ML, Warnke R, Sklar J. Monoclonality of lymphoproliferative lesions in cardiac-transplant recipients: Clonal analysis based on immunoglobulin-gene rearrangements. N Engl J Med 1984;310:477-482. 16. Geary ML, Sklar J. Lymphoproliferative disorders in cardiac transplant recipients are multiclonal lymphomas. Lancet 1984;2:489-493. 17. Hanto DW, Birkenbach M, Frizzera G, et al. Confirmation of the heterogeneity of posttransplant Epstein-Barr virus-associated B cell proliferations by immunoglobulin gene rearrangement analyses. Transplantation 1989;47:458-464. 18. List AF, Greco FA, Vogler LB. Lymphoproliferative diseases in immunocompromised hosts: the role of Epstein-Barr virus. J Clin Oncol 1987;5:1673-1689. 19. Hanto DW, Frizzera G, Gajl-Peczalska KJ, Simmons RL. EpsteinBarr virus, immunodeficiency, and B cell lymphoproliferation. Transplantation 1985;39:461-472. 20. Brusamolino E, Pagnucco G, Bernasconi C. Secondary lymphomas: A review on lymphoproliferative diseases arising in immunocompromised hosts. Prevalence, clinical features and pathogenetic mechanisms. Haematologica 1989;74:605-622. 21. Cohen JI. Epstein-Barr virus lymphoproliferative disease associated with acquired immunodeficiency. Medicine. 1991; 70:137-160. 22. Linder J, Purtilo DT. Current concepts of immunodeficiency disorders. Mod Pathol 1990;3:524-544. 23. Biemer JJ. Malignant lymphomas associated with immunodeficiency states. Ann Clin Lab Sci 1990; 20:175-191. 24. Bird AG, Britton S. The relationship between Epstein-Barr virus and lymphoma. Semin Hematol 1982; 19:285-300. 25. Zutter MM, Martin PJ, Sale GE, et al. Epstein-Barr virus lymphoproliferation after bone marrow transplantation. Blood 1988;72:520-529. 26. McCune JM. Epstein-Barr virus associated lymphoproliferative disease in mice and men. Lab Invest 1991;65:377-380. 27. Swinnen LJ, Costanzo-Nordin MR, Fisher SG, et al. Increased incidence of lymphoproliferative disorder afterimmunosuppression with the monoclonal antibody OKT3 in cardiac-transplant recipients. N Engl J Med 1990;323:1723-1728. 28. Starzl TE, Klintmal GB, Weil R, et al. Cyclosporin A and steroid therapy in sixty-six cadaver kidney recipients. Surg Gynecol Obstet 1981;153:486-494. 29. Randhawa PS, Yousem SA, Paradis 1L, et al. The clinical spectrum, pathology, and clonal analysis of Epstein-Barr virus-associated lymphoproliferative disorders in heart-lung transplant recipients. Am J Clin Pathol 1989;92:177-185. 30. Frizzera G. The clinico-pathological expressions of Epstein-Barr virus infection in lymphoid tissues. Virchows Archiv Cell Pathol 1987;53:1-12. 31. Siegelman MH, Geary ML, Warnke R, Sklar J. Frequent biclonality and Ig gene alterations among B cell lymphomas that show multiple histologic forms. J Exp Med 1985; 161:850-863. 32. Locker J, Nalesnik M. Molecular genetic analysis of lymphoid tumors arising after organ transplantation. Am J Pathol 1989;135:977-987. 33. Willis RA. Pathology of Tumours. St. Louis: C.V. Mosby, 1948, pi. 34. Brown NA, Liu C, Garcia CR, et al. Clonal origins of lymphoproliferative disease induced by Epstein-Barr virus. J Virol 1986;58:975-978. 35. Wang F, Gregory C, Sample C, et al. Epstein-Barr virus latent membrane protein (LMP1) and nuclear proteins 2 and 3C are effectors of phenotypic changes in B lymphocytes: EBNA-2 and LMP1 cooperatively induce CD23. J Virol 1990;64:2309-2318. 36. Young L, Alfieri C, Hennessy K, et al. Expression of Epstein-Barr virus transformation-associated genes in tissues of patients with EBV lymphoproliferative disease. N Engl J Med 1989; 321:1080-1085. 37. Burnet FM. The concept of immunological surveillance. Progr Exp Tumor Res 1970;13:1-27. 38. Hudnall SD. Cyclosporin A renders target cells resistant to immune cytolysis. Eur J Immunol 1991;21:221-226. 39. Williams GT. Programmed cell death: Apoptosis and oncogenesis. Cell 1991;65:1097-1098. 40. Hanto DW, Frizzera, Gajl-Peczalska KJ, et al. Epstein-Barr virusinduced B-cell lymphoma after renal transplantation: Acyclovir therapy and transition from polyclonal to monoclonal B-cell proliferation. New Engl J Med 1982;306:913-918. 41. Colby BM, Shaw JE, Elion GB, Pagano JS. Effect of acyclovir [9-(2-hydroxyethoxymethyl)guanine] on Epstein-Barr virus DNA replication. J Virol 1980;34:560-568. 42. Andersson J, Ernberg I. Management of Epstein-Barr virus infections. Am J Med 1988;85:107-115. 43. Katz BZ, Raab-Traub N, Miller G. Latent and replicating forms of Epstein-Barr Virus DNA in lymphomas and lymphoproliferative diseases. J Infect Dis 1989; 160:589-598. 44. Raab-Traub N, Flynn K. The structure of the termini of the Epstein-Barr virus as a marker of clonal cellular proliferation. Cell 1986;47:883-889. A.J.C.P. • March 1993