Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
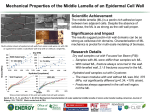
© 2014. Published by The Company of Biologists Ltd | Development (2014) 141, 807-815 doi:10.1242/dev.102699 RESEARCH ARTICLE STEM CELLS AND REGENERATION Human embryonic epidermis contains a diverse Langerhans cell precursor pool Christopher Schuster1, Michael Mildner2, Mario Mairhofer3, Wolfgang Bauer1, Christian Fiala4, Marion Prior1, Wolfgang Eppel3, Andrea Kolbus3, Erwin Tschachler2, Georg Stingl1 and Adelheid Elbe-Bürger1,* KEY WORDS: Langerhans cell, Precursor, Development, Skin, Skin equivalent INTRODUCTION Langerhans cells (LCs) are antigen-presenting cells (APCs) that play important roles as immune sentinels in skin (Romani et al., 2012a). During human skin development, their precursors are first identified in the epidermis at 7-9 weeks estimated gestational age (EGA), based on the expression of CD45 (PTPRC – HGNC), HLA-DR, CD1c and ATPase (Foster et al., 1986; Fujita et al., 1991; Schuster et al., 2009). The distinguishing features of LCs in adult human epidermis, namely Birbeck granules, CD207/langerin, and CD1a are detectable only after 11 weeks EGA (Foster et al., 1986; Schuster et 1 Department of Dermatology, Division of Immunology, Allergy and Infectious Diseases (DIAID), Laboratory of Cellular and Molecular Immunobiology of the Skin, Medical University of Vienna, Vienna, Austria. 2Department of Dermatology, Research Division of Biology and Pathobiology of the Skin, Medical University of Vienna, Vienna, Austria. 3Department of Obstetrics and Gynaecology, Medical University of Vienna, Vienna, Austria. 4Gynmed-Ambulatorium, Vienna, Austria. *Author for correspondence ([email protected]) This is an Open Access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/3.0), which permits unrestricted use, distribution and reproduction in any medium provided that the original work is properly attributed. Received 16 August 2013; Accepted 10 December 2013 al., 2009). Our observation that not all HLA-DR-positive (HLADR+) epidermal cells in embryonic human skin express the LC markers CD1a, CD1c or CD207/langerin, prompted us to hypothesize that during ontogeny the LC phenotype is acquired in the epidermis (Schuster et al., 2009), a notion that was recently validated in the murine system (Seré et al., 2012). Owing to this stepwise development of the LC phenotype, it is conceivable that other molecular structures required for the initiation of immune responses including MHC-II molecules (e.g. HLA-DR) may also be acquired in the epidermis. Thus, by looking at early stages of development the original phenotype of LC precursors could be unravelled. Indeed, an earlier study identified dendritic or round epidermal cells in the first trimester that expressed the scavenger receptor CD36 (Fujita et al., 1991). Concomitant with HLA-DR+ epidermal cells becoming more frequent, CD36+ cells in the human epidermis decrease in numbers and are – as in healthy adult skin – not detectable at the end of the first trimester. Their origin, precise phenotype and ultimate fate have yet to be elucidated. At 7 weeks EGA, the earliest time point where epidermal LC precursors have been identified (Foster et al., 1986), haematopoiesis in humans is active in the yolk sac, the aorta-gonad-mesonephros region and the foetal liver, representing potential sites of origin for these precursors, but inactive in the bone marrow (Tavian and Péault, 2005). Although local proliferation has been described in epidermal leukocytes during the first trimester (Schuster et al., 2009), the type(s) of progenitors that colonize the epidermis and their relationship to haematopoietic stem cells remain unknown. The aim of this study was to further characterize the phenotype of LC precursors in first trimester human epidermis, in particular to analyse co-expression of HLA-DR with various molecules often thought to be present on LC precursors such as CD14, CD36 and CD45, thereby broadening our knowledge about their ontogeny in vivo. Moreover, to extend and confirm our in vivo observations we used a human three-dimensional full-thickness skin model that evaluated the LC differentiation potential of various cord blood- or peripheral blood-derived cells phenotypically resembling the precursor cells found during ontogeny. RESULTS Human embryonic skin harbours leukocytes with distinct phenotypes In healthy adult human skin, CD36 is found on a multitude of cells including immune cells such as dermal dendritic cells and macrophages as well as non-immune cells including endothelial cells and melanocytes (Foster, 1993). To explore the expression of CD45+CD36+ cells in developing human skin, we compared whole prenatal with adult skin cell suspensions (Fig. 1A). Using flow cytometry, we found CD45+CD36+ cells in first trimester skin, though at lower frequencies than in adult skin (0.71±0.33%, n=8 versus 4.06±1.56%, n=6; P=0.003; Fig. 1C). However, 807 Development ABSTRACT Despite intense efforts, the exact phenotype of the epidermal Langerhans cell (LC) precursors during human ontogeny has not been determined yet. These elusive precursors are believed to migrate into the embryonic skin and to express primitive surface markers, including CD36, but not typical LC markers such as CD1a, CD1c and CD207. The aim of this study was to further characterize the phenotype of LC precursors in human embryonic epidermis and to compare it with that of LCs in healthy adult skin. We found that epidermal leukocytes in first trimester human skin are negative for CD34 and heterogeneous with regard to the expression of CD1c, CD14 and CD36, thus contrasting the phenotypic uniformity of epidermal LCs in adult skin. These data indicate that LC precursors colonize the developing epidermis in an undifferentiated state, where they acquire the definitive LC marker profile with time. Using a human three-dimensional full-thickness skin model to mimic in vivo LC development, we found that FACS-sorted, CD207– cord bloodderived haematopoietic precursor cells resembling foetal LC precursors but not CD14+CD16– blood monocytes integrate into skin equivalents, and without additional exogenous cytokines give rise to cells that morphologically and phenotypically resemble LCs. Overall, it appears that CD14– haematopoietic precursors possess a much higher differentiation potential than CD14+ precursor cells. RESEARCH ARTICLE Development (2014) doi:10.1242/dev.102699 CD45–CD36+ cells were significantly more frequent in first trimester than adult skin (20.06±5.93%, n=8 versus 2.14% ± 1.17, n=6; P<0.001). These cells most likely represent undifferentiated mesenchymal, endothelial and periderm cells. Unexpectedly, we also observed that the relative expression of the monocyte marker CD14 on CD36+ leukocytes did not differ significantly between prenatal and adult skin (Fig. 1A,B, upper panel). Strikingly, significantly fewer CD45+CD36+ cells in prenatal skin expressed HLA-DR compared with adult skin (Fig. 1A,B, lower panel). Expression of CD14 on CD45+CD36– and CD45–CD36+ cells between the first trimester and adult skin was comparable, whereas HLA-DR was found significantly less frequently. The notion that first trimester skin is devoid of HLA-DR, an indicator of antigen-presenting capacity, was corroborated by the fact that in first trimester skin CD36+ leukocytes outnumbered HLA-DR+ as well as CD14+ leukocytes (Fig. 1C). By contrast, HLA-DR+ leukocytes were significantly more frequent than CD36- or CD14-expressing cells in adult skin (Fig. 1C). Fig. 1. CD45+CD36+ cells are the predominant leukocyte population in human prenatal skin. (A) Multiparameter flow cytometry of freshly isolated single cell suspensions of prenatal and adult human skin was performed by incubation with monoclonal antibodies against the cell surface markers indicated (n=5). Gates in dot plots were set according to isotype-matched control staining. Dead cells (based on 7-AAD uptake) were excluded. Histograms show CD14 and HLA-DR expression of indicated regions (black line; grey line, isotype control). (B) Dot graphs of the percentage expression of CD14 and HLA-DR in CD45+CD36+ (R1), CD45+CD36– (R2) and CD45–CD36+ (R3) cells. Bars indicate the mean of investigated groups. (C) Flow cytometric analysis of the percentage of HLA-DR-, CD14- and CD36-expressing cells relative to total skin cells. Empty symbols represent adult skin, filled symbols prenatal (9-14 weeks EGA) skin. 808 To further characterize the phenotype and the localization of CD36+ cells in prenatal skin, triple immunofluorescence staining was performed on cryostat sections. As the moderate thickness of the embryonic epidermis precludes the enzymatic separation from the underlying dermis (and consequently a comparative assessment of epidermal and dermal subsets by flow cytometry), immunofluorescence remains the only technique available to study the compartmental distribution of epidermal leukocyte subsets. We found that epidermal CD36+ cells are primarily round or moderately dendritic in shape (Fig. 2A, arrowhead) and always co-express the haematopoietic cell marker CD45+, thus confirming and extending previous findings (Fujita et al., 1991). The frequency of CD45+ epidermal cells between 9-11 and 12-14 weeks EGA did not differ but was significantly lower than in adult skin (Fig. 2B). CD45+CD36+ epidermal cells could be readily identified up to the end of the first trimester but not beyond 18 weeks EGA. CD45+ epidermal cells in first trimester human skin displayed striking surface marker heterogeneity. Of note, at 9-11 weeks EGA, significantly fewer CD45+ epidermal cells stained for HLA-DR than at 12-14 weeks EGA, confirming our flow cytometric data of HLADR depletion also for the epidermal leukocyte compartment (Fig. 2C, left). When HLA-DR expression became more pronounced on epidermal leukocytes, the frequency of CD45+CD36+ cells concomitantly declined (Fig. 2C, middle), although CD36 expression was occasionally found until the end of the first trimester. Surprisingly, a small percentage of CD45+ epidermal cells expressed neither CD36 nor HLA-DR (Fig. 2A, double arrow and inset; Fig. 2C, right graph). Owing to the broad expression of CD36 on haematopoietic cells (e.g. myeloid precursor cells and their progeny, red blood cells, monocytes, dendritic cells) and non-haematopoietic cells (e.g. keratinocytes under inflammatory conditions, a subset of melanocytes), it was not possible to determine whether it was associated with one specific cell type more than the others. To better define the phenotype of embryonic CD36+ skin cells and in particular CD36+ epidermal cells, we performed co-immunostaining experiments with other markers. Similar to the distribution of CD36, CD14 was predominately expressed on mainly round dermal cells and occasionally in the epidermis (Fig. 3A; supplementary material Fig. S1). In contrast to CD36, CD14 was exclusively found on CD45+ cells and appeared to become less frequent on epidermal Development CD45+CD36+ cells are the predominant leukocyte population in human embryonic epidermis RESEARCH ARTICLE Development (2014) doi:10.1242/dev.102699 Fig. 2. Human embryonic epidermis contains various leukocyte subsets with regard to CD36 and HLA-DR expression. (A) Immunofluorescence triple labelling identified CD45+CD36+HLA-DR+ (arrowhead), CD45+CD36–HLA-DR+ (arrow) and CD45+CD36–HLA-DR– (double arrow) epidermal cells in first trimester human skin. LCs in healthy adult skin do not express CD36. Alexa Fluor 488labelled laminin 5 monoclonal antibody visualizes the dermo-epidermal junction. (B) Dot graph of the increase of CD45+ epidermal cells/linear centimetre of epidermis. Bars indicate the mean of the investigated groups. (C) The percentages of the indicated surface molecules among total CD45+ epidermal cells. Bars indicate the mean of investigated groups. Scale bars: 50 μm. arrowhead, middle panel), the nature of which remains to be determined but perhaps they are macrophages, dendritic cells or mast cell precursors (Tavian and Péault, 2005). We discovered that some epidermal leukocytes in first trimester human skin did not express any commonly used monocyte or dendritic cell marker and could only be identified as haematopoietic cells on the basis of their staining for CD45. In addition, they did not express CD34 but partially expressed markers found on monocytes, namely CD14, CD36 and HLA-DR. Cord blood cells with phenotypes resembling embryonic resident epidermal leukocytes develop into CD207+ LCs in a human skin equivalent model Human skin equivalents are a highly valuable tool to study the origin and development of LCs, given that potential precursors can be mixed with keratinocytes and allowed to integrate in the differentiating epithelium. These skin equivalents are generated with primary human keratinocytes and fibroblasts that are seeded into a collagen matrix. Lifting of keratinocytes to the air-liquid surface induces terminal differentiation, resulting in a stratified and cornified epidermis (Fig. 4A) (Mildner et al., 2010). In such a model, LC 809 Development leukocytes towards the end of the first trimester (Fig. 3B). Similar to HLA-DR expression on CD36+ cells, CD14 was observed on both CD45+CD36+ and CD45+CD36– cells (data not shown). CD45+ epidermal cells expressing neither CD36 nor CD14 were also found (Fig. 3A, double arrow; supplementary material Fig. S1). Of note, the dendritic cell marker CD1c also showed this diversity of expression (Fig. 3C, arrow and arrowhead; supplementary material Fig. S2, arrow and arrowhead). Given that CD14 and CD36 can also be detected on early CD34+ myeloid precursor cells (Thoma et al., 1994), we then analysed whether epidermal leukocytes express the haematopoietic stem cell marker CD34. No co-expression of CD34 and CD45 was detectable in the epidermis at any time point investigated (Fig. 3D, arrow; supplementary material Fig. S3, arrow), whereas CD34 was evident on dermal vessels in first trimester human skin (Fig. 3D, arrowhead; supplementary material Fig. S3, arrowhead). Intriguingly, CD45+CD34+ dermal cells were rarely detectable and located predominantly within vessels (Fig. 3D, arrowhead; supplementary material Fig. S3, arrowhead). Solitary CD45+CD34+ cells were present at a very low frequency in the developing dermis (Fig. 3D, arrowhead, middle panel; supplementary material Fig. S3, RESEARCH ARTICLE Development (2014) doi:10.1242/dev.102699 precursors should ideally develop from precursors without additional exogenous cytokines because all important stimuli are supposed to be provided by the artificial epidermis and dermis. To examine this, skin equivalents were tested for the production of key cytokines required for LC development, such as TGFβ1 (Borkowski et al., 1996; Geissmann et al., 1998; Kaplan et al., 2007; Strobl et al., 1996), GM-CSF (Geissmann et al., 1998; van de Laar et al., 2012) and the evolutionarily highly conserved IL-34 (IL-34 – HGNC) (Greter et al., 2012; Wang et al., 2012). Using immunohistochemistry, we found that skin equivalents express high levels of TGFβ1, although in a different pattern compared with adult skin. In healthy adult skin, TGFβ1 is located exclusively suprabasally (Schuster et al., 2009), whereas in skin equivalents TGFβ1 is also expressed in cells of the basal layer. Interestingly, the basal layer showed varied expression, perhaps reflecting stratification of pre-existing cells in the formation of the epidermis of the skin equivalent rather than development through proliferation attained in normal skin. Moreover, TGFβ1high keratinocytes are scattered throughout the whole epidermis (Fig. 4A, inset, arrows). When analysing supernatants and lysates with ELISA, all three cytokines can be detected in skin equivalents (Fig. 4B). Kinetic experiments during days 1-8 revealed that the levels of TGFβ1 in the supernatants remain constant throughout the whole observation period, whereas its total amount in epidermal lysates gradually increased until day 5 and then decreased (Fig. 4B, upper and lower panel). The GM-CSF level in supernatants steadily increased until day 5 but thereafter reduced, so that on day 8 the level was the same as at day 3. IL-34 was not detectable in supernatants but showed constant levels in the lysates. Taken together, these data show that skin equivalents are endowed with the molecular prerequisites to promote the development of LC. 810 Next, we tested the differentiation capacity of LC precursor candidates in skin equivalents. For this purpose, CD34+ cord bloodderived cells obtained by fluorescence-activated cell sorting (FACS) were cultured (Caux et al., 1992; Strobl et al., 1996). After 10 days, specific subsets (e.g. CD1a+CD14–, CD1a–CD14–, CD1a–CD14+), and in parallel CD14+CD16– blood monocytes, were analysed (Fig. 4C) and sorted to high purity (Fig. 5C). Basically, these populations lacked the expression of the LC marker CD207 and variably expressed CD36. Although almost all CD1a+CD14– and CD1a–CD14+ cells co-express CD36, this marker is only found on a subset of CD1a–CD14– haematopoietic precursors. All populations expressed the pan-leukocyte marker CD45, the myeloid cell marker CD33 and to a varying degree HLA-DR. CD34 had been lost in all populations, whereas a small CD117+ population was identified exclusively in the CD1a–CD14– subset, most probably representing mast cells. The dendritic cell marker CD1c was only detectable on CD1a+CD14– cells. CD14+CD16– monocytes invariably expressed CD36 and HLA-DR and lacked expression of the dendritic cell markers CD1a, CD1c and CD207. Cord blood-derived subsets, as shown in Fig. 5A, were co-cultured with keratinocytes for 8 days and equivalents were then analysed by immunohistochemistry (Fig. 5B). Unexpectedly, all cord blood-derived precursor subsets gave rise to CD1a+ and CD207+ LC in skin equivalents (Fig. 5C). These cells were dendritic in shape and principally evenly distributed with occasional clusters. Although the difference of integrated CD1a or CD207 cells within one cord blood sample was rather low, a high specimen-specific variability in cell number was observed (Fig. 4D). CD1a+CD14– and CD1a–CD14– cells had a higher differentiation potential than CD1a–CD14+ cells (Fig. 4D) to develop into CD1a+ or CD207+ dendritic cells. Although CD207+ cells slightly outnumbered CD1a+ cells in most samples, the difference was not Development Fig. 3. Human embryonic epidermis contains leukocytes with distinct phenotypes. (A,C) Immunofluorescence triple labelling identified (A) CD45+CD36+CD14+ (arrowhead) and CD45+CD36–CD14– (double arrow) as well as (C) CD45+CD36+CD1c+ (arrow) and CD45+CD36–CD1c+ (arrowhead) epidermal cells in first trimester human skin. (B) Dot graph of the percentage of CD14+ leukocytes relative to all epidermal CD45+ cells. Bars indicate the mean of investigated groups. Scale bars: 50 μm. (D) Immunofluorescence double labelling identified solitary (middle; arrowhead) and vessel-associated (right; inset, arrowhead) CD45+CD34+ dermal cells. Epidermal leukocytes do not express CD34 (left; arrow). Scale bars: 50 μm. RESEARCH ARTICLE Development (2014) doi:10.1242/dev.102699 statistically significant. CD14+CD16– blood monocytes never matured into LCs under these conditions (Fig. 5C,D). DISCUSSION This study, which focused on the development of epidermal leukocytes in the first trimester, showed that human epidermis contains a multitude of phenotypically distinct LC precursors, in contrast to the uniformity of LCs in adult skin. Using a human threedimensional full-thickness skin model, we also found that cord blood-derived CD14+ progenitor cells possess the potential to give rise to CD207+ LCs (Schaerli et al., 2005), although to a significantly lesser extent than CD1a+CD14– and CD1a–CD14– progenitors under similar conditions. LC precursors in human first trimester skin are heterogeneous HLA-DR+ leukocytes in embryonic epidermis can be subdivided according to the expression of the scavenger receptor CD36, as has been described previously (Fujita et al., 1991). Interestingly, we found that 23.8% of epidermal leukocytes between 9 and 11 weeks EGA express neither CD36 nor HLA-DR and that HLA-DR expression on CD45+ cells roughly equals expression of CD36, thus confirming and extending previous results (Fujita et al., 1991). In short, these epidermal leukocytes are CD45+CD36+HLA-DR+, CD45+CD36–HLA-DR+ or CD45+CD36+HLA-DR–, CD45+CD36–HLA-DR–. At the end of the first trimester, HLA-DR becomes dominant whereas CD36 expression abates and cannot be found at later stages of development. CD14 on epidermal leukocytes is found less frequently than CD36, yet it is almost invariably coexpressed with CD36. Like CD36, CD14 is also not detectable on epidermal cells after 18 weeks EGA. It should be emphasized that the lower frequency of CD14+ compared with CD36+ epidermal cells could be explained by the intricate detection of CD14 by immunofluorescence. In mice, it has been shown that during skin inflammation Gr1+ monocytes can give rise to epidermal LCs (Ginhoux et al., 2006). CD36 and CD14 are also found on a subset 811 Development Fig. 4. Skin equivalents fulfil the requirements for LC development. (A) Immunohistochemical staining was performed on cryostat sections of skin equivalents at day 8. TGFβ1 is found throughout the epidermis with occasional cells expressing it at high levels (inset, arrows). Data are representative of five experiments. Scale bar: 50 μm. (B) TGFβ1, GM-CSF and IL-34 levels were analysed in cell culture supernatants of skin equivalents or lysed epidermal equivalents at the indicated time points. Values are means ± s.d. of three experiments. (C) Multiparameter flow cytometry of propagated and cultured CD34+ cord blood-derived haematopoietic stem cells and blood monocytes was performed by incubation with monoclonal antibodies against the cell surface markers indicated (black line, indicated antibody; grey line, isotype control). Gates in dot plots were set according to isotype-matched control staining. Dead cells (based on 7-AAD uptake) were excluded. RESEARCH ARTICLE Development (2014) doi:10.1242/dev.102699 of human blood monocytes (Zamora et al., 2012), hence it cannot be excluded that these cells represent monocytic LC precursors. Of note, a subset of CD45+CD36+ LC precursors in first trimester epidermis expresses CD1c, indicating that committed dendritic cells can also co-express CD36 (Schuster et al., 2009). The lack of CD34 on epidermal leukocytes suggests that the initial precursor does not have haematopoietic stem cell potential. Given that the expression of CD34 is highest on uncommitted stem cells and is increasingly lost as the progenitors differentiate, it cannot be excluded that these epidermal leukocytes in first trimester skin show low-level expression of CD34, which is not detectable using immunofluorescence (Ordóñez, 2012). Owing to the lack of appropriate immunohistochemical markers for different differentiation stages of the progeny of haematopoietic stem cells, it is, at present, not possible to investigate whether these early precursors possess at least some regenerative potential. However, we and others have previously shown that leukocytes in developing mouse and human skin show a higher proliferation capacity than 812 those in adult skin (Chang-Rodriguez et al., 2005; Schuster et al., 2009; Chorro et al., 2009). The phenotypic heterogeneity of LC precursors during skin development results from the presence and absence of molecules representative of LCs in healthy adult skin. The principal cause of this diversity remains unexplained to date and different scenarios, or a combination thereof, are possible: (1) gain and/or loss of antigens, (2) asynchronous maturation of precursors, or (3) colonization by different precursor cells. In humans, blood formation starts in the yolk sac, and later shifts to the aorta-gonad-mesonephros region, the foetal liver, and finally, around 11 weeks EGA, to the bone marrow (Péault and Tavian, 2003). It is possible that LC precursors differ depending on their origin (Hoeffel et al., 2012). Evidence for this comes from the most recent fate-mapping experiments in mice showing that the primitive epidermis is colonized by a first wave of yolk sac-derived precursors and macrophages (Hoeffel et al., 2012). Subsequently, these early precursors are largely replaced by precursors that originate in the foetal liver. Based on these data we Development Fig. 5. Cord blood-derived cells develop into CD207+ LCs in a human skin equivalent model. (A) Representative dot plot of FACS-sorted haematopoietic precursors and blood monocytes (n=6). (B) Schematic view of LC development from cord blood-derived precursors or blood monocytes in skin equivalents composed of primary human keratinocytes and fibroblasts in a collagen matrix. (C) Immunohistochemical analysis of CD1a and CD207 expression in the epidermis of a skin equivalent at day 8. Primary antibodies were detected using secondary horse anti-mouse biotin-conjugated antibodies, followed by incubation with streptavidin-HRP. Staining was visualized by AEC. Scale bars: 50 μm. (D) Statistical analyses of CD1a+ and CD207+ cell frequency in the indicated populations; data are from six independent experiments. RESEARCH ARTICLE CD207– precursors integrate in artificial skin To directly test whether CD14+CD36+ epidermal leukocytes give rise to LCs, we used a human three-dimensional full-thickness skin model (Mildner et al., 2010) and studied the integration of distinct precursor cells in the newly forming epidermis. To date, only a few groups have been able to achieve integration of LC precursors or LCs into skin equivalents (Bechetoille et al., 2007; Hubert et al., 2005; Laubach et al., 2011; Ouwehand et al., 2011; Régnier et al., 1997; Schaerli et al., 2005). To our knowledge, we are the first to have succeeded in comparatively assessing the differentiation capacity of distinct progenitor subsets using artificial skin. Our finding that cord blood-derived precursor cells but not CD14+CD16– monocytes from peripheral blood were able to mature into CD1a+CD207+ LCs might indicate that CD36+ or CD14+ leukocytes in first trimester human epidermis are not monocytes but phenotypically similar precursors or progenitors (Ziegler-Heitbrock et al., 2010). Of note, although various functional differences between foetal or neonatal and adult monocytes have been described (Adkins et al., 2004; Fadel and Sarzotti, 2000; Levy, 2005), it is still unknown whether monocytes possess a higher differentiation capacity during the first trimester than in adult life. Surprisingly, CD1a+ precursors, which are generally regarded to be dendritic cells, do not possess a higher potential than CD1a–CD14– haematopoietic precursors. It is conceivable that – as has been postulated by various in vitro studies – CD14+ cord-blood derived precursors represent an intermediate stage between CD34+ haematopoietic stem cells and CD1a+ precursors (Caux et al., 1992; Jaksits et al., 1999). Of note, CD36 is found to a varying degree on all these cord blood-derived subsets as well as on CD14+ monocytes. Therefore, in contrast to CD14, CD36 cannot be used to further define the phenotype of potential LC precursors. Similarities between LC development in mice and humans The development of LCs in mice and humans differs in various aspects, exemplified by the postnatal acquisition of MHC class II and subsequently langerin in mice (Chorro et al., 2009; Elbe et al., 1989; Romani et al., 1986; Tripp et al., 2004). In humans, by contrast, 54.2% of epidermal leukocytes express HLA-DR by 11 weeks EGA. This percentage increases in utero to 88.0% after 12 weeks EGA. Although the chronological developmental steps of LC precursors in mice and humans differ (Chorro and Geissmann, 2010; Elbe-Bürger and Schuster, 2010; Ginhoux and Merad, 2010), recent experiments reveal amazing similarities. After injection of wild-type bone marrow into IdD2–/– mice entirely lacking LCs, an LC network was generated over a period of 3 weeks (Romani et al., 2012b; Seré et al., 2012). Intriguingly, CD45+ and less numerous HLA-DR+ LC precursors were present 1 week after bone marrow transplantation, whereas prominent CD11c and CD207 expression was not seen until 2-3 weeks. Thus, the sequential acquisition of surface markers not only resembled the murine but also human ontogeny and corroborates the notion that CD45+ precursors colonized the epidermis, where they sequentially acquire their phenotype. Given that: (1) T cells are not present in prenatal skin before 18 weeks EGA (Di Nuzzo et al., 2009; Schuster et al., 2012); (2) no other immune cells exist with a tropism for the epidermis; and (3) apoptosis is not detectable in first trimester epidermal leukocytes, we assume that CD45+CD36–HLA-DR– cells in embryonic skin are LC precursors. CD45+HLA-DR– cells were also identified in the epidermis of healthy adult skin, but these cells most probably are lymphocytes as previously reported (Foster and Elbe, 1997). We identified phenotypically heterogeneous LC precursors in human embryonic epidermis, whereas leukocytes resembling phenotypically adult LC can only be found by the end of the second trimester. Together with our finding that defined cord blood-derived subsets, phenotypically similar to those described in embryonic epidermis, can give rise to LCs in a human three-dimensional fullthickness skin model, our data are an important step in our understanding of LC biology in human skin. MATERIALS AND METHODS Skin samples After legal termination of pregnancy, 42 specimens of human embryonic (914 weeks EGA, first trimester) and foetal (18-24 weeks EGA) trunk skin were studied. The age was estimated by crown-rump length and maternal history. Healthy adult skin was collected after plastic surgery. The study was approved by the local ethics committee of the Medical University of Vienna and conducted in accordance with the declaration of Helsinki Principles. Parents or participants gave their written informed consent. Preparation of skin cell suspensions Prenatal and adult skin was incubated on 1.2 U/ml Dispase II (Roche Diagnostics, Indianapolis, IN) in PBS overnight at 4°C. Because it was impossible to efficiently separate dermis and epidermis in embryonic skin, unseparated skin, regardless of age, was vigorously agitated in a shaking bath in 0.53 U/ml Liberase 3 (Roche Diagnostics) in PBS at 37°C for 60-90 minutes. The resulting single-cell suspensions were washed with RPMI 1640 medium (Life Technologies) supplemented with 10% heat-inactivated FCS (PromoCell, Heidelberg, Germany), 25 mM HEPES, 10 μg/ml gentamicin, 2 mM L-glutamine, 0.1 mM non-essential amino acids, 1 mM sodium pyruvate, 50 μM 2-mercaptoethanol and 0.002% antibioticantimycotic solution (all Invitrogen) and analysed by flow cytometry. Generation of cord blood-derived CD34+ haematopoietic precursors and isolation of CD14+ blood monocytes Samples of cord blood from healthy human donors were collected from fullterm deliveries. The collection was approved by the local ethics committee and conducted in accordance with the declaration of Helsinki Principles. Mononuclear cells were isolated as described and stored in liquid nitrogen (Mairhofer et al., 2013). After thawing, CD34+ haematopoietic precursors were separated from cord blood mononuclear cells by positive immunoselection (CD34+ MicroBead Kit; Miltenyi Biotec GmbH, Bergisch Gladbach, Germany) and the number of isolated, viable CD34+ cells was determined using a modified ISHAGE gating strategy (Mairhofer et al., 2013). Dead cells were excluded with 7-AAD (BD Biosciences). The staining protocol was calibrated with the BD Stem Cell Control Kit (BD Biosciences). Isolated CD34+ haematopoietic precursors were cultured for 3 days under expansion conditions before being induced to differentiate into CD14+ and CD1a+ cells (Caux et al., 1996; Jaksits et al., 1999; Strobl et al., 1996). Briefly, CD34+ haematopoietic precursors were expanded using XVivo 15 (Lonza, Basel, Switzerland) containing penicillin (100 U/l), and streptomycin (100 μg/ml) and supplemented with thrombopoetin (50 ng/ml), SCF (50 ng/ml) and Flt3L (50 ng/ml; all Peprotech, Rocky Hill, NJ) for 3 days. Subsequently, cells were differentiated using the above mentioned medium supplemented with heat-inactivated 10% FCS (PAA, NJ), GM-CSF 813 Development speculate that the heterogeneity of human epidermal leukocytes might also reflect different precursors. To date, this concept has not been validated in humans, first and foremost because the immune cells of the human yolk sac remain poorly characterized (Janossy et al., 1986). However, given that the haematopoiesis in these organs in the human embryo and foetus is overlapping (Péault and Tavian, 2003), a dissection of the precise origin without concomitantly looking at the haematopoietic sites may be futile. In addition, further analysis is hindered because it is not currently possible to analyse embryonic skin before 9 weeks EGA, given the extremely low numbers of epidermal leukocytes at this developmental time point, which precludes a meaningful statistical analysis. Development (2014) doi:10.1242/dev.102699 RESEARCH ARTICLE Generation of organotypic skin cultures In vitro organotypic skin cultures were generated as described previously with minor modifications (Mildner et al., 2010). Briefly, a suspension of collagen type I (Biochrom, Berlin, Germany) containing human primary fibroblasts (1×105 cells/ml) was poured into cell-culture inserts (3 μm pore size; BD Biosciences) and allowed to form a gel for 2 hours at 37°C. The gels were then equilibrated with keratinocyte growth medium (KGM; Lonza) for 2 hours. Subsequently, primary human neonatal keratinocytes (1.5´106 cells; Lonza) together with FACS-sorted cord blood-derived CD1a+CD14–, CD1a–CD14– or CD1a–CD14+ (8×104 cells) precursors or CD14+CD16– blood monocytes (8×104 cells) were placed onto the collagen matrix. After overnight incubation the medium was removed from both the inserts and external wells, and placed in the external wells with 10 ml serum-free keratinocyte defined medium (SKDM), consisting of KGM but without bovine pituitary extract and supplemented with 1.3 mM calcium chloride (Sigma, Vienna, Austria), 10 μg/ml transferrin (Sigma), 50 μg/ml ascorbic acid (Sigma) and 0.1% BSA (Sigma). Medium was changed every second day. After 8 days of co-culture, the newly formed epidermis containing integrated LCs was mechanically peeled off, fixed in ice-cold acetone for 10 minutes and subjected to immunohistochemical staining. Cytokine determination in cell culture supernatants and lysates of organotypic skin cultures To assess the production and secretion of TGFβ1, GM-CSF and IL-34, culture media from organotypic skin cultures devoid of haematopoietic cells were collected at days 1, 3, 5 and 8 after a 24-hour incubation period in 1 ml SKDM. Supernatants were collected and cell lysates were prepared by incubation of the epidermal sheets in a 0.1% NP40 lysis buffer for 30 minutes on ice. Cell culture supernatants and lysates of epidermal sheets were stored at –80°C until use. Cytokine levels were determined by ELISA (R&D Systems) according to the manufacturer’s instructions. Experiments were performed in duplicate using cells from three different donors. Flow cytometry Single-cell suspensions were stained with the following monoclonal antibodies: PE anti-CD1c (AD5-8E7, Miltenyi), PE anti-CD33 (WM53, BD Biosciences), PE anti-CD34 (581, BD Biosciences), PE anti-CD36 (TR9, Biolegend, San Diego, CA, USA), PE anti-CD45 (HI30, BD Biosciences), PE anti CD117 (YB5.B8, BD Biosciences), PE anti-CD207 (DCGM4, Beckman Coulter), PE and APC anti-HLA-DR (L243; BD Biosciences), APC anti-CD14 (TuK4, Invitrogen), FITC anti-CD1a (HI149, BD Biosciences) and PE/Cy7 anti-CD45 (J.33; Beckman Coulter). Appropriate isotype controls were included. Dead cells were excluded with 7-AAD (Calbiochem, Darmstadt, Germany). Four-colour flow cytometry analyses were performed on an LSR-II (Becton Dickinson) and on a FACSAria (Becton Dickinson). Data were analysed using FlowJo software (Tree Star, Ashland, OR). Immunofluorescence Prenatal and adult skin specimens were embedded in Optimum Cutting Tissue compound (Tissue-Tek, Sakura Finetek, Zoeterwoude, The Netherlands), snap-frozen in liquid nitrogen, and stored at –80°C until 814 further processing. Six micrometer sections were cut, air dried, fixed in icecold acetone for 10 minutes and washed in PBS. Fixed sections were stained with unconjugated primary antibodies [anti-CD1c (L161; Serotec, Kidlington, UK), anti-CD14 (TuK4, Invitrogen), anti-HLA-DR (L243, BD Biosciences)] overnight at 4°C and subsequently incubated for 2 hours at room temperature with biotin-conjugated goat anti-mouse IgG (Vector Laboratories). Biotinylated antibodies were detected with streptavidinconjugated NorthernLight 637 (R&D Systems). Subsequently, sections were blocked with 10% mouse serum and 2% mouse IgG (BD Biosciences) for 1 hour at room temperature and stained overnight at 4°C with Alexa Fluor 555 anti-CD45 (MEM28, Exbio, Vestec, Czech Republic), FITC anti-CD34 (AC136, Miltenyi), FITC anti-CD36 (TR9, Immunotools, Friesoythe, Germany) and Alexa Fluor 488 anti-laminin 5 (D4B5; Millipore) to visualize the dermo-epidermal junction. Finally, the CD36 signal was amplified using anti-fluorescein Alexa Fluor 488-labelled rabbit immunoglobulin (Invitrogen). Slides were mounted using Vectashield (Vector Laboratories) and images were recorded using a confocal laser scanning microscope (LSM 410; Carl Zeiss) equipped with four lasers emitting lights at 405, 488, 543 and 633 nm. Immunohistochemistry After fixation, the epidermis of skin equivalents was washed in PBS. Epidermal sheets were then incubated with anti-CD1a (WM35, Peli Cluster, Amsterdam, The Netherlands), anti-CD207 (DCGM4, Beckman Coulter) or appropriate isotype antibodies overnight at 4°C, followed by blocking of endogenous peroxidase activity by incubating the sheets for 10 minutes in methanol containing 0.03% hydrogen peroxide. Subsequently, sections were incubated for 2 hours at room temperature with biotin-conjugated goat antimouse IgG using the Elite mouse IgG Vectastain kit (Vector Laboratories). Biotinylated antibodies were detected with HRP streptavidin and staining was visualized with AEC (Dako, Glostrup, Denmark). Finally, sections were mounted with Aquatex (Merck) and examined using an Eclipse 80 microscope (Nikon). Appropriate isotype controls (BD Biosciences) were included. Staining for TGFβ1 (Santa Cruz Biotechnology) and rabbit control serum (Dako) on cryostat section was performed as described previously (Schuster et al., 2009). Quantification of cells in skin sections and epidermal sheets Immunoreactive cells were counted in multiple skin sections with a total epidermal length of 4-27 cm or on epidermal sheets with a total surface area of 2.2-25.7 mm2 by two independent investigators (×40 object lens; Nikon). Statistics Differences between groups were assessed with the Mann-Whitney U-test, the Wilcoxon matched-pair signed rank test or Student’s t-test (GraphPad Software). The reported P-values are from two-sided tests. A P-value smaller than 5% was considered statistically significant. Acknowledgements We thank Dr Anton Stift (Department of Surgery, Medical University of Vienna, Austria) for the provision of adult human skin samples, and Drs Herbert Strobl and Muzlifah Haniffa for fruitful discussion. Competing interests The authors declare no competing financial interests. Author contributions C.S., M. Mildner, M. Mairhofer, W.B. and M.P. performed the experiments and analysed the data. C.F. and W.E. provided study material. C.S., A.K., E.T., G.S. and A.E.-B. conceived and designed the research. C.S. and A.E.-B. wrote the manuscript. Funding This project was funded by an Austrian Science Fund (FWF) grant [P19474-B13 to A.E.-B.]. Deposited in PMC for immediate release. Supplementary material Supplementary material available online at http://dev.biologists.org/lookup/suppl/doi:10.1242/dev.102699/-/DC1 Development (100 ng/ml), TNFα (2.5 ng/ml), SCF (20 ng/ml) and Flt3L (50 ng/ml; all Peprotech) for 7 days. On day 10, cells were harvested, stained and FACSsorted according to the expression of CD14 and CD1a using a FACSAria (Becton Dickinson). For the isolation of CD14+CD16– human peripheral blood monocytes from healthy volunteers, PBMCs were prepared by density gradient centrifugation using BD Vacutainer CPT tubes (BD Biosciences). T cells, B cells, NK cells and haematopoietic precursors were labelled with FITC-conjugated monoclonal antibodies against CD3 (UCHT1, An der Grub, Kaumberg, Austria), CD15 (W6D3, BD Biosciences), CD19 (LT19, Miltenyi), CD34 (AC136, Miltenyi) and CD56 (C218, Beckman Coulter) and subsequently depleted using anti-mouse IgG1 magnetic beads (Miltenyi). Resulting cells were then labelled with PE-Cy7-anti-CD16 (3G8, Beckman Coulter, Fullerton, CA) and APC-CD14 (TuK4, Invitrogen) and CD14+CD16– cells were sorted using a FACSAria. Development (2014) doi:10.1242/dev.102699 References Adkins, B., Leclerc, C. and Marshall-Clarke, S. (2004). Neonatal adaptive immunity comes of age. Nat. Rev. Immunol. 4, 553-564. Bechetoille, N., Dezutter-Dambuyant, C., Damour, O., André, V., Orly, I. and Perrier, E. (2007). Effects of solar ultraviolet radiation on engineered human skin equivalent containing both Langerhans cells and dermal dendritic cells. Tissue Eng. 13, 2667-2679. Borkowski, T. A., Letterio, J. J., Farr, A. G. and Udey, M. C. (1996). A role for endogenous transforming growth factor β 1 in Langerhans cell biology: the skin of transforming growth factor β 1 null mice is devoid of epidermal Langerhans cells. J. Exp. Med. 184, 2417-2422. Caux, C., Dezutter-Dambuyant, C., Schmitt, D. and Banchereau, J. (1992). GMCSF and TNF-α cooperate in the generation of dendritic Langerhans cells. Nature 360, 258-261. Caux, C., Vanbervliet, B., Massacrier, C., Dezutter-Dambuyant, C., de Saint-Vis, B., Jacquet, C., Yoneda, K., Imamura, S., Schmitt, D. and Banchereau, J. (1996). CD34+ hematopoietic progenitors from human cord blood differentiate along two independent dendritic cell pathways in response to GM-CSF+TNF α. J. Exp. Med. 184, 695-706. Chang-Rodriguez, S., Hoetzenecker, W., Schwärzler, C., Biedermann, T., Saeland, S. and Elbe-Bürger, A. (2005). Fetal and neonatal murine skin harbors Langerhans cell precursors. J. Leukoc. Biol. 77, 352-360. Chorro, L. and Geissmann, F. (2010). Development and homeostasis of ‘resident’ myeloid cells: the case of the Langerhans cell. Trends Immunol. 31, 438-445. Chorro, L., Sarde, A., Li, M., Woollard, K. J., Chambon, P., Malissen, B., Kissenpfennig, A., Barbaroux, J. B., Groves, R. and Geissmann, F. (2009). Langerhans cell (LC) proliferation mediates neonatal development, homeostasis, and inflammation-associated expansion of the epidermal LC network. J. Exp. Med. 206, 3089-3100. Di Nuzzo, S., Pavanello, P., Masotti, A., Giordano, G. and De Panfilis, G. (2009). Densities, distribution and phenotypic expression of T cells in human fetal skin. Arch. Dermatol. Res. 301, 753-755. Elbe, A., Tschachler, E., Steiner, G., Binder, A., Wolff, K. and Stingl, G. (1989). Maturational steps of bone marrow-derived dendritic murine epidermal cells. Phenotypic and functional studies on Langerhans cells and Thy-1+ dendritic epidermal cells in the perinatal period. J. Immunol. 143, 2431-2438. Elbe-Bürger, A. and Schuster, C. (2010). Development of the prenatal cutaneous antigen-presenting cell network. Immunol. Cell Biol. 88, 393-399. Fadel, S. and Sarzotti, M. (2000). Cellular immune responses in neonates. Int. Rev. Immunol. 19, 173-193. Foster, C. A. (1993). Heterogeneity among CD36+ cells in normal and diseased human skin. In Dermal Immune System (ed. B. J. Nickoloff), pp. 245-275. Ann Arbor, NY; London; Tokyo: CRC Press. Foster, C. A. and Elbe, A. (1997). Lymphocyte subpopulations of the skin. In Skin Immune System (SIS) (ed. J. D. Bos), pp. 85-108. Boca Raton, FL; New York, NY: CRC Press. Foster, C. A., Holbrook, K. A. and Farr, A. G. (1986). Ontogeny of Langerhans cells in human embryonic and fetal skin: expression of HLA-DR and OKT-6 determinants. J. Invest. Dermatol. 86, 240-243. Fujita, M., Furukawa, F., Horiguchi, Y., Ueda, M., Kashihara-Sawami, M. and Imamura, S. (1991). Regional development of Langerhans cells and formation of Birbeck granules in human embryonic and fetal skin. J. Invest. Dermatol. 97, 65-72. Geissmann, F., Prost, C., Monnet, J. P., Dy, M., Brousse, N. and Hermine, O. (1998). Transforming growth factor β1, in the presence of granulocyte/macrophage colony-stimulating factor and interleukin 4, induces differentiation of human peripheral blood monocytes into dendritic Langerhans cells. J. Exp. Med. 187, 961-966. Ginhoux, F. and Merad, M. (2010). Ontogeny and homeostasis of Langerhans cells. Immunol. Cell Biol. 88, 387-392. Ginhoux, F., Tacke, F., Angeli, V., Bogunovic, M., Loubeau, M., Dai, X. M., Stanley, E. R., Randolph, G. J. and Merad, M. (2006). Langerhans cells arise from monocytes in vivo. Nat. Immunol. 7, 265-273. Greter, M., Lelios, I., Pelczar, P., Hoeffel, G., Price, J., Leboeuf, M., Kündig, T. M., Frei, K., Ginhoux, F., Merad, M. et al. (2012). Stroma-derived interleukin-34 controls the development and maintenance of Langerhans cells and the maintenance of microglia. Immunity 37, 1050-1060. Hoeffel, G., Wang, Y., Greter, M., See, P., Teo, P., Malleret, B., Leboeuf, M., Low, D., Oller, G., Almeida, F. et al. (2012). Adult Langerhans cells derive predominantly from embryonic fetal liver monocytes with a minor contribution of yolk sac-derived macrophages. J. Exp. Med. 209, 1167-1181. Hubert, P., Bousarghin, L., Greimers, R., Franzen-Detrooz, E., Boniver, J. and Delvenne, P. (2005). Production of large numbers of Langerhans’ cells with intraepithelial migration ability in vitro. Exp. Dermatol. 14, 469-477. Jaksits, S., Kriehuber, E., Charbonnier, A. S., Rappersberger, K., Stingl, G. and Maurer, D. (1999). CD34+ cell-derived CD14+ precursor cells develop into Langerhans cells in a TGF-beta 1-dependent manner. J. Immunol. 163, 4869-4877. Development (2014) doi:10.1242/dev.102699 Janossy, G., Bofill, M., Poulter, L. W., Rawlings, E., Burford, G. D., Navarrete, C., Ziegler, A. and Kelemen, E. (1986). Separate ontogeny of two macrophage-like accessory cell populations in the human fetus. J. Immunol. 136, 4354-4361. Kaplan, D. H., Li, M. O., Jenison, M. C., Shlomchik, W. D., Flavell, R. A. and Shlomchik, M. J. (2007). Autocrine/paracrine TGFbeta1 is required for the development of epidermal Langerhans cells. J. Exp. Med. 204, 2545-2552. Laubach, V., Zöller, N., Rossberg, M., Görg, K., Kippenberger, S., Bereiter-Hahn, J., Kaufmann, R. and Bernd, A. (2011). Integration of Langerhans-like cells into a human skin equivalent. Arch. Dermatol. Res. 303, 135-139. Levy, O. (2005). Innate immunity of the human newborn: distinct cytokine responses to LPS and other Toll-like receptor agonists. J. Endotoxin Res. 11, 113-116. Mairhofer, M., Schulz, J. C., Parth, M., Beer, U., Zimmermann, H. and Kolbus, A. (2013). Evaluation of a xeno-free protocol for long-term cryopreservation of cord blood cells. Cell Transplant. 22, 1087-1099. Mildner, M., Jin, J., Eckhart, L., Kezic, S., Gruber, F., Barresi, C., Stremnitzer, C., Buchberger, M., Mlitz, V., Ballaun, C. et al. (2010). Knockdown of filaggrin impairs diffusion barrier function and increases UV sensitivity in a human skin model. J. Invest. Dermatol. 130, 2286-2294. Ordóñez, N. G. (2012). Immunohistochemical endothelial markers: a review. Adv. Anat. Pathol. 19, 281-295. Ouwehand, K., Spiekstra, S. W., Waaijman, T., Scheper, R. J., de Gruijl, T. D. and Gibbs, S. (2011). Technical advance: Langerhans cells derived from a human cell line in a full-thickness skin equivalent undergo allergen-induced maturation and migration. J. Leukoc. Biol. 90, 1027-1033. Péault, B. and Tavian, M. (2003). Hematopoietic stem cell emergence in the human embryo and fetus. Ann. N. Y. Acad. Sci. 996, 132-140. Régnier, M., Staquet, M. J., Schmitt, D. and Schmidt, R. (1997). Integration of Langerhans cells into a pigmented reconstructed human epidermis. J. Invest. Dermatol. 109, 510-512. Romani, N., Schuler, G. and Fritsch, P. (1986). Ontogeny of Ia-positive and Thy-1positive leukocytes of murine epidermis. J. Invest. Dermatol. 86, 129-133. Romani, N., Brunner, P. M. and Stingl, G. (2012a). Changing views of the role of Langerhans cells. J. Invest. Dermatol. 132, 872-881. Romani, N., Tripp, C. H. and Stoitzner, P. (2012b). Langerhans cells come in waves. Immunity 37, 766-768. Schaerli, P., Willimann, K., Ebert, L. M., Walz, A. and Moser, B. (2005). Cutaneous CXCL14 targets blood precursors to epidermal niches for Langerhans cell differentiation. Immunity 23, 331-342. Schuster, C., Vaculik, C., Fiala, C., Meindl, S., Brandt, O., Imhof, M., Stingl, G., Eppel, W. and Elbe-Bürger, A. (2009). HLA-DR+ leukocytes acquire CD1 antigens in embryonic and fetal human skin and contain functional antigen-presenting cells. J. Exp. Med. 206, 169-181. Schuster, C., Vaculik, C., Prior, M., Fiala, C., Mildner, M., Eppel, W., Stingl, G. and Elbe-Bürger, A. (2012). Phenotypic characterization of leukocytes in prenatal human dermis. J. Invest. Dermatol. 132, 2581-2592. Seré, K., Baek, J. H., Ober-Blöbaum, J., Müller-Newen, G., Tacke, F., Yokota, Y., Zenke, M. and Hieronymus, T. (2012). Two distinct types of Langerhans cells populate the skin during steady state and inflammation. Immunity 37, 905-916. Strobl, H., Riedl, E., Scheinecker, C., Bello-Fernandez, C., Pickl, W. F., Rappersberger, K., Majdic, O. and Knapp, W. (1996). TGF-β 1 promotes in vitro development of dendritic cells from CD34+ hemopoietic progenitors. J. Immunol. 157, 1499-1507. Tavian, M. and Péault, B. (2005). Embryonic development of the human hematopoietic system. Int. J. Dev. Biol. 49, 243-250. Thoma, S. J., Lamping, C. P. and Ziegler, B. L. (1994). Phenotype analysis of hematopoietic CD34+ cell populations derived from human umbilical cord blood using flow cytometry and cDNA-polymerase chain reaction. Blood 83, 21032114. Tripp, C. H., Chang-Rodriguez, S., Stoitzner, P., Holzmann, S., Stössel, H., Douillard, P., Saeland, S., Koch, F., Elbe-Bürger, A. and Romani, N. (2004). Ontogeny of Langerin/CD207 expression in the epidermis of mice. J. Invest. Dermatol. 122, 670-672. van de Laar, L., Coffer, P. J. and Woltman, A. M. (2012). Regulation of dendritic cell development by GM-CSF: molecular control and implications for immune homeostasis and therapy. Blood 119, 3383-3393. Wang, Y., Szretter, K. J., Vermi, W., Gilfillan, S., Rossini, C., Cella, M., Barrow, A. D., Diamond, M. S. and Colonna, M. (2012). IL-34 is a tissue-restricted ligand of CSF1R required for the development of Langerhans cells and microglia. Nat. Immunol. 13, 753-760. Zamora, C., Cantó, E., Nieto, J. C., Angels Ortiz, M., Juarez, C. and Vidal, S. (2012). Functional consequences of CD36 downregulation by TLR signals. Cytokine 60, 257-265. Ziegler-Heitbrock, L., Ancuta, P., Crowe, S., Dalod, M., Grau, V., Hart, D. N., Leenen, P. J., Liu, Y. J., MacPherson, G., Randolph, G. J. et al. (2010). Nomenclature of monocytes and dendritic cells in blood. Blood 116, e74-e80. Development RESEARCH ARTICLE 815