Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
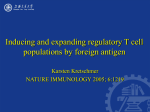
Human CD4+CD25+ Regulatory T Cells Share Equally Complex and Comparable Repertoires with CD4+CD25− Counterparts This information is current as of June 17, 2017. Kimberly A. Kasow, Xiaohua Chen, James Knowles, David Wichlan, Rupert Handgretinger and Janice M. Riberdy J Immunol 2004; 172:6123-6128; ; doi: 10.4049/jimmunol.172.10.6123 http://www.jimmunol.org/content/172/10/6123 Subscription Permissions Email Alerts This article cites 35 articles, 17 of which you can access for free at: http://www.jimmunol.org/content/172/10/6123.full#ref-list-1 Information about subscribing to The Journal of Immunology is online at: http://jimmunol.org/subscription Submit copyright permission requests at: http://www.aai.org/About/Publications/JI/copyright.html Receive free email-alerts when new articles cite this article. Sign up at: http://jimmunol.org/alerts The Journal of Immunology is published twice each month by The American Association of Immunologists, Inc., 1451 Rockville Pike, Suite 650, Rockville, MD 20852 Copyright © 2004 by The American Association of Immunologists All rights reserved. Print ISSN: 0022-1767 Online ISSN: 1550-6606. Downloaded from http://www.jimmunol.org/ by guest on June 17, 2017 References The Journal of Immunology Human CD4ⴙCD25ⴙ Regulatory T Cells Share Equally Complex and Comparable Repertoires with CD4ⴙCD25ⴚ Counterparts1 Kimberly A. Kasow, Xiaohua Chen, James Knowles, David Wichlan, Rupert Handgretinger, and Janice M. Riberdy2 D4⫹CD25⫹ T cells are an essential component of peripheral immune tolerance (1). Murine studies characterizing this population have become an area of intense investigation and have demonstrated a therapeutic potential for these cells in preventing the onset of autoimmune disease and graft-vshost disease (2– 4). However, the precise mechanisms that control their development and functional activity have remained elusive. Studies of human CD4⫹CD25⫹ regulatory T cells have been even more limited (5–9). Despite the many unresolved questions regarding regulatory T cells, the general consensus is that both murine and human CD4⫹CD25⫹ T cells require activation through their TCR and cell-cell contact to mediate their activity (10 –12). An important feature of these cells is that once activated, they are able to downmodulate immune responses in an Ag-nonspecific manner (13). In terms of the development of CD4⫹CD25⫹ T cells, murine studies have shown that this subset can be generated in the thymus and requires signals through the IL-2R (14, 15). Additional murine studies have also demonstrated that the expression of a member of the Forkhead transcription factor family, Foxp3, is necessary for the development of CD4⫹CD25⫹ T cells, and animals deficient in C Division of Stem Cell Transplantation, St. Jude Children’s Research Hospital, Memphis, TN 38105 Received for publication October 30, 2003. Accepted for publication March 16, 2004. The costs of publication of this article were defrayed in part by the payment of page charges. This article must therefore be hereby marked advertisement in accordance with 18 U.S.C. Section 1734 solely to indicate this fact. 1 This work was supported by Training Grant T32CA70089 from the National Cancer Institute (to K.A.K.) and the American Lebanese and Syrian Associated Charities. 2 Address correspondence and reprint requests to Dr. Janice M. Riberdy, Division of Stem Cell Transplantation, Mail Stop 321, St. Jude Children’s Research Hospital, 332 North Lauderdale Street, Memphis, TN 38105. E-mail address: [email protected] Copyright © 2004 by The American Association of Immunologists, Inc. this molecule develop severe autoimmune and inflammatory dysfunctions (16 –18). The human allele, Foxp3, is likely to be a critical factor in the development of human CD4⫹CD25⫹ T cells as well. Individuals with the fatal syndrome of immune dysfunction, polyendocrinopathy, enteropathy, and X-linked inheritance have mutations at this locus (19). It is clear that the development of a functional CD4⫹CD25⫹ T cell population is critical for the maintenance of a healthy immune system. However, as activated CD4⫹CD25⫹ T cells can suppress an immune response in an Ag-nonspecific manner, it is equally important to understand what mechanisms regulate the activation and functional capability of these cells (13). One feature that is likely to contribute to the regulation of these cells is the overall avidity of the TCR for its cognate ligand. Studies have suggested that thymocytes with high affinity TCRs can be directed toward a regulatory T cell lineage (20). Consistent with this idea is the observation that reducing the threshold of activation in thymocytes preferentially selects a population of CD4⫹CD25⫹ T cells with phenotypic and functional characteristics of regulatory T cells (21). Yet, the high affinity nature of CD4⫹CD25⫹ T cells does not appear to skew the repertoire, as examination of murine T cell repertoires by V staining has shown a diverse usage of V gene segments, with a similar distribution of the CD4⫹CD25⫺ T cell population (22–24). Limited analysis of V gene usage in human CD4⫹CD25⫹ regulatory T cells from peripheral blood suggests that these cells comprise a diverse repertoire. However, a comprehensive study examining the repertoire of human CD4⫹CD25⫹ regulatory T cells from multiple anatomical niches has been lacking (25). Interestingly, emerging data suggest that humans may also expand CD4⫹CD25⫹ T cells in the periphery to compensate for an increased life span accompanied by decreased thymic output (26, 27). Temporal studies to examine whether such peripheral mechanisms alter the repertoire as an individual ages may shed 0022-1767/04/$02.00 Downloaded from http://www.jimmunol.org/ by guest on June 17, 2017 CD4ⴙCD25ⴙ T cells are critical mediators of peripheral immune tolerance. However, many developmental and functional characteristics of these cells are unknown, and knowledge of human regulatory T cells is particularly limited. To better understand how human CD4ⴙCD25ⴙ T cells develop and function, we examined the diversity of CD4ⴙCD25ⴙ and CD4ⴙCD25ⴚ T cell repertoires in both thymus and peripheral blood. Levels of T receptor excision circles (TREC) were comparable in purified CD4ⴙCD25ⴙ and CD4ⴙCD25ⴚ thymic populations, but were significantly higher than those in samples derived from peripheral blood, consistent with murine studies demonstrating thymic development of CD4ⴙCD25ⴙ regulatory T cells. Surprisingly, CD4ⴙCD25ⴚ T cells isolated from peripheral blood had greater TREC quantities than their CD4ⴙCD25ⴙ counterparts, supporting the possibility of extrathymic expansion as well. CD4ⴙCD25ⴙ and CD4ⴙCD25ⴚ T cells from a given individual showed overlapping profiles with respect to diversity by V staining and spectratyping. Interestingly, CD4ⴙCD25ⴙ T cells have lower quantities of CD3 than CD4ⴙCD25ⴚ T cells. Collectively, these data suggest that human CD4ⴙCD25ⴙ T cells recognize a similar array of Ags as CD4ⴙCD25ⴚ T cells. However, reduced levels of TCR on regulatory T cells suggest different requirements for activation and may contribute to how the immune system regulates whether a particular response is suppressed or augmented. The Journal of Immunology, 2004, 172: 6123– 6128. 6124 CD4⫹CD25⫹ REGULATORY T CELL REPERTOIRE Materials and Methods Thymic and peripheral blood cells Peripheral blood cells from normal healthy donors were collected at St. Jude Children’s Research Hospital (Memphis, TN) with permission from the institutional review board. Thymic tissues were obtained from children undergoing cardiac procedures at LeBonheur Children’s Medical Center (Memphis, TN). The University of Tennessee Memphis institutional review board and the LeBonheur executive committee granted approval for use of these specimens. Purification of T cell subsets Single-cell suspensions were prepared from thymic tissue. Both thymic and peripheral blood cells were centrifuged over a gradient of Ficoll-Paque Plus (Pharmacia Biotech, Uppsala, Sweden). Cells were washed with Dulbecco’s PBS (Cambrex, Walkersville, MD) and resuspended in MACS buffer (PBS, 2 mM EDTA, and 0.5% human serum albumin or BSA). CD4⫹CD25⫹ and CD4⫹CD25⫺ T cells were purified by magnetic bead separation using an autoMACS cell separator (Miltenyi Biotec, Bergisch Gladbach, Germany). Thymocytes were first depleted of CD8⫹ cells using CD8 microbeads (Miltenyi Biotec). Untouched CD4⫹ T cells were purified from both peripheral blood cells and CD8-depleted thymocytes by magnetic depletion using a CD4⫹ T cell isolation kit (Miltenyi Biotec). CD4⫹ T cell populations were fractionated into CD25⫹ and CD25⫺ subsets by either a single-step positive selection using anti-CD25 microbeads (Miltenyi Biotec) or a two-step isolation using anti-CD25 PE (ACT-1; DAKO Cytomation, Glostrup, Denmark), followed by anti-PE microbeads (Miltenyi Biotec). All microbead isolations followed the manufacturer’s instructions (Miltenyi Biotec). For the purified PBL and thymus products, the CD4⫹ purity range was 82–98% (see Fig. 1, inset, for representative CD4⫹CD25⫹ purification). Flow cytometry Thymocytes and PBL were analyzed using a BD LSR or BD LSRII flow cytometer and Cell Quest Pro, BD FACSDiVa (BD Biosciences, San Jose, CA), or FlowJo software (Tree Star, Ashland, OR). The following mAbs were used to check the purity of the positive and negative selected cells: anti-CD3 and anti-CD4 (SK7 and SK3, respectively; BD Biosciences), anti-CD8 and anti-CD25 (DK25 and ACT1, respectively; DAKO Cytomation), and anti-CD25 (M-A251; BD PharMingen San Diego, CA). The anti-V family Abs were purchased from Immunotech (Marseilles, France). DNA and RNA isolation DNA was isolated from purified CD4⫹CD25⫹ and CD4⫹CD25⫺ T cells using the QIAamp DNA Mini kit (Qiagen, Valencia, CA) following the manufacturer’s instructions. RNA was isolated from purified CD4⫹CD25⫹ 3 Abbreviations used in this paper: TREC, T receptor excision circle; ⌬Ct, change in Ct value; sj, signal joint. FIGURE 1. Relative TREC levels. A, CD4⫹CD25⫹ and CD4⫹CD25⫺ T cells from human thymus and PBL were purified. The inset shows CD25 expression on the isolated populations after a typical purification. Relative TREC levels were determined by real-time PCR, and the mean of duplicate reactions is shown in arbitrary units. Bars with the same color scheme represent purified CD4⫹CD25⫹ and CD4⫹CD25⫺ T cells from the same individual, as indicated. Note that thymic and PBL samples are not from the same individual. All reactions had slopes between ⫺3.1 and ⫺3.4. B, Amplification curves for CD4⫹CD25⫹ (f) and CD4⫹CD25⫺ (E) T cell populations. The y-axis represents the values of normalized target-specific fluorescence signals (change in reaction), and the x-axis shows the number of PCR cycles. The Ct values are defined as the PCR cycle at which the change in reaction passes a threshold of 10 SD above the baseline fluorescence (threshold shown as solid line). ⌬Ct in these figures represents the difference in Ct value between the CD4⫹CD25⫹ and CD4⫹CD25⫺ T cell populations. The amplification reactions for each sample were performed in duplicate. and CD4⫹CD25⫺ T cells using the Rneasy Mini kit (Qiagen) following the manufacturer’s instructions. Detection and quantitation of signal-joint (sj) TREC Relative TREC levels were determined as previously described (28). In brief, DNA was isolated from purified CD4⫹CD25⫹ and CD4⫹CD25⫺ T cell populations, and real-time PCR was performed on 200 ng of DNA using an ABI 7700 system (Applied Biosystems, Foster City, CA). All samples were studied in duplicate reactions, using primers and conditions described by Hazenberg et al. (28). The C␣ constant region was used as an internal control to normalize for input DNA. A standard curve was generated by cloning the sj TREC fragment in pCR 2.1-TOPO vector using TOPO TA Cloning kit (Invitrogen, Carlsbad, CA). The standard curve and TREC values were analyzed by Sequence Detector software. The number of TREC molecules in the sample was calculated as number of copies per 105 cells. Downloaded from http://www.jimmunol.org/ by guest on June 17, 2017 light on the role of CD4⫹CD25⫹ T cells in immunological defects associated with the elderly. To better understand how human CD4⫹CD25⫹ T cells develop and function, we have extensively analyzed the diversity of the CD4⫹CD25⫹ T cell repertoire in both thymic and peripheral blood compartments by V staining and spectratyping. We have also compared the regulatory T cell subset with the CD4⫹CD25⫺ counterpart for T receptor excision circle (TREC)3 content and CD3 levels. Together, our data demonstrate that human CD4⫹CD25⫹ T cells are probably generated in the thymus with a repertoire of comparable diversity to that of CD4⫹CD25⫺ T cells. Interestingly, TREC data are consistent with the hypothesis that peripheral expansion could contribute to the maintenance of this population (26, 27). Finally, lower levels of CD3 in both thymic and peripheral blood populations of naturally selected human CD4⫹CD25⫹ T cells support the idea that these cells are a high affinity population with different requirements for activation. Such alterations in the threshold of activation provide the immune system with key mechanisms to control the level of suppressor activity associated with CD4⫹CD25⫹ regulatory T cells. The Journal of Immunology TCR V CDR3 size spectratyping The CDR3 size distribution of 27 distinct TCR V families was determined by RT-PCR as previously described (29). In brief, RNA was extracted and cDNA was synthesized using Superscript II reverse transcriptase (Invitrogen). PCR was performed with a forward primer specific for one of the TCR V families along with a constant C reverse primer labeled with fluorescent FAM, using the conditions described by Gorski et al. (29). RT-PCR products were analyzed on an ABI PRISM 310 Genetic Analyzer (Applied Biosystems), using GeneScan software. The normal TCR V CDR3 size is characterized by a Gaussian distribution, containing 8 –10 peaks for each V subfamily. The overall complexity of TCR V subfamilies was determined by spectratype complexity scoring as previously described (30). Quantitation of CD3-⑀ by real-time RT-PCR Relative levels of CD3-⑀ were determined by real-time RT-PCR as previously described (31). Briefly, RNA was extracted, cDNA was synthesized, and PCR was performed using the conditions and CD3-⑀ forward and reverse primers described by Pennington et al. (31). Experimental samples and data points for the standard curve were assayed in duplicate. Human GAPDH mRNA was used as the endogenous control to normalize for input RNA. CD4⫹CD25⫹ T cells are potent mediators of tolerance and can down-modulate immune responses in the settings of both autoimmunity and viral infection (1–3, 32). Once activated through the TCR, these cells can regulate a variety of effector cell functions in an Ag-nonspecific manner (13). The lack of Ag specificity suggests a promising therapeutic potential for these cells for human disease, because one does not have to identify the precise antigenic epitope in each MHC haplotype. However, delineating the mechanisms that control the development and function of CD4⫹CD25⫹ T cells has been a challenge, and many questions remain unanswered. In particular, studies addressing how human CD4⫹CD25⫹ T cells develop, maintain homeostasis, and regulate activity have been both difficult and limited (5–11, 27). Here, we assay for evidence of thymic development and compare the repertoires of CD4⫹CD25⫹ T cells with the CD4⫹CD25⫺ counterparts to determine whether the same spectrum of Ags capable of eliciting a robust effector cell response might also stimulate potent regulatory T cell activity. for the purified PBL cells ranged from 0.5 to 4.3 between the CD4⫹CD25⫹ and CD4⫹CD25⫺ T cell subsets (Fig. 1). TCR V staining To address whether human CD4⫹CD25⫹ T cells exhibit a diverse repertoire, CD4⫹CD25⫹ and CD4⫹CD25⫺ T cells from both thymus (n ⫽ 2) and peripheral blood (n ⫽ 4) were isolated. Purified cells were doubly stained with anti-CD25 and a specific V Ab to analyze a panel of 21 subfamilies by flow cytometry. Although the precise fingerprint varied between individuals, the profiles of TCR V usage from CD4⫹CD25⫹ T cells were strikingly similar to those of the CD4⫹CD25⫺ counterparts (Fig. 2). This was true for purified thymic subsets as well as isolated PBL populations. Spectratyping Although TCR V staining examines the prevalence of specific V families within the repertoire, spectratyping dissects the diversity within a particular family (29). Although we did not observe any repertoire skewing in the CD4⫹CD25⫹ subset at the level of TCR V gene usage, the high avidity of CD4⫹CD25⫹ T cells could alter the distribution within a given V family. Thus, we compared the spectratyping profiles of purified human CD4⫹CD25⫹ T cells with the CD4⫹CD25⫺ counterparts for five thymii and six peripheral blood samples. Fig. 3 shows the profiles of representative thymocyte and PBL samples. In general, the profiles for both thymic and PBL CD4⫹CD25⫹ T cell populations were as broadly complex as those from the CD4⫹CD25⫺ T cell subset. To validate that the CD4⫹CD25⫹ and CD4⫹CD25⫺ T cell subsets were equally complex, each isolated sample was given a spectratype complexity score, as described by Wu et al. (30). In brief, the number of oligoclonal peaks for each V family was counted. For CD4⫹CD25⫹ T cells isolated from thymus and PBL, the ranges of complexity scores were 195–210 and 187–210, respectively. Similarly, the score ranges of CD4⫹CD25⫺ T cells from thymus and PBL were 206 –214 and 188 –215, respectively. T receptor excision circle analysis One marker that can be used as a rough estimate of developmental proximity to the thymus is the level of T receptor excision circles. To ascertain whether the level of TREC was different between the CD4⫹CD25⫹ and CD4⫹CD25⫺ T cell subsets, specific populations were isolated from human thymus (n ⫽ 3) and PBL (n ⫽ 5). Note that thymic and PBL samples were not from the same individual and could not be directly compared, but ranges of TREC levels for purified thymic and PBL cells could be compared to determine relative trends. TREC values for the various purified subsets were assayed by real-time PCR. Fig. 1A illustrates the range of TREC content observed in different individuals (5,175– 200,410 copies/105 cells for thymus and 23–2,386 copies/105 cells for PBL). Despite variation in TREC values between different thymii, CD4⫹CD25⫹ and CD4⫹CD25⫺ thymocytes isolated from the same thymus did not have significantly different levels of TREC. Relative TREC values were independent of the actual number of cells or the quantity of DNA isolated (data not shown). Importantly, the range of TREC values from thymocytes was significantly higher than that found in the PBL samples (Fig. 1A; p ⫽ 0.001). In contrast to purified thymocytes, four of five individuals had decreased levels of TREC in the CD4⫹CD25⫹ PBL compared with the CD4⫹CD25⫺ counterpart. The change in Ct values (⌬Ct) FIGURE 2. V analysis. Purified CD4⫹CD25⫹ and CD4⫹CD25⫺ thymocyte and lymphocyte populations were stained for CD25 and TCR V before analysis by flow cytometry. f, CD25⫹ T cells; E, CD25⫺ T cells. Downloaded from http://www.jimmunol.org/ by guest on June 17, 2017 Results 6125 6126 CD4⫹CD25⫹ REGULATORY T CELL REPERTOIRE In all comparisons of CD4⫹CD25⫹ T cells with CD4⫹CD25⫺ T cells the ranges overlapped, and no significant differences were observed in the overall breadth of the repertoires. Occasionally, an oligoclonal expansion was observed in a particular V family that was unique to either the CD4⫹CD25⫹ or CD4⫹CD25⫺ T cell subset (see V 25 for thymus and V 23 for PBL; Fig. 3), but, in general, the repertoires were overlapping. CD3 expression The striking similarity between the repertoires suggested that the spectrum of Ags capable of either selecting CD4⫹CD25⫹ T cells in the thymus or activating CD4⫹CD25⫹ T cells in the periphery could similarly stimulate the CD4⫹CD25⫺ T cell counterparts. Although many parameters contribute to both thymic selection and immune responses in the periphery, one factor that could affect whether the CD4⫹CD25⫹ T cell subset was preferentially activated would be the density of TCR expression (21). We have examined CD3 expression by real-time RT-PCR for CD4⫹CD25⫹ and CD4⫹CD25⫺ T cell populations isolated from both thymus (n ⫽ 2) and PBL (n ⫽ 3). In all cases, the CD4⫹CD25⫹ T cell population had dramatically lower levels of CD3 RNA (Fig. 4A). Flow cytometric analysis of mean fluorescence intensity also demonstrates an inverse correlation between CD25 and CD3 expression, with the CD4⫹CD25bright population having the lowest levels of CD3 (Fig. 4B). This correlation was observed for both thymus and PBL samples. In addition, purified CD4⫹CD25⫹ T cells exhibited decreased surface expression of CD3 compared with the CD4⫹CD25⫺ counterpart whether they were isolated from thymus (n ⫽ 2) or PBL (n ⫽ 4). Preliminary studies showed similar results with anti-TCR staining (data not shown). Discussion Ideally, one would compare thymic and peripheral blood samples from the same individual. However, thymic samples originated from children undergoing cardiac surgery, and obtaining peripheral blood was not feasible. Peripheral blood samples were obtained from adult donors. Thus, our strategy was to compare the CD4⫹CD25⫹ T cell population with the CD4⫹CD25⫺ counterpart. This approach allowed us to determine which trends were associated with either a particular subset of cells or an anatomical niche, but did not allow for a direct comparison between thymic and peripheral blood repertoires. At first, we sought evidence that human CD4⫹CD25⫹ T cells were generated in the thymus, as many murine studies have elegantly shown (14, 15, 33). As a thymocyte rearranges its TCR genes, TREC is generated, and high levels of these excision circles are generally thought to reflect recent developments in the thymus. However, as TREC is not replicated during mitosis, proliferation of a particular T cell subset will affect the overall level of TREC (28). Higher relative TREC values in both CD4⫹CD25⫹ and CD4⫹CD25⫺ thymocytes compared with the PBL samples strongly suggests that human CD4⫹CD25⫹ thymocytes are not simply peripheral lymphocytes relocated in the thymus. Rather, these cells are most likely generated in the thymus. Higher TREC in purified thymocytes was not simply due to the fact that thymic samples were from children and PBL were from adults. Average TREC levels from the PBL of children posthemopoietic stem cell transplant with documented immune reconstitution were still noticeably lower than the range seen for thymic samples (X. Chen, data not shown). Comparable TREC values in both CD4⫹CD25⫹ and CD4⫹CD25⫺ thymocytes also suggest that any proliferation is likely to be limited and equivalent in both populations. Comparative studies of patients with thymic hypoplasia to healthy age-matched controls have shown that the functional capacity of a thymus is important in maintaining normal numbers of CD4⫹CD25⫹ T cells. One striking observation from this study is a decline in the absolute number of CD4⫹CD25⫹ T cells from Downloaded from http://www.jimmunol.org/ by guest on June 17, 2017 FIGURE 3. Spectratyping. Purified CD4⫹CD25⫹ and CD4⫹CD25⫺ thymocytes and lymphocytes were assayed by RT-PCR for CDR3 length to determine the spectratyping profiles of each V subfamily. The Gaussian curve represents expression of the V subfamilies within each TCR V family. The Journal of Immunology birth to 3 years of age in the control group. Importantly, the absolute number of CD4⫹CD25⫹ T cells remained relatively constant in older children and adults (34). It has been also been suggested that human CD4⫹CD25⫹ T cells may expand in the periphery to compensate for the increased life span and decreased thymic output seen in humans (27). A decreased amount of TREC in the CD4⫹CD25⫹ T cells isolated from PBL is consistent with the idea that human regulatory T cells may also expand in the periphery and thus provide a mechanism to maintain absolute numbers of this population (26, 27, 34). The extent to which such putative mechanisms exist remains unknown and warrants further investigation. Alternatively, one must consider the possibility that some of the CD4⫹ T cells expressing CD25 are recently activated T cells responding to Ag. Proliferation in response to stimulation would artificially dilute the overall TREC content of the CD4⫹CD25⫹ T cell population. It is unlikely, however, that four of the five individuals were acutely infected at the time of sam- pling. Furthermore, routine functional analysis of CD4⫹CD25⫹ T cells isolated with the CD25 microbeads demonstrated functional suppressor activity (D. Wichlan, data not shown). Interestingly, purification methods that isolate both CD25bright and CD25int cells do not yield functionally active suppressor cells. In contrast, CD25bright cells alone demonstrate potent activity (D. Wichlan, manuscript in preparation). Experiments to address whether the CD25 intermediate cells are actively inhibiting the function of the CD25bright cells are underway (D. Wichlan, data not shown). Thus, understanding the functional composition of purified CD4⫹CD25⫹ T cells remains a challenge for future clinical strategies. It is clear that CD4⫹CD25⫹ T cells must be stimulated through the TCR to become functionally active (10 –12). However, once activated, this population is able to down-modulate immune responses in an Ag-nonspecific manner (13). Thus, a critical question is whether the same spectrum of Ags capable of activating a conventional CD4⫹ T cell response is able to stimulate CD4⫹CD25⫹ T cells. Previous murine studies have compared the CD4⫹CD25⫹ and CD4⫹CD25⫺ T cell repertoires with respect to V gene usage and demonstrated that the regulatory T cell repertoire is indeed diverse and remarkably similar to the CD4⫹CD25⫺ T cell subset (22–24). However, murine studies have also suggested that CD4⫹CD25⫹ T cells are a high avidity population (20, 35). In support of this idea, experimental manipulation to reduce the threshold of activation demonstrated that thymocytes can be diverted into the CD4⫹CD25⫹ T cell lineage (21). Thus, it was conceivable that certain high avidity clones could be preferentially selected in the thymus, and the clonal distribution could vary between the CD4⫹CD25⫹ and CD4⫹CD25⫺ T cell subsets. Likewise, exposure to Ag in the periphery could alter the clonal makeup of particular V families. Our spectratyping has shown that despite the high avidity nature of CD4⫹CD25⫹ T cells, the distribution of clones within the various V subfamilies largely overlaps with that of the CD4⫹CD25⫺ counterparts. Also worth considering is the possibility that although the repertoires are very similar with respect to V gene usage and complexity, important differences may still exist at the level of Ag specificity. In a simplified view, having equally complex repertoires between subsets would imply that the same Ags capable of eliciting a robust immune response from the CD4⫹CD25⫺ T cells could activate the regulatory T cell component. In response to autoimmune reactions it would be highly desirable to activate CD4⫹CD25⫹ regulatory cells as efficiently as effector cell responses. In contrast, during an infection it would be advantageous to preferentially activate the effector cells before stimulating a population capable of initiating a dampening effect. One characteristic that may contribute to whether the CD4⫹CD25⫹ T cells are optimally stimulated is the density of TCR expression (21). The realtime RT-PCR of CD3 levels demonstrates a dramatically lower level of expression in the CD4⫹CD25⫹ T cell population in both thymocytes and PBL. Altering the threshold of activation by modulating the density of TCR provides a mechanism to differentially activate the CD4⫹CD25⫹ and CD4⫹CD25⫺ T cell subsets, despite the overall similarity in repertoires. In summary, our TREC data with human thymocytes and PBL are consistent with murine studies demonstrating that CD4⫹CD25⫹ T cells are generated in the thymus before migrating to the periphery (14, 15, 33). Interestingly, the decreased levels of TREC in the CD4⫹CD25⫹ T cells isolated from peripheral blood support the idea that peripheral mechanisms of homeostasis may be important in maintaining the levels of regulatory T cells as thymic output decreases (26, 27, 34). Nonetheless, it is clear that Downloaded from http://www.jimmunol.org/ by guest on June 17, 2017 FIGURE 4. CD3⑀ expression. A, Amplification curves for CD3⑀ expression in CD4⫹CD25⫹ and CD4⫹CD25⫺ T cells purified from thymus and PBL (f, CD4⫹CD25⫹ T cells; E, CD4⫹CD25⫺ T cells). The change in reaction and ⌬Ct defined are described in Fig. 1B. B, Flow cytometry of CD3 expression on unpurified CD8⫺CD4⫹ thymocytes and CD4⫹ lymphocytes with the indicated level of CD25 (CD25⫺, CD25int, and CD25bright). The insets show the actual CD25 gates for cells depicted in the CD3 histograms. 6127 6128 the repertoire of human CD4⫹CD25⫹ T cells is as broad and complex as the CD4⫹CD25⫺ T cell population. Finally, the precise mechanisms that determine whether an immune response is preferentially ablated by regulatory T cells remain unclear, but differential TCR expression may be one of the many parameters contributing to the overall outcome. Acknowledgments We thank Drs. Ray Barfield, Thasia Leimig, and Mario Otto for their assistance in procuring and processing the thymic specimens, and Jim Houston and Marti Holladay for expert help with flow cytometry. We also thank Dr. Wing Leung for critical reading of the manuscript and help with statistical analysis. References 15. Bensinger, S. J., A. Bandeira, M. S. Jordan, A. J. Caton, and T. M. Laufer. 2001. Major histocompatibility complex class II-positive cortical epithelium mediates the selection of CD4⫹25⫹ immunoregulatory T cells. J. Exp. Med. 194:427. 16. Hori, S., T. Nomura, and S. Sakaguchi. 2003. Control of regulatory T cell development by the transcription factor Foxp3. Science 299:1057. 17. Fontenot, J. D., M. A. Gavin, and A. Y. Rudensky. 2003. Foxp3 programs the development and function of CD4⫹CD25⫹ regulatory T cells. Nat. Immunol. 4:330. 18. Khattri, R., T. Cox, S.-A. Yasayko, and F. Ramsdell. 2003. An essential role for scurfin in CD4⫹CD25⫹ T regulatory cells. Nat. Immunol. 4:337. 19. Bennett, C. L., J. Christie, F. Ramsdell M. E. Brunkow, P. J. Ferguson, L. Whitesell, T. E. Kelly, F. T. Saulsbury, P. F. Chance, and H. D. Ochs. 2001. The immune dysregulation, polyendocrinopathy, enteropathy, X-linked syndrome (IPEX) is caused by mutations of Foxp3. Nat. Genet. 27:20. 20. Jordan, M. S., A. Boesteanu, A. J. Reed, A. L. Petron, A. E. Holenbeck, M. A. Lerman, A. Naji, and A. J. Caton. 2001. Thymic selection of CD4⫹CD25⫹ regulatory T cells induced by an agonist self-peptide. Nat. Immunol. 2:301. 21. Stephens, G. L., and L. Ignatowicz. 2003. Decreasing the threshold for thymocyte activation biases CD4⫹ cells toward a regulatory (CD4⫹CD25⫹) lineage. Eur. J. Immunol. 33:1282. 22. Romagnoli, P., D. Hudrisier, and J. P. M. van Meerwijk. 2002. Preferential recognition of self antigens despite normal thymic deletion of CD4⫹CD25⫹ regulatory T cells. J. Immunol. 168:1644. 23. Pacholczyk, R., P. Kraj, and L. Ignatowicz. 2002. Peptide specificity of thymic selection of CD4⫹CD25⫹ T cells. J. Immunol. 168:613. 24. Taams, L., M. Vukmanovic-Stejic, M. Salmon, and A. Akbar. 2003. Immune regulation by CD4⫹CD25⫹ regulatory T cells: implications for transplantation tolerance. Trans. Immunol. 11:277. 25. Taams, L. S., M. Vukmanovic-Stejic, J. Smith, P. J. Dunne, J. M. Fletcher, F. J. Plunkett, S. B. Ebeling, G. Lombardi, M. H. Rustin, J. W. J. Bijlsma, et al. 2002. Antigen-specific T cell suppression by human CD4⫹CD25⫹ regulatory T cells. Eur. J. Immunol. 32:1621. 26. Taams, L. S., J. Smith, M. H. Rustin, M. Salmon, L. W. Poulter, and A. N. Akbar. 2001. Human anergic/suppressive CD4⫹CD25⫹ T cells: a highly differentiated and apoptosis-prone population. Eur. J. Immunol. 31:1122. 27. Akbar, A. N., L. S. Taams, M. Salmon, and M. Vukmanovic-Steijic. 2003. The peripheral generation of CD4⫹CD25⫹ regulatory T cells. Immunology 109:319. 28. Hazenberg, M. D., S. A. Otto, J. W. T. Cohen Stuart, M. C. M. Verschuren, J. C. C. Borleffs, C. A. B. Boucher, R. A. Coutinho, J. M. A. Lange, T. F. Rinke de Wit, A. Tsegaye, et al. 2000. Increased cell division but not thymic dysfunction rapidly affects the T-cell receptor excision circle content of the naive T cell population in HIV-1 infection. Nat. Med. 6:1036. 29. Gorski, J., T. Piatek, M. Yassai, J. Gorski, and K. Maslanka. 1995. Improvements in repertoire analysis by CDR3 spectratyping Bifamily PCR. Ann. NY Acad. Sci. 756:99. 30. Wu, C. J., A. Chillemi, E. P. Alyea, E. Orsini, D. Neuberg, R. J. Soiffer, and J. Ritz. 2000. Reconstitution of T-cell receptor repertoire diversity following T-cell depleted allogeneic bone marrow transplantation is related to hematopoietic chimerism. Transplantation 95:352. 31. Pennington, J., S. F. Garner, J. Sutherland, and L. M. Williamson. 2001. Residual subset population analysis in WBC-reduced blood components using real-time PCR quantitation of specific mRNA. Transfusion 41:1591. 32. Susmit, S., U. Kumaraguru, C. D. Pack, S. Lee, and B. Rouse. 2003. CD4⫹CD25⫹ T cells regulate virus-specific primary and memory CD8⫹ T cell responses. J. Exp. Med. 198:889. 33. Papiernik, M., M. L. Moraes, C. Pontoux, F. Vasseur, and C. Penit. 1998. Regulatory CD4⫹ T cells; expression of IL-2R ␣ chain, resistance to clonal deletion and IL-2 dependency. Int. Immunol. 10:371. 34. Sullivan K. E., D. McDonald-McGinn, and E. H. Zackai. 2002. CD4⫹CD25⫹ T cell production in healthy humans and in patients with thymic hypoplasia. Clin. Diag. Lab. Immunol. 9:1129. 35. Suto, A., H. Nakajima, K. Ikeda, S. Kubo, T. Nakayama, M. Taniguchi, T. Saito, and I. Iwamoto. 2002. CD4⫹CD25⫹ T-cell development is regulated by at least 2 distinct mechanisms. Blood 99:555. Downloaded from http://www.jimmunol.org/ by guest on June 17, 2017 1. Sakaguchi, S., N. Sakaguchi, J. Shimizu, S. Yamazaki, T. Sakihama, M. Itoh, Y. Kuniyasu, T. Nomura, M. Toda, and T. Takahashi. 2001. Immunologic tolerance maintained by CD25⫹CD4⫹ regulatory T cells: their common role in controlling autoimmunity, tumor immunity, and transplantation tolerance. Immunol. Rev. 182:18. 2. Maloy, K. J., and F. Powie. 2001. Regulatory T cells in the control of immune pathology. Nat. Immunol. 2:816. 3. Wood, K. J., and S. Sakaguchi. 2003. Regulatory T cells in transplantation tolerance. Nat. Rev. Immunol. 3:199. 4. Shevach, E. M. 2000. Regulatory T cells in autoimmunity. Annu. Rev. Immunol. 18:423. 5. Jonuleit, H., E. Schmitt, M. Stassen, A. Tuettenberg, J. Knop, and A. H. Enk. 2001. Identification and functional characterization of human CD4⫹CD25⫹ T cells with regulatory properties isolated from peripheral blood. J. Exp. Med. 193:1285. 6. Levings, M. K., R. Sangregorio, and M.-G. Roncarolo. 2001. Human CD25⫹CD4⫹ T regulatory cells suppress naive and memory T cell proliferation and can be expanded in vitro without loss of function. J. Exp. Med. 193:1295. 7. Dieckmann, D., H. Plottner, S. Berchtold, T. Berger, and G. Schuler. 2001. Ex vivo isolation and characterization of CD4⫹CD25⫹ T cells with regulatory properties from human blood. J. Exp. Med. 193:1303. 8. Baecher-Allan, C., J. A. Brown, G. J. Freeman, and D. A. Hafler. 2001. CD4⫹CD25high regulatory cells in human peripheral blood. J. Immunol. 167: 1245. 9. Ng, W. F., P. J. Duggan, F. Ponchel, G. Matarese, G. Lombardi, A. D. Edwards, J. D. Isaacs, and R. I. Lechler. 2001. Human CD4⫹CD25⫹ cells: naturally occurring population of regulatory T cells. Blood 98:2736. 10. Dieckmann, D., C. H. Bruett, H. Ploettner, M. B. Lutz, and G. Schuler. 2002. Human CD4⫹CD25⫹ regulatory, contact-dependent T cells induce interleukin 10-producing contact-independent type 1-like regulatory T cells. J. Exp. Med. 196:247. 11. Levings, M. K., R. Sangregorio, C. Sartirana, A. L. Moschin, M Battaglie, P. C. Orban, and M.-G. Roncarolo. 2002. Human CD25⫹CD4⫹ T suppressor cell clones produce transforming growth factor , but not interleukin 10, and are distinct from type 1 regulatory cells. J. Exp. Med. 196:1335. 12. Thornton, A. M., and E. M. Shevach. 1998. CD4⫹CD25⫹ immunoregulatory T cells suppress polyclonal T cell activation in vitro by inhibiting interleukin 2 production. J. Exp. Med. 188:287. 13. Thornton, A. M., and E. M. Shevach. 2000. Suppressor effector function of CD4⫹CD25⫹ immunoregulatory T cells is antigen nonspecific. J. Immunol. 164: 183. 14. Curotto de Lafaille, M. A., and J. J. Lafaille. 2002. CD4⫹ regulatory T cells in autoimmunity and allergy. Curr. Opin. Immunol. 14:771. CD4⫹CD25⫹ REGULATORY T CELL REPERTOIRE