Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Cardiac contractility modulation wikipedia , lookup
Heart failure wikipedia , lookup
Electrocardiography wikipedia , lookup
Antihypertensive drug wikipedia , lookup
Management of acute coronary syndrome wikipedia , lookup
Mitral insufficiency wikipedia , lookup
Arrhythmogenic right ventricular dysplasia wikipedia , lookup
Coronary artery disease wikipedia , lookup
Quantium Medical Cardiac Output wikipedia , lookup
Artificial heart valve wikipedia , lookup
Lutembacher's syndrome wikipedia , lookup
Heart arrhythmia wikipedia , lookup
Dextro-Transposition of the great arteries wikipedia , lookup
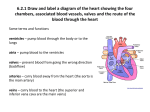
Chapter 20 Cardiovascular System: The Heart AP2 Chap. 20: Cardio Syst-Heart 1 Cardiovascular System: The Heart I. Fxns of the heart II. Size, Shape, & Location of the heart III. Anatomy of the heart IV. Route of blood flow thru the heart V. Histology VI. Electrical Properties VII. Cardiac Cycle VIII.Mean Arterial BP IX. Regulation of the heart X. Heart & Homeostasis XI. FX of aging on the heart AP2 Chap. 20: Cardio Syst-Heart 2 Cardiovascular System • Heart is actually 2 pumps: 1st pump receives O2 poor blood from the body and pumps it to the lungs – Pulmonary Circulation 2nd pump receives O2 rich blood from the lungs and pumps it to the body – Systemic Circulation Fig. 20.1 pg 679 AP2 Chap. 20: Cardio Syst-Heart 3 I. Functions of the Heart AP2 Chap. 20: Cardio Syst-Heart 4 I. Fxns of the heart 1. Generating BP (blood pressure) – Pg 680 Figure 20.2a Contractions of the ♥ generate the BP, wh/ is responsible for blood mvment thru vessels 2. Routing Blood – ♥ is the interchange between pulmonary & systemic circulation, thus insuring better oxygenation of bld going to tissues 3. Insuring One-Way blood flow – Valves of the heart are 1-way thus insuring no backflow 4. Regulating Blood Supply – As metabolic needs of the tissues D the heart can D rate & force of contraction to aid the AP2 Chap. 20: Cardio Syst-Heart tissues 5 II. Size, shape, & location of the ♥ AP2 Chap. 20: Cardio Syst-Heart 6 II. Size, shape, & location of the ♥ • ~ size of a closed fist, shaped like a blunt cone • Lies obliquely within the mediastinum with its base directed back and superior & apex coming forward inferiorly to the left. AP2 Chap. 20: Cardio Syst-Heart Front View Pg 684 Figure 20.5 a Posterior View Pg 685 Figure 20.5 c 7 III. Anatomy of the ♥ A. B. C. D. Pericardium Heart Wall External Anatomy & Coronary Circulation Heart Chambers & Valves AP2 Chap. 20: Cardio Syst-Heart 8 III. Anatomy of the heart: Pericardium • A sac surrounding the heart made of 2 layers that can also be called the pericardial sac. • It can D in size to accommodate more fluid or D in heart size 1. Fibrous Pericardium – Pg 681 Figure 20.3 Aids in holding the heart in place 2. Serous Pericardium – Reduces friction as the heart beats and is made up of 3 regions: a) Parietal Pericardium • Lies just under & Lines #1 b) Pericardial Cavity • • c) Lies between a) & c) filled with pericardial fluid Helps reduce friction as heart moves in the pericardial sac Visceral Pericardium • Lines the exterior surface of the heart 9 III. Anatomy of the Heart: Heart Wall • Has 3 main layers: 1. Epicardium • Outermost layer that protects from friction Pg 682 Figure 20.4 2. Myocardium • Middle layer responsible for contraction 3. Endocardium • • • • Atria (top chambers) – • Innermost layer & protects from friction created by flowing blood Simple squamous epi over CT Heart valves are modified Endocardium Mainly smooth w/some raised areas called pectinate muscles that are separated by smooth parts by a ridge called cristae terminalis Ventricles (bottom chambers) – Have large ridges called trabeculae carneae 10 III. Anatomy of the Heart: External Anatomy & Coronary Circulation Right Auricle Left Auricle There is also a posterior Interventricular Sulcus AP2 Chap. 20: Cardio Syst-Heart 11 III. Anatomy of the Heart: External Anatomy & Coronary Circulation These veins come from the body with O2 poor blood and empty into the right atrium + Coronary Sinus These veins come from the lungs with O2 Rich blood and empty into the left atrium. 12 III. Anatomy of the Heart: External Anatomy & Coronary Circulation These arteries exit the heart carrying O2 poor blood to the lungs This major artery exits the heart carrying O2 rich blood to the body. 13 III. Anatomy of the Heart: External Anatomy & Coronary Circulation Blood flow to the coronary blood vessels isn’t continuous. • Cardiac Muscle contracts blood vessels get compressed & blood doesn’t readily flow • Cardiac Muscle relaxes Blood vessels aren’t compressed & blood flow thru the coronary blood vessels resumes AP2 Chap. 20: Cardio Syst-Heart 14 III. Anatomy of the Heart: External Anatomy & Coronary Circulation Major Arteries (A) supplying heart tissue • Lie within the coronary sulcus & interventricular sulci. • Rt. & Lt. Coronary Arteries (CA) – Major A’s supplying blood to heart – Exit the aorta just as it leaves the heart and lie w/in the coronary sulcus – Right is smaller in diameter than left Branches of the Rt.CA • Rt. Marginal A • Supply bld to lat’l wall of the rt ventricle • Post’r Interventricular A. • Supplies bld to the posterior & inferior region of the heart Pg 685 Figure 20.6a Branches of the Lt.CA • Ant. Interventricular A – Supplies most of the ant. heart • Left Marginal A – Supplies bld to the lat. lt. ventricle • Circumflex A – supplies most of the posterior heart. 15 III. Anatomy of the Heart: External Anatomy & Coronary Circulation Major veins (V) draining the heart tissue Pg 685 Figure 20.6a • Great Cardiac V – Major vein draining the tissue on the left side of the heart • Small Cardiac Vein – Drains the right margin of the heart • Both empty into the Coronary Sinus – Empties into the right atrium AP2 Chap. 20: Cardio Syst-Heart 16 hambers & Valves III. Anatomy of the heart: Interatrial Septum • piece of tissue that separates L from R atrium • Foremen Ovale/ Fossa Ovalis • Ovale, an opening between the atria in a embryo & fetus to bypass pulmonary circulation that seals and forms the Ovalis Pg 686 Figure 20.7 Right Atrium Left Atrium – Upper R chamber – 3 openings: – Upper L chamber – 4 uniform openings: 1. Superior Vena Cava – Drains upper body 2. Inferior Vena Cava – Drians Lower Body 3. Coronary Sinus – Pulmonary Veins 1. 2. 2 from each lung Drains lungs after getting O2 Drains the Heart 17 hambers & Valves III. Anatomy of the heart: Interventricular Septum • Thick muscular piece of tissue that separates L from R ventricle • Each ventricle has 1 large, superiorly placed outflow route near midline Pg 686 Figure 20.7 Right Ventricle Left Ventricle – Lower R chamber – Opens to the pulmonary trunk – Lower L chamber – Opens to the aorta 18 Semilunar Valves • Composed of 3 pocket like semilunar cusps/flaps the free inner borders meet in the center of the arteries to block blood flow. Pulmonary Valve Between the R ventricle and the Pulmonary Trunk Aortic Valve Between L ventricle and the Aorta III. Anatomy of the heart: Chambers & Valves 19 Atrioventricular Valves – Composed of cusps/flaps allow blood to flow from atrium to the ventricles but because of design help to prevent back flow Tricuspid Valve Between the R atrium and R ventricle 3 cusps/flaps Bicuspid Valve Between the L atrium and L ventricle 2 cusps/flaps III. Anatomy of the heart: Chambers & Valves 20 Pg 687 Figure 20.9 • Blood pushing out of the ventricle causes enough pressure to push the semilunar valves open while at the same time causing the atrioventricular valves to seal with the help of the chordae tendineae and the papillary muscle. As the ventricle relaxes the semilunar valves get sucked back effectively sealing them while the atrioventricular valves open • Chordae Tendineae • Strong CT strings that connect to the cusps of AV-valves • Papillary Muscle • Cone-shaped muscular pillars, that contract when V contract & prevent flaps from protracting 21 IV. Route of blood flow thru the heart AP2 Chap. 20: Cardio Syst-Heart 22 Figure 20.10 Pg 688 AP2 Chap. 20: Cardio Syst-Heart 23 Cardiac Cycle • Arteries: • BLUE: – Carries blood away from the heart • Veins: – Deoxygenated blood • RED – Oxygenated blood – Carries blood toward the heart AP2 Chap. 20: Cardio Syst-Heart 24 Lung Tissue Body Tissue Left Atrium Right Atrium Right Ventricle Left Ventricle AP2 Chap. 20: Cardio Syst-Heart 25 Tricuspid Valve Pulmonary Semilunar Valve Bicuspid Valve Aortic Semilunar Valve AP2 Chap. 20: Cardio Syst-Heart 26 Pulmonary Arteries Coronary Arteries Inferior Vena Cava Pulmonary Veins Superior Vena Cava Coronary Sinus AP2 Chap. 20: Cardio Syst-Heart 27 Body Tissue Inferior Vena Cava Superior Vena Cava Coronary Sinus • Deoxygenated blood drains into the Right atrium via the: – The inferior vena cava drains the lower body tissue – The superior vena cava drains the upper body tissue – The coronary sinus drains the heart tissue 28 Right Atrium • The right atrium fills with deoxygenated blood AP2 Chap. 20: Cardio Syst-Heart 29 Right Atrium Tricuspid Valve • Deoxygenated blood goes from the right atrium thru the tricuspid valve into the right ventricle. 30 Right Ventricle • The right ventricle fills with deoxygenated blood 31 Pulmonary Semilunar Valve Right Ventricle • Deoxygenated blood is squeezed from the right ventricle thru the pulmonary semilunar valve into the 32 pulmonary trunk. Pulmonary Arteries Lung Tissue • The pulmonary trunk splits into the right and left pulmonary arteries carrying deoxygenated blood in to the right and left lungs respectively to pick up oxygen and drop off carbon dioxide. 33 Lung Tissue • In the lungs CO2 is exchanged for O2 AP2 Chap. 20: Cardio Syst-Heart 34 Lung Tissue Left Atrium Pulmonary Veins • The right and left pulmonary veins carry the newly oxygenated blood back to the left atrium from the right and left lungs respectively. 35 Left Atrium • The left atrium fills with freshly oxygenated blood. 36 Left Atrium Bicuspid Valve Left Ventricle • The oxygenated blood is pumped from the left atrium thru the bicuspid valve into the left ventricle. 37 Left Ventricle • The left ventricle fills with freshly oxygenated blood. 38 Aorta Aortic Semilunar Valve Left Ventricle • Oxygenated blood is squeezed from the left ventricle thru the aortic semilunar valve into the aorta. 39 Coronary Arteries Aorta Body Tissue Aortic Semilunar Valve • The aorta splits into the right and left coronary arteries carrying oxygenated blood to the heart tissue. 40 Coronary Arteries Aorta Body Tissue • Then the aorta continues to carry the oxygenated blood to the body tissues. 41 V. Histology A. Heart Skeleton B. Cardiac Muscle C. Conducting System AP2 Chap. 20: Cardio Syst-Heart 42 V. Histology: Heart Skeleton • Consists of a plate of fibrous CT that serves 3 purposes: 1. Supports both the semilunar & atrioventricular valves to insure they don’t collapse 2. Acts as electrical insulation between the atria & ventricles 3. Acts as a point of attachment for cardiac muscle AP2 Chap. 20: Cardio Syst-Heart Figure 20.11 Pg 690 43 V. Histology: Cardiac Muscle (CM) Figure 20.11 Pg 690 • CM cells joined by intercalated disks that allow action potentials to move directly from 1 cell to the next, thus cardiac muscle cells fxn as a unit – Intercalated disks are a combo of desmosomes (wh/hold cells together) & gap junctions (wh/allow for cell to cell communication) • Elongated, branching cells w/ 1 or 2 centrally located nuclei. • Like skeletal muscle actin & myosin are organized to form sarcomeres. Arrangement of both the Smooth ER & transverse tubules varies but fxns essentially the same. • CM cells have a slow onset as well as period of contraction due to Ca2+ mvmt along myofibrils. • Has a good blood supply to support aerobic respiration – ATP prod’d with: • Glucose, Fatty Acids, Lactic Acid • CM doesn’t develop O2-debt 44 V. Histology: Conducting System (CS) • Consists of modified CM-cells that form 2 nodes & a conducting bundle. (both of which are made up of small diameter cells to slow action potential) 1. SA-Node 2. AV-Node • • • SA-node initiates action potentials that spread across the atria & cause them to contract At the AV-node action potential slows allowing atria to complete contraction & ventricles to fill Next it follows along the AV bundle, Rt & Lt bundle branches & Purkinje fibers. – This causes the contraction of the ventricles from the apex of the heart toward the base SA-node AV-node AV bundle Rt & Lt Bundle braches Purkinje fibers 45 V. Histology: Conducting System (CS) • The CS of the heart consists of modified CM-cells that form 2 nodes & a conducting bundle. 1. SA-Node medial to the opening of the superior vena cava • A.k.a. Pacemaker (generates spontaneous action potentials) 2. AV-Node- medial to the tricuspid valve SA-node AV-node AV bundle Rt & Lt Bundle braches Purkinje fibers 46 VI. Electrical Properties A. Action potentials B. Autorhythmicity of cardiac muscle C. Refractory periods of cardiac muscle D. Electrocardiogram AP2 Chap. 20: Cardio Syst-Heart 47 VI. Electrical Properties • CM have a resting membrane potential (RMP) • Depends on the permeability of the PM – Low permeability to Na+ and Ca2+ – Higher permeability to K+ • Once their threshold is reached….an Action Potential results AP2 Chap. 20: Cardio Syst-Heart 48 VI. Electrical Properties: Action Potentials Permeability D’s during and action potential in CM 1. Depolarization Phase – Voltage-Gated (VG) Na+ channels open (Na+ rushes in) VG K+ channels close (K can’t get out) VG Ca2+ channels begin to open (Ca2+ goes in) – – 2. Early Repolarization & Plateau Phase – VG Na+ channels close (Na+ can’t get in) Some VG K+ channels open causing “early” repolarization – • – 3. K+ goes out in a rush VG Ca2+ channels are open, prod’ing the plateau by further slowing repolarization (Ca2+ coming in) Final Repolarization Phase – – VG Ca2+ channels close Many VG K+ channels open Action potentials in CM last longer than in SM SM 2 ms CM 200-500ms 49 VI. Electrical Properties: Action Potentials • Gap junctions w/in intercalated disks do allow action potentials to transfer between CM-cells, but they do slow the rate of the action potential between them. • Calcium-induced calcium release (CICR) – Movement of the Ca2+ into the cell stimulates the release of Ca2+ from the sarcoplasmic reticulum • Ca2+ binding facilitates the interaction between actin & myosin to produce the contraction of CM. AP2 Chap. 20: Cardio Syst-Heart 50 VI. Electrical Properties: Autorhythmicity of the heart • Autorhythmicity means at regular intervals it is selfstimulating • SA-node’s pacemaker cells generate action potentials spontaneously & @ regular intervals. – This is the initial step toward full heart contraction. – Prepotential is the beginning of the spontaneously developing local potential in the pacemaker cells • Unlike other CM-cells, Ca2+ is primarily responsible for the depolarization phase in pacemaker cells. • Even with the SA-node setting the rhythm of the heart there are some other CM-cells that can generate spontaneous AP’s, the SA node is just quicker than the others thus setting the pace. These other regions are called Ectopic Focuses. – Ex/ AV-bundle – Artificial EF’s can be created by changing the CM-cell membrane’s permeability 51 VI. Electrical Properties Refractory periods of CM • Time it takes to begin another AP. – Absolute – Relative • CM has a prolonged depolarization & thus a prolonged RP. This allows time for cardiac muscle to relax b4 the next action potential causes a contraction. Electrocardiogram • Records the electrical activities of the heart. • Can be used as a diagnostic tool. • P-wave Depolarization of atria • QRS-wave Depolarization ventricles (AV-node R&L bindle branches, & Purkinje fibers) • T-wave repolarization of ventricles 52 VII. Cardiac Cycle •Repetitive pumping process that begins w/the onset of CM contraction and ends with the A. Events occurring during ventricular systole B. Events occurring during ventricular diastole C. Heart Sounds D. Aortic Pressure Curve AP2 Chap. 20: Cardio Syst-Heart 53 VII. Cardiac Cycle Heart: 2 separate circuits in the same organ RIGHT SIDE O2 poor blood from body R Atrium Tricuspid Valve R Ventricle Pulmonary Valve Lungs for O2 pick-up LEFT SIDE O2 rich blood from lungs L Atrium Bicuspid Valve L Ventricle Aortic Valve Body to drop off O2 & pick-up CO2 The Atria Each atria can be considered a primer pumps The Ventricles Each Ventricle can be considered a power pumps Produce major force causing blood to flow thru pulmonary & systemic arteries (respectively) Movement from High to Low pressure 54 – Ventricular systole – Atrial systole • Diastole: to dilate – Ventricular diastole – Atrial diastole • Without “reference” to V or A. It is referring to V only AP2 Chap. 20: Cardio Syst-Heart V. Diastole A. Systole • Time frame between cycles can vary widely from 0.25s in newborns to 1s or more in well trained athletes • Systole: to contract V. Systole VII. Cardiac Cycle 55 • Period of isovolumic contraction • Period of ejection – Once the V’s have enough pressure to cause the semilunar valves of the aorta and pulmonary arteries to open pushing the blood through (Pressure in V’s is greater than in the Pulmonary trunk or aorta) • Period of isovolumic relaxation – As V’s relax pressure w/in decreases below that in the pulmonary trunk & aorta causing the blood to flow back toward the V’s wh/causes the semilunar valves to close. When the valves close all valves are closed and no blood flows into relaxing V’s VII. Cardiac Cycle – Brief interval in which the V’s (filled with blood) begin to contract but no movement of blood occurs because the pressure isn’t yet great enough to open the valves 56 VII. Cardiac Cycle: 5 periods 1. Period of Isovolumic Contraction: heart is contracting but vol isn’t Ding b/c valves are not open 2. Period of Ejection: semilunar valves open & blood is ejected 3. Period of Isovolumic Relaxation: heart muscle is relaxing but vol doesn’t D b/c no valves are open 4. Passive Ventricular Filling when blood flows from higher pressure in veins & atria into the lower pressured relaxed ventricles 5. Active Ventricular Filling results when atria contract & pump blood into the ventricles AP2 Chap. 20: Cardio Syst-Heart 57 Figure 20.18 pg 698 58 VII. Cardiac Cycle: Events of: Ventricular Systole • Contraction of V closes AV valves, opens semilunar valves, & ejects blood from the heart • End diastolic volume: vol of bld just b4 it contracts • End Systolic Volume: vol of bld after contraction Ventricular Diastole • • • Relaxation of the V results in closing of the semilunar valves, opens the AV valves, & movement of bld into V Most bld mvmt occurs when bld moves from higher pressure in veins & atria to the lower pressure (sucking) relaxing V’s Contraction of the Atria completes filling Heart Sounds • 1st Sound: “Lubb” Closure of the AV Valves • 2nd Sound “Dupp” Close of the Semilunar Valves • Possible 3rd sound Turbulent blood flow 59 VIII. Mean Arterial Blood Pressure AP2 Chap. 20: Cardio Syst-Heart 60 VIII. Mean Arterial Blood Pressure (MAP) • Ave. bld pressure in the aorta MAP= CO X PR • Cardiac Output (CO) amount of bld pumped thru the heart per minute – CO= heart rate X stroke volume – Stroke Volume is the amount of bld pumped thru the heart per beat • Equal to ( end-diastolic volume – end-systolic volume) • This can D based on 2 things – Venus return (amount of bld coming into heart) increases SV – Increased ventricular contraction can increase SV • Peripheral Resistance (PR) total resistance to bld flow thru bld vessels • Cardiac reserve difference btwn resting & exercising CO 61 Figure 20.21 Factors affecting MAP pg 704 AP2 Chap. 20: Cardio Syst-Heart 62 IX. Regulation of the Heart A. Intrinsic Regulation B. Extrinsic Regulation AP2 Chap. 20: Cardio Syst-Heart 63 IX. Regulation of the heart To maintain homeostasis, the amount of blood pumped by the heart must vary dramatically • Intrinsic Regulation: – Results from normal fxnal characteristics of the heart – Doesn’t depend on neuronal or hormonal regulation • Extrinsic Regulation: – Involves neural & hormonal control – Neural: sympathetic & parasympathetic reflexes – Hormonal: epi & norepi from the adrenal medulla AP2 Chap. 20: Cardio Syst-Heart 64 IX. Regulation of the heart Intrinsic Regulation • As venous return increases, end-diastolic volume increases. The greater the end-diastolic volume, the greater the stretch on the ventricular walls. • Preload extent to wh/ventricular walls are stretched • Cardiac muscle exhibits a length vs. tension relationship. Meaning the longer it gets the more power it contracts with. • Venous Return: – amount of bld returning to heart @ each cardiac cycle • Starlings law of the heart – Increased Preload causes the CM-fibers to contract w/greater force & prod a greater stroke volume – Afterload- pressure the contracting ventricles must overcome to move bld. 65 IX. Regulation of the heart Extrinsic Regulation Nervous System Control • Cardioregulatory center of the medulla oblongata regulates the parasympathetic & sympathetic nervous control of the heart – PNS • Supplied by the vegus nerve • Postganglionic neurons secrete Ach increases membrane permeability to K+ hyperpolarizes the membrane slows down action potentials decreases heart rate – SNS • Supplied by cardiac nerves • Postganglionic neurons secrete norepi increases membrane permeability to Na & Ca depolarization of the membrane speeds up action potentials increases heart rate & force of contraction Hormonal Control • Epi & Norepi get released from the adrenal medulla into bld as a result of SNS stimulation – Long lasting FX compared to NS stimulation – Increases the rate & force of CM contraction. 66 X. Heart & Homeostasis A. Effect of BP B. Effect of pH, CO2, & O2 C. Effect of Extracellular Ion [ ] D. Effect of Body Temperature AP2 Chap. 20: Cardio Syst-Heart 67 X. Heart & Homeostasis Pumping efficiency of the heart plays an important role in the maintenance of homeostasis. BP in systemic circulation must be maintained at a level high enough to achieve any XD that must occur. And conditions of metabolic activity may D thanks to exercise & rest FX of BP FX of Extracellular ion [ ] • Baroreceptors are those that monitor BP (Stretch receptors) • Decrease in BP baroreceptor reflexes increase SNS stimulation & decrease PNS stimulation of heart. increase in heart rate & force of contraction • Increase or decrease in extracellular K decrease in heart rate • Increase in extracellular Ca increased force of contraction & decrease heart rate – Decreased Ca opposite FX FX of Body Temperature • Increase in body temp increase in heart rate • Decrease in body temp decrease in heart rate 68 Fig 20.23 Pg 708 AP2 Chap. 20: Cardio Syst-Heart 69 X. Heart & Homeostasis FX of pH, CO2, & O2 Chemoreceptors (CR) monitor blood pH, CO2, and O2 Response: • All regulatory mechanisms fxning • Medullary CR reflexes together respond to: – CO2 & pH • SNS & PNS stimulation of the heart • Carotid body CR reflex – Stimulated by O2 levels • Decreased heart rate & vasoconstriction – blood pH – blood CO2 levels – blood O2 levels • Produce an increase in heart rate & vasoconstriction • Lowered O2 increases respiratory rate wh/ activates the SNS stimulation of the heart AP2 Chap. 20: Cardio Syst-Heart 70 Fig 20.24 Pg 709 AP2 Chap. 20: Cardio Syst-Heart 71 XI. FX of Aging of the heart AP2 Chap. 20: Cardio Syst-Heart 72 XI. FX of Aging of the heart • Aging results in gradual changes to the heart that are mostly seen when exercising • Abnormal enlargement (Hypertrophy) of the L. ventricle is common • Max Heart rate may decrease • Increase in abnormal valve fxn & arrhythmia • Increased O2 consumption, req’d to pump same amount of bld, make age-related coronary artery disease more severe • Exercise improves fxnal capacity of heart at all ages AP2 Chap. 20: Cardio Syst-Heart 73