Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Gene regulatory network wikipedia , lookup
Lipid signaling wikipedia , lookup
Evolution of metal ions in biological systems wikipedia , lookup
Specialized pro-resolving mediators wikipedia , lookup
Butyric acid wikipedia , lookup
Biosynthesis wikipedia , lookup
Point mutation wikipedia , lookup
Amino acid synthesis wikipedia , lookup
Biochemistry wikipedia , lookup
Glyceroneogenesis wikipedia , lookup
Citric acid cycle wikipedia , lookup
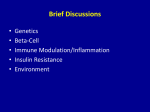
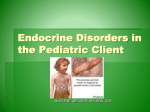
The Glucose/Fatty Acid Cycle 1963–2003 Short-chain 3-hydroxyacyl-CoA dehydrogenase deficiency associated with hyperinsulinism: a novel glucose–fatty acid cycle? S. Eaton*†1 , I. Chatziandreou*, S. Krywawych†, S. Pen*, P.T. Clayton† and K. Hussain† *Department of Paediatric Surgery, Institute of Child Health, 30 Guilford Street, London WC1N 1EH, U.K., and †Department of Biochemistry, Endocrinology and Metabolism, Institute of Child Health, 30 Guilford Street, London WC1N 1EH, U.K. Abstract Hyperinsulinism of infancy is caused by inappropriate insulin secretion in pancreatic β-cells, even when blood glucose is low. Several molecular defects are known to cause hyperinsulinism of infancy, such as KATP channelopathies and regulatory defects of glucokinase and glutamate dehydrogenase. Although defects of fatty acid oxidation have not previously been known to cause hyperinsulinism, patients with deficiency in SCHAD (short-chain 3-hydroxyacyl-CoA dehydrogenase; an enzyme of mitochondrial β-oxidation) have hyperinsulinism. A novel link between fatty acid oxidation and insulin secretion may explain hyperinsulinism in these patients. Introduction SCHAD (short-chain L-3-hydroxyacyl-CoA dehydrogenase; EC 1.1.1.35) catalyses the NAD+ -dependent conversion of L-3-hydroxyacyl-CoA to 3-ketoacyl-CoA in mitochondrial fatty acid β-oxidation. The Schad gene is expressed in most tissues including the pancreas [1] but SCHAD activity is particularly high in the islets of Langerhans, suggesting that SCHAD and the regulation of fat oxidation may have an important function in the β-cell [2,3]. Deficiency of one of the enzymes of mitochondrial β-oxidation typically produces hypoglycaemia with elevated plasma concentrations of nonesterified fatty acids and low plasma concentrations of ketone bodies (high non-esterified fatty acids/D-3-hydroxybutyrate ratio) [4]. Deficiency of SCHAD activity has been described but none of these cases has been shown to have mutations in the Schad gene [5]. Apart from fatty acid oxidation defects, the main cause of hypoketotic hypoglycaemia in infancy and childhood is hyperinsulinism. So far mutations in four different genes have been identified as causing hyperinsulinism. These are gain-of-function mutations of the enzymes glucokinase and glutamate dehydrogenase and defects in the genes encoding the SUR1 or KIR6.2 subunits of the KATP channel in the β-cell membrane [6]. In these disorders, the pathogenesis of the hyperinsulinism can be explained using a simple model of β-cell signalling: increased β-cell glucose metabolism leads to increased ATP production from acetyl-CoA in the citric acid cycle and a rise in the ATP/ ADP ratio. This leads in turn to opening of potassium channels, depolarization of the cell membrane and calcium influx through voltage-gated calcium channels, which finally triggers insulin secretion (Figure 1). The defects causing Key words: β-oxidation, carnitine palmitoyltransferase I (CPT I), 3-hydroxyacyl-CoA dehydrogenase, hyperinsulinism. Abbreviations used: SCHAD, short-chain l-3-hydroxyacyl-CoA dehydrogenase; CPT I, outer membrane carnitine palmitoyltransferase I; LCFA-CoA, long-chain fatty-acyl-CoA. To whom correspondence should be addressed (e-mail [email protected]). 1 hyperinsulinism increase ATP production (increased metabolism of glucose or glutamate) or they cause permanent depolarization. SCHAD deficiency associated with mutations in the Schad gene We recently described a child who presented with non-ketotic hypoglycaemia with significant plasma insulin at the time of hypoglycaemia [7]. This child had hydroxybutyrylcarnitine in blood, suggesting that SCHAD enzyme activity could be defective. This proved to be the case: fibroblast SCHAD activity was low, there was no SCHAD immunoreactive protein and a homozygous point mutation in the Schad gene was found [7]. We have subsequently diagnosed another child with a similar clinical and biochemical phenotype (K. Hussain, P.T. Clayton, S. Krywawych, I. Chatziandreou and S. Eaton, unpublished work), and another family that was originally reported to have glucagon deficiency has since been found to have hyperinsulinaemic hypoglycaemia associated with a homozygous point mutation in the Schad gene [8–10]. Hence, it appears that SCHAD deficiency associated with mutations in the Schad gene may be a rare but consistent cause of hyperinsulinism. Fatty acid oxidation disorders are frequently characterized by non-ketotic hypoglycaemia, associated with a variety of other symptoms such as cardiomyopathy, myopathy and retinopathy; however, hyperinsulinism has never been associated with any known fatty acid oxidation disorder [5], so it is of importance to determine the biochemical basis for hyperinsulinism in these patients. The anaplerotic/lipid signalling pathway for augmentation of insulin secretion Fatty acids are a major energy source for unstimulated islets [11]. An early metabolic event caused by glucose is a shift C 2003 Biochemical Society 1137 1138 Biochemical Society Transactions (2003) Volume 31, part 6 Figure 1 Pancreatic β-cell insulin secretion indicating KATP -channel-dependent insulin secretion (solid arrows) and augmentation/anaplerosis pathway (dashed arrows) from fatty acids to glucose as fuel. It has been proposed that, as in other tissues, this occurs in the β-cell through conversion of glucose, via pyruvate carboxylase, oxaloacetate, citrate and acetyl-CoA, to malonyl-CoA which, by inhibiting CPT I (outer membrane carnitine palmitoyltransferase I), blocks the entry of long-chain fatty-acyl CoA (LCFA-CoA) into the mitochondrion (Figure 1). Thus LCFA-CoA is converted instead into diacylglycerol, triacylglycerols and fatty acids; it can also be used for protein acylation. LCFA-CoA or the complex lipids derived from it are potent regulators of enzymes, ion channels and various signal-transducing effectors that could thus augment insulin secretion by a KATP independent mechanism [12]. In addition to malonyl-CoA, other short-chain acyl-CoA esters such as methylmalonylCoA, succinyl-CoA and acetyl-CoA can inhibit CPT I [13]. We hypothesized that L-3-hydroxybutyryl-CoA accumulating in the cytosol, originating either from circulating L-β-hydroxybutyrate/L-β-hydroxybutyryl-carnitine or from export of L-3-hydroxybutyryl-CoA accumulating within pancreatic β-cell mitochondria, inhibits CPT I and thereby triggers insulin secretion via the augmentation/lipid signalling pathway (Figure 2). However, this would require a cytosolically active carnitine acetyltransferase, which does not appear to be present [14], or a cytosolic short-chain acyl-CoA synthase active towards L-3-hydroxybutyrate, and preliminary evidence suggests that CPT I is not sensitive to inhibition by L-3-hydroxybutyryl-CoA (S. Pen and S. C 2003 Biochemical Society Eaton, unpublished work). In addition, deficiency of L-CPT I (liver isoform of CPT I) is not known to cause hyperinsulinism [5]. Other hypotheses for insulin secretion in SCHAD deficiency There are several other potential mechanisms for insulin secretion in SCHAD deficiency. They include the following. (i) The physiological ketone body, D-hydroxybutyrate, stimulates insulin secretion [15] and it is possible that the mechanism that causes D-hydroxybutyrate to stimulate insulin secretion is more sensitive to L-hydroxybutyrate compared with D-hydroxybutyrate. However, this explanation is unlikely because insulin secretion was lower from DLhydroxybutyrate than D-hydroxybutyrate [15]. (ii) The α-ketoglutarate dehydrogenase/α-ketoglutarate–glutamate dehydrogenase–glutamate axis is thought to be important in the control of the anaplerosis/augmentation pathway [16] and intramitochondrial L-3-hydroxybutyryl-CoA could interfere with this pathway, e.g. by inhibition of α-ketoglutarate dehydrogenase. (iii) L-Hydroxybutyrate, L-hydroxybutyryl-CoA or L-hydroxybutyryl-carnitine could inhibit KATP channels, thus triggering insulin secretion. However, long-chain acyl-CoA esters are activators rather than inhibitors of KATP channels [17]. (iv) L-Hydroxybutyrate, Lhydroxybutyryl-CoA or L-hydroxybutyryl-carnitine could The Glucose/Fatty Acid Cycle 1963–2003 Figure 2 Potential pathways by which l-hydroxybutyrate or a metabolite could trigger insulin secretion via inhibition of CPT I l-β-OHB-carnitine, l-β-hydroxybutyryl-carnitine; l-β-OHB-CoA, l-β-hydroxybutyryl-CoA; CAT, carnitine acetyltransferase. trigger insulin secretion via the recently described G-proteincoupled receptor GPR40 [18]. (v) SCHAD deficiency causes modulation of other genes associated with the insulinsecretion apparatus and thus triggers insulin secretion. These possibilities are difficult to assess, at least in part because there are no defined inhibitors of SCHAD activity. Conclusions SCHAD deficiency associated with mutations in the Schad gene is a potential cause of hyperinsulinism. The molecular basis of hyperinsulinism in these patients may provide insight into a novel glucose–fatty acid cycle. The Science Development Initiative of Great Ormond Street Hospital/ Institute of Child Health are thanked for support. References 1 Vredendaal, P.J., van den Berg, I.E., Malingre, H.E., Stroobants, A.K., Olde, W.D. and Berger, R. (1996) Biochem. Biophys. Res. Commun. 223, 718–723 2 Ågren, A., Borg, K., Brolin, S.E., Carlman, J. and Lundqvist, G. (1977) Diabete Metab. 3, 169–172 3 Hammar, H. and Berne, C. (1970) Diabetologia 6, 526–528 4 Eaton, S. (2002) Prog. Lipid Res. 41, 197–239 5 Rinaldo, P., Matern, D. and Bennett, M.J. (2002) Annu. Rev. Physiol. 64, 477–502 6 Hussain, K. and Aynsley-Green, A. (2003) Int. J. Biochem. Cell Biol. 35, 1312–1317 7 Clayton, P.T., Eaton, S., Aynsley-Green, A., Edginton, M., Hussain, K., Krywawych, S., Datta, V., Malingre, H.E.M., Berger, R. and van den Berg, I.E.T. (2001) J. Clin. Invest. 108, 457–465 8 Molven, A., Rishaug, U., Matre, G.E., Njølstad, P.R. and Søvik, O. (2002) Am. J. Med. Genet. 113, 40–46 9 Vidnes, J. and Øyasaeter, S. (1977) Pediatr. Res. 11, 943–949 10 Søvik, O., Matre, G.E., Rishaug, U., Njølstad, P.R. and Molven, A. (2002) J. Inherit. Metab. Dis. 25, 63A 11 Berne, C. (1975) Biochem. J. 152, 661–666 12 Prentki, M., Joly, E., El Assaad, W. and Roduit, R. (2002) Diabetes 51, S405–S413 13 Kashfi, K., Mynatt, R.L. and Cook, G.A. (1994) Biochim. Biophys. Acta 1212, 245–252 14 Poirier, M., Vincent, G., Reszko, A.E., Bouchard, B., Kelleher, J.K., Brunengraber, H. and Des Rosiers, C. (2002) Am. J. Physiol. Heart Circ. Physiol. 283, H1379–H1386 15 Biden, T.J. and Taylor, K.W. (1983) Biochem. J. 212, 371–377 16 Maechler, P. (2002) Cell. Mol. Life Sci. 59, 1803–1818 17 Branstrom, R., Leibiger, I.B., Leibiger, B., Corkey, B.E., Berggren, P.O. and Larsson, O. (1998) J. Biol. Chem. 273, 31395–31400 18 Itoh, Y., Kawamata, Y., Harada, M., Kobayashi, M., Fujii, R., Fukusumi, S., Ogi, K., Hosoya, M., Tanaka, Y., Uejima, H. et al. (2003) Nature (London) 422, 173–176 Received 1 July 2003 C 2003 Biochemical Society 1139