Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Persistent vegetative state wikipedia , lookup
Neuroanatomy wikipedia , lookup
National Institute of Neurological Disorders and Stroke wikipedia , lookup
Haemodynamic response wikipedia , lookup
Visual selective attention in dementia wikipedia , lookup
Neuropsychopharmacology wikipedia , lookup
Aging brain wikipedia , lookup
Alzheimer's disease wikipedia , lookup
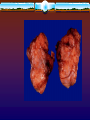
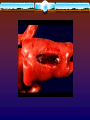
NEUROLOGY PICTURES CHALLENGE Danil Hammoudi.MD SINOE MEDICAL ASSOCIATION Glioblastoma Multiforme Etiology: • The exact etiology is not known but has to do with several mutations in protooncogenes and tumor suppressor genes. • Some appear as a part of several hereditary syndromes such as neurofibromatosis or Turcot's syndrome. Pathogenesis: • The cause of the glioblastoma or any brain tumor is not known but changes or loss of chromosome 17 and inactivation of a tumor suppressor gene, p53, play a role. Thus far, we do not know what precipitates these changes. Epidemiology: • Glioblastomas are the most comman primary brain tumor. • They account for 50% of all gliomas and arise after age 50 in most patients. • Younger patients tend to have a better prognosis than the elderly. • Radiation and chemotherapy appear to extend the life of the patient. General Gross Description: • The glioblastoma multiforme has a multiform or variable appearance with evidence of old and recent hemorrhage (yellowish-brown to red), necrosis and areas of firm tissue. • Usually the glioblastoma is seen as a mass lesion involving a focal area although it may cross the corpus callosum to the other hemisphere or be multifocal. General Microscopic Description: • Microscopically the glioblastoma has many forms as well. • Is a highly cellular tumor with pleomorphic, basophilic nuclei with indistinct cytoplasmic borders or plump pink cytoplasm and a delicate fibrillary background. • Mitoses,necrosis, and capillary endothelial proliferation are common. Clinical Correlations: • The clinical appearance of the glioblastoma is typical for brain tumors in general with a slowly progressive neurological deficit of a focal nature, that is, a slowly progressive hemiparesis of one side of the body. • Prognosis is poor, in that, patients live only 6 month to a year after diagnosis Recent Infarct Etiology: • Cerebral infarcts are due to occlusion of an artery by a thrombus or embolus effectively cutting off nutrients and oxygen to the area fed by the artery. Pathogenesis: • The most comman cause of cerebral infarct is due to atherosclerosis of cerebral and coronary arteries which is related to age, smoking, hypertension, serum lipids and cholesterol, and diabetes. Epidemiology: • Stroke is a common cause of death and disablility in patients over 55 but can be seen younger individuals as well. General Gross Description: • The brain shows tannish discoloration and swelling as well as softening in the area of the pale infarct. • In the hemorrhagic infarct, the grey matter will show multiple petechial hemmorrhages in the area affected. General Microscopic Description: • Microscopically, the cerebral grey and white matter in the affected area will be pale show vacuolization at the border between the infarct and intact tissue. • Within the first 24 hours, a few neutrophils will appear. • Within three days, macrophages will appear to phagocytose necrotic tissue and there will be swelling or reactive change in astrocytes at the border of the infarct as if to wall it off. Clinical Correlations: • Patients with a cerebral infarct (stroke) will have the sudden onset of focal neurological deficit such as a hemiparesis which gets somewhat worse with the accompanying edema and then stabilizes, unless there has been a massive stroke with edema, herniation and death. • After beginning resolution of the infarct, the patients neurological deficit may improve. Meningioma Etiology: • Meningiomas arise from arachnoid cells. • Their cause is not known but occasionally they arise at sites of trauma or irradiation or in some hereditary tumor diatheses such as neurofibromatosis. Pathogenesis: • The tumor grows from arachnoid cells when there has been loss of tumor suppressor genes and activation of protooncogenes. • Why these changes occur is not known. Epidemiology: • Meningiomas make up 15 - 20% of all intracranial tumors. • They are more comman in women than men, probably related to their tendency to have estrogen and progesterone receptors. • They are the only truly benign tumor in that they usually do not recur after complete surgical removal. General Gross Description: • Meningiomas have a smooth bosselated external surface which is usually pink-tan in color. • Cut surface shows a firm, tan tumor mass with fasicles that tend to whorl and stream. • These tumors may invade the dura but normally do not invade the brain or show necrosis. • The brain is compressed beneath the tumor. General Microscopic Description: • Microscopically, meningiomas are made up of plump spindle or polygonal cells which in some areas tend to form lobules, in others, fasicles of cells tend to stream and form small whorls. • Psammoma bodies (round calcifications) are often present but mitoses and necrosis are uncommon. Clinical Correlations: • Patients usually have the slow onset of focal neurological signs, occasionally with seizures. • Complete removal of the tumor is usually curative. Alzheimer's Disease Etiology: • Familial types are known but most cases are sporadic. Pathogenesis: • The cause of Alzheimer's disease is unknown. • May be due to deposition of amyloid in the parenchyma of the brain which is toxic to neurons and oligodendroglia. • An alternative hypothesis is that deposition of amyloid is a secondary effect. The amyloid deposition is thought to be due to an abnormality in the amyloid precursor protein. Epidemiology: • Senile dementia is seen in over 32% of the population over 85 years and increases rapidly after that. • Alzheimer's disease is the most common senile dementia in patients greater than 65 years old. Alzheimer's disease is seen before 65 years of age and is called presenile dementia. Most familial cases are presenile. • Since the 85 years of age and older group is increasing rapidly, Alzheimer' disease is becoming an important disease. General Gross Description: • Generally atrophied with large ventricles. General Microscopic Description: • Alzheimer's disease is characterized by the formation of round senile plaques often with an amyloid center in the neuropil of the cerebral cortex as well as neurofibrillary tangles within neurons. • The diagnosis is made by counting the number of senile plaques per 20x field and the number of neurofibrillary tangles in the same area, using the Bielschowsky stain. Clinical Correlations: • Alzheimer's disease is a devastating disease causing loss of recent memory, followed by old memories and apraxias or inability to carry out a normal procedure such as dressing, eating etc. The patient is finally bedridden with many neurological signs and usually dies of pneumonia, heart attack, or stroke. • Lifespan with the disease is usually 5 Years after diagnosis but may be 10 years if the patient is otherwise healthy. Toward the end the patient is unable to recognize anyone and may become hostile. Spinal Bifida Etiology: • Spina bifida is due to failure of the posterior neural tube to close properly during fetal life. Pathogenesis: • Spina bifida is due to a number reasons not all of which are known. Some of the known ones include folic acid deficiency, obesity, and Hypervitaminosis A. Epidemiology: • As in other neural tube defects, spina bifida is a sporadic disease seen in 1:1000 live births in the United States. • In further pregnancies, if the patient has one infant with a neural tube defect, her chance of having another affected infant is 1:50 and with a third pregnancy if the second infant manifests the defect her chance of another affected infant is 1:25. General Gross Description: • Spina bifida is an abnormality of development of the spinal cord which takes several forms. • The least severe form is spina bifida occulta in which the vertebral arches do not form in the lumbar area but the spinal cord is relatively normal. • The next most severe form is the meningocoele in which the meninges are in a skin covered sac but the cord is relativesly normal. • In the meningomyelocoele an abnormal spinal cord is present in a skin covered sac often but not always in the lumbar area. • In rachischsis much the spinal cord which is abnormal is open and covered by skin or meninges only. • In some cases the cord may be bifed, that is divided or there may be diplomyelia or a double cord. General Microscopic Description: • In spinal bifida occulta and the meningocoele, the spinal cord and meninges may be relatively normal. • In the meningomyelocoele, the cord is made up of a jumbled mass of vascular meninges with islands of neuronal-glial tissue. • Microscopically, the cord and meninges in rachischisis appear as a jumbled mass of vascular meninges and glial neuronal islands just as in the meningomyelocoele. Clinical Correlations: • The clinical symptoms depend on the severity of the spinal cord lesion. Often patients with spina bifida occulta have no symptoms but may have a lumbar dimple or lipoma. • Patients with lumbar meningomyelocoele have loss of function of lower extremities and may also have bowel and bladder dysfunction. • Patients with rachischisis rarely live. • Many patients with more severe forms of spina bifida have Arnold Chiari malformation of the cerebellum Astrocytoma Etiology: • Astrocytomas of all grades have been associated with cranial therapeutic irradiation, exposure to pesticides, and N-Nitroso compounds. • Endogenous mutations caused by these agents or other causes act to produce astrocytomas. Pathogenesis: • Astrocytomas of any type and at any age are infiltrative tumors that act as mass lesions wherever they are found and cause symptoms related to the area which they infiltrate. • If untreated and even if treated (except in the case of pilocytic astrocytoma), astrocytomas are an important cause of death. Death is due to transtentorial herniation from the expanding mass lesion. Epidemiology: • Astrocytomas make up 60% of brain tumors. • There are 7-10 cases per 100,000 population discovered per year. • Grade I astrocytomas (pilocytic Astrocytomas) are seen in the cerebellum, brainstem and optic nerves of children. • Grade II astrocytomas are seen in the cerebral hemispheres of 20-40 year old individuals and high grade astrocytomas which are most malignant in their course seen in patients in their 50's and 60's. General Grossare Description: • Low grade astrocytomas appear as greyish white areas in the cerebral or cerebellar hemisphere that tend to "erase" normal structures and enlarge the area in which they arise. • Sometimes, they are associated with cysts. • High grade astrocytomas such as the glioblastoma multiforme are multiform in their appearance being firm to necrotic and yellow, grey , brown and/or hemorrhagic. General Microscopic Description: • The low grade astrocytomas have mainly oval pale nuclei with indistinct cytoplasmic borders and fibrillary processes with only mild pleomorphism. • Pilocytic astrocytomas are spindle shaped with numerous collections of reddish astrocytic fibers called Rosenthal fibers. • The higher the grade, the more cellular, the more pleomorphic and the more basophilic the tumor cell nuclei become. • In the glioblastoma very pleomorphic and basophilic nuclei are seen as are necrosis, mitotic figures and capillary endothelial proliferation. Clinical Correlations: •Astrocytomas act as progressive mass lesions of the brain parenchyma causing progressive loss of function in the areas invaded. • Invasion of the motor strip or tract causes hemiparesis followed be hemiplegia. • Invasion of the speech areas cause aphasia etc. • If the cerebral cortex is involved there may be seizures. In children with cerebellar lesions there is ataxia and partial obstruction of the fourth ventricle with increased intracranial pressure causing nausea, vomiting, lethargy and headache. • Cerebral lesions also lead to increased intracranial pressure by their mass effect. Atrophy Etiology: • Cerebral atrophy, that is, widening of the sulci and narrowing of the gyri, can be seen after many types of damage to the brain such as chronic HIV infection, ischemic infarcts, and old trauma. • It can also be seen with aging, degenerative diseases such as Alzheimer's disease and multiple sclerosis and chronic disease. • Dilatation of the ventricles accompany the gyral changes. Pathogenesis: • The pathogenesis of atrophy is loss of neurons and astrocytosis in the cortex and other structures along with other signs of aging or ongoing disease. Epidemiology: • Cerebral atrophy is common in aging as with chronic diseases. • Almost everyone will develop it as they go through life. General Gross Description: • In ceebral atrophy there is widening of the sulci and narrowing of the gyri as well as enlargement of the lateral ventricles. General Microscopic Description: • Microscopic finding will be loss of neurons and astrocytosis as well as findings of the accompanying disease such as senile plagues and neurofibrillary tangles in Alzheimer's disease or white matter plaques in multiple sclerosis. Clinical Correlations: • Cerebral atrophy of mild to moderate degree may have no clinical signs although severe atrophy is usually seen in patients with dementia