Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
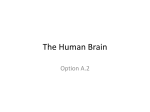
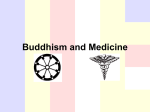
Advances in Heart Failure Mind-Body Medicine in Chronic Heart Failure A Translational Science Challenge Sitaramesh Emani, MD; Philip F. Binkley, MD, MPH T patients with congestive heart failure. Does the current value or future potential of heart/brain medicine in fact justify the creation of a new transdisciplinary and translational scientific field of study and realm of clinical practice? Downloaded from http://circheartfailure.ahajournals.org/ by guest on June 15, 2017 he connection between the mind and body has often been regarded by Western medicine as something ascribed to the mystical and a topic residing outside the scope of scientific thought. However, it has been a long-term integral tenet in the medical practice of many other cultures.1 It could be argued that the reliance of Western thought on the concept of dualism in which Plato, Aristotle, and other classical philosophers separated the body as a physical entity from the mind as a “spiritual” force has ultimately discouraged health care professionals from serious consideration of what has appeared to be a vague and even mysterious connection between the mind and body.2 Nevertheless, a growing body of research has progressively identified the mechanistic building blocks that demystify the reciprocal mind-body interaction and show that it is clearly a physical rather than mystical connection. Descriptions of neurovisceral changes in which readily demonstrated structural alterations in the brain, heart, and other organ systems arise in response to stress and a variety of emotional states provide further demonstration of the true organic mind-body connection. Perhaps the most abundant mechanistic data pertain to the brain-heart interaction under both conditions of health and a variety of cardiovascular disease states. The increasing body of evidence for these important interactions has in fact led to the call for dedicated integrated fields such as neurocardiology or behavioral cardiology.3–5 It is therefore important to examine the current state of our understanding of mind-body interactions including the experimental evidence identifying the physiological basis for these interactions and their impact on clinical outcomes. As will be shown, there is a significant overlap between the pathophysiologic mechanisms of congestive heart failure and the major effectors of mind-body connections. This provides the basis for potential new therapies that incorporate mind-body medicine. However, it must be determined whether our current understanding of the mechanisms governing mind-body interactions is sufficient to proceed with routine application of mind-body therapies in patients with heart failure. Further, are patients with heart failure amenable to interventions that act on the “heart-mind” axis in the same way as those without heart failure? This review will examine this understanding in an effort to determine whether current evidence justifies incorporation of mind-body medicine in the treatment of The Mechanistic Building Blocks Governing Mind-Heart Interactions The Autonomic Nervous System The autonomic nervous system is probably the earliest and most closely studied effector limb of the mind-heart interaction. As early as 1915, Eppinger and Hess3 proposed that behaviors may differ between individuals because of a predominance of sympathetic or parasympathetic activity. This predominance determined the physiological as well as behavioral responses to environmental stimuli and could predispose individuals to disease states such as hypertension or asthma. As discussed in excellent reviews by Samuels,5,6 the impact of stress and intense emotion on cardiovascular function was submitted to credible scientific thought and investigation in 1942 by Walter Cannon7 in a report reviewing what has been called “Voodoo Death.” This report described episodes of sudden death recounted from a variety of cultures which were apparently secondary to profound fear or emotion often inspired by superstitious beliefs. Cannon speculated that death resulted from enhanced sympathetic nervous system and adrenal responses to intense emotional stress and a belief in a power over which the victim had no control. The events discussed in his article are in fact early descriptions of what has come to be known as sudden unexpected death, and a myriad of evidence has supported the major role of the sympathetic nervous system in mediating these episodes.5,6 Foundation evidence for the role of the autonomic nervous system in stress-induced sudden cardiac death has been provided by a variety of animal models. A wide range of stressors have been shown to be associated with sudden death.5,8,9 In general, interventions that interrupt release of intracardiac but not circulating norepinephrine prevent stressinduced sudden death. Autonomically mediated mind-body interactions constitute one of the fundamental links between emotional states and cardiovascular disease in human beings.9 –11 Perhaps the most Received March 11, 2010; accepted August 16, 2010. From The Ohio State University Division of Cardiovascular Medicine and the Dorothy Davis Heart and Lung Research Institute, Columbus, Ohio. Correspondence to Philip F. Binkley, MD, The Ohio State University, 473 W 12th Ave, Columbus, OH 43210-1252. E-mail [email protected] (Circ Heart Fail. 2010;3:715-725.) © 2010 American Heart Association, Inc. Circ Heart Fail is available at http://circheartfailure.ahajournals.org 715 DOI: 10.1161/CIRCHEARTFAILURE.110.951509 716 Circ Heart Fail November 2010 Downloaded from http://circheartfailure.ahajournals.org/ by guest on June 15, 2017 dramatic example of this connection is in the so-called “broken heart syndrome” or Takotsubo cardiomyopathy.3,5,12 This syndrome of acute and generally reversible heart failure with a characteristic pattern of ventricular contraction abnormalities appears due in part to increased sympathetic activity producing either direct myocardial damage or contractile dysfunction resulting from diffuse coronary vasospasm. A variety of other stress and distress related conditions have been similarly shown to be characterized by significant abnormalities of the autonomic nervous system. Prominent among these is depression, which has been shown to be associated with sympathetic and parasympathetic imbalance and accordingly an environment that can promote coronary artery disease, congestive heart failure, and sudden death.10,13–22 Although sustained increases in sympathetic activity are known to adversely affect cardiovascular function, inappropriately enhanced activity of the parasympathetic nervous system may be similarly damaging. ECG recordings obtained in some rat models of stress show that sudden death is mediated by profound bradycardia progressing to asystole.5,6,8 This suggests that extreme stress may produce an “autonomic storm” characterized by excessive activation of both the sympathetic and parasympathetic nervous systems. Such malignant parasympathetic activity has been shown to play a role in human disease. In a study by Luu et al,23 62% of deaths in patients with advanced heart failure awaiting cardiac transplantation were due to profound bradycardia, suggesting malignant vagotonia as a cause of death. The autonomic control of mind-body interactions has special relevance to patients with heart failure who characteristically have marked parasympathetic/sympathetic imbalance.24,25 Can stress produce autonomic imbalance that in fact leads to the occurrence or progression of ventricular failure? In turn, can the autonomic imbalance in heart failure that parallels that found in stress states in fact promote distress? The significant coincidence of congestive heart failure and depression13,26 and data indicating that depression may precede the appearance of congestive heart failure27,28 suggest that this may be the case. Mind-body interactions that interrupt this reciprocal autonomic dysfunction may therefore benefit both conditions. How Are Emotions and Stress Connected to the Heart? The autonomic nervous system is classically regarded as an “involuntary” system regulated by hypothalamic centers and thus beyond direct conscious control.5,29,30 Nevertheless, it appears that conscious effort can alter cardiovascular function acting through the so-called involuntary autonomic nervous system.5,30,31 However, the question remains how an involuntary nervous system may mediate the cardiovascular responses that characterize conscious mind-heart interactions and the physiological response to various mental states. Increasing understanding of the relationship of cortical function to autonomic control centers provides insight into possible mechanisms for volitional control of cardiovascular function.5,29,32–39 Recognition of the role of cortical control of autonomic function dates to at least 1869 when John Hughlings Jackson40,41 observed significant cardiovascular changes during major motor seizure activity. He reasoned that cortical centers governed not only voluntary motor movements but vasomotion and visceral motor activity. Over the years, a variety of stimulation, ablation, and neuroanatomic studies have defined cortical regions that have projections to centers having direct control over sympathetic and parasympathetic activity.40 These cortical regions include the insular cortex, the somatic and motor sensory cortex, the medial prefrontal cortex, and the anterior cingulate cortex. As an example, the insular cortex has been shown to have a “representation of the autonomic nervous system5” as well as “viscerotopic sensory inputs,”29 including those from the cardiovascular system. Studies in animal models using both insular cortex stimulation and localized destructive lesions and studies in humans who have had insular strokes suggest that the right posterior insular cortex modulates cardiovascular sympathetic control and the left posterior insular cortex modulates parasympathetic function.29,37–39,42– 47 In these models and in human subjects, stimulation of the left insular cortex produced ST changes, widening of the QRS complex, complete heart block leading to asystolic death, and contraction band necrosis (see below).42– 44 The cardiovascular regulatory capacity of the insular cortex suggests one pathway for volitional cardiovascular control that may be operative in mind-heart interactions. Similarly, the anterior cingulated cortex (ACC) has been shown to serve as an interface between cognitive and emotional inputs with projections to autonomic control centers.40,48 It therefore plays a critical role in adaptive responses to the internal and external environment and has been shown to mediate these responses through autonomic pathways. The ACC is functionally, anatomically, and histologically designed to integrate the emotional and cognitive activity of the mind with the physiological responses of the cardiovascular system as well as other organ systems. Functional imaging studies in humans have demonstrated that cortical centers such as the ACC and prefrontal cortex constitute a network integrating emotional and cognitive components of the mind with autonomic cardiovascular control.49 Integrative body-mind training has been shown to increase parasympathetic activity, increase electroencephalographic theta waves originating from these regions, and increase blood flow to these central nervous system centers. Therefore, changes in cognitive and emotional state produce changes in autonomic cardiovascular control producing what some authors have called “brain-body harmony.”49 These functional changes can be accompanied by structural central nervous system changes as evidenced by destructive lesions in the ACC in patients with depression who have had a myocardial infarction.50 Data for more than a century have confirmed that cortical centers integrating emotional responses and cognitive states, which constitute in part what is regarded as the “mind,” have a direct connection to autonomic function. Autonomic control is not simply based on reflex responses but is tightly linked to cortical function. It would therefore be surprising if positive and negative emotional and cognitive states did not have an impact on cardiovascular function and the evolution of cardiovascular diseases. The cortical influence over auto- Emani and Binkley nomic centers supports the belief that cardiovascular function and disease risk can be altered through conscious efforts. Inflammatory and Neuroimmune Pathways Downloaded from http://circheartfailure.ahajournals.org/ by guest on June 15, 2017 Both cardiovascular disease and mental distress are associated with activation of proinflammatory mechanisms. The commonality of these mechanisms identifies inflammatory pathways as a major mediator of reciprocal mind-heart interactions. In addition, inflammation and autonomic activity are closely tied promoting states of neuroimmune activation that are operative in governing both psychological and cardiovascular function. Although the end-organ effects of proinflammatory cytokines are well recognized, the immune system also serves as a communication network between the central nervous system and other organ systems.51–54 Cytokines produced and released in the periphery can diffuse into the central nervous system, where they in many ways function as neurotransmitters.51,55–59 Importantly, proinflammatory cytokines, either from the periphery or produced within the central nervous system, can stimulate the production of norepinephrine and sympathetic activity.60,61 However, beyond the role of circulating cytokines which must diffuse through the blood-brain barrier to the central nervous system, Tracey and other have shown that proinflammatory cytokines convey signals through the peripheral nervous system constituting a system of rapid communication from the periphery to the central nervous system.54 It is apparent that cytokine signaling via the Vagus nerve can occur with cytokine concentrations that fall well below the circulating levels required to cross the blood-brain barrier.54,62– 64 In response to peripheral signaling by cytokines, the autonomic nervous system can in turn activate both proinflammatory and antiinflammatory mechanisms. Bierhaus et al65 showed that stress-induced increases in catecholamines and cortisol rapidly increase NF- expression in peripheral blood monocytes that subsequently increase cytokine production. Further, NF- production could be inhibited by ␣- and -adrenergic blockade demonstrating the role of sympathetic activation in triggering proinflammatory states. The description of a “cholinergic antiinflammatory reflex” exemplifies the orchestration of the mind-body communication network integrating inflammation and autonomic function.54,66 Studies by Tracey et al54,55,66 have shown that stimulation of the efferent Vagus nerve reduces both cytokine production and release by cells of the reticuloendothelial system. The inflammatory reflex consists of stimulation of vagal afferent fibers by cytokines, as discussed above, resulting in an augmentation of central parasympathetic outflow via the Vagus nerve and consequent reduction of cytokine production and release. This system constitutes a servocontrol mechanism that keeps inflammation in check preventing the deleterious effects of excessive proinflammatory stimulation. Conversely, reduced parasympathetic activity, as occurs in disease states such as congestive heart failure, can result in a failure to inhibit proinflammatory cytokine production enhancing the risk of end-organ inflammatory damage and has been shown to be a possible cause of increased proinflammatory cytokines in human subjects.67 Mind-Body Medicine in CHF 717 The evidence is clear that unrestrained proinflammatory stimulation is associated with cognitive and mood changes. A variety of animal models have shown that acute or chronic stress results in increased proinflammatory cytokine production accompanied by behavioral changes and cognitive impairment.55,68,69 These studies parallel investigations in human subjects that show a significant association between distress and depression and immune activation.70,71 Similar to animal studies, administration of cytokines to human subjects, such as interferon-␣, or stimulation of the immune system through vaccination results in depressed mood and activation of the central nervous system in regions known to affect cognitive function and mood.72–74 Studies by Kiecolt-Glaser and Glaser73,75–77 exemplify the connection between chronic stress conditions in human subjects and increases in proinflammatory cytokines. Aging care givers of patients with dementia were followed over a 6-year period with measurement of circulating concentrations of interleukin-6 (IL-6). Progressive increases in IL-6 concentrations were seen in all patients over time, but the rate of increase was significantly higher in members of the care giver cohort, who were under increased stress.76 Similar increases in IL-6 were seen in other stress states such as marital discord.73,77 These and similar studies demonstrate one pathway by which acute or chronic stress can lead to immune system activation with resultant inflammatory cardiovascular damage. Especially considering the apparent role of inflammation in the pathogenesis of congestive heart failure,78,79 these data suggest an intriguing link between stress and the evolution of ventricular dysfunction. Preliminary data from Ferketich et al80 support this link in a study in which patients with symptomatic reduction in ventricular systolic function were screened for symptoms of depression using the Beck Depression Inventory (BDI). In these patients, there was a significant linear correlation between BDI score and concentration of tumor necrosis factor-␣. It can be safely said that the coincidence of depression and heart failure likely creates a proinflammatory environment that can promote the progression of both disorders. A variety of effectors of both the proinflammatory cascade and autonomic nervous system likely play a role in patients with congestive heart failure. As an example, nitric oxide, which is dysregulated in congestive heart failure, plays a role in modulating autonomic function and in mediating inflammation.81 Reduction in nitric oxide production in congestive heart failure has been associated with abnormalities in autonomic balance.82– 87 Recent studies of a loss of function polymorphism of the promoter for nitric oxide synthase demonstrate that it is indeed tightly linked to autonomic function in patients with congestive heart failure.88 Therefore, nitric oxide exemplifies a family of mediators of both inflammatory and autonomic pathways that regulates mindbody interactions and that is especially relevant in patients with congestive heart failure. Environmental Factors Contributing to Mind-Heart Interactions Although mind-body interactions are often considered a self-contained, closed-loop process, there is evidence that 718 Circ Heart Fail November 2010 Downloaded from http://circheartfailure.ahajournals.org/ by guest on June 15, 2017 Figure. Proposed remodeling of mind-heart interactions leads to progressive increases in neuroimmune activation in response to stress. In a state such as depression, there is increased sympathetic activity, decreased parasympathetic activity, and activation of proinflammatory pathways. In response to stress, there is further activation of the sympathetic nervous system and proinflammatory pathways and further withdrawal of parasympathetic activity. This results in an environment that promotes sudden cardiac death and vascular and myocardial injury. external factors, such as infectious agents, may play a role in governing these interactions. A progression of studies has shown a role for Epstein-Barr virus (EBV) infection in mediating altered mood through cytokine stimulation.75,89 –93 An early viral protein, dUTPase, produced even during incomplete replication of EBV, has been shown to stimulate peripheral blood mononuclear cells to produce IL-6 and other cytokines. A strong association between the titer of dUTPase antibody and concentration of circulating IL-6 was found in the above noted study of caregiver stress. Therefore, reactivation of EBV, which is a common latent infection, appears to result in stimulation of production of IL-6 and other proinflammatory cytokines that can mediate both depression and cardiovascular injury. This provides a model by which an external infectious agent may modulate mind-body interactions through promotion and even initiation of the inflammatory “network of communication.” Neurovisceral Regulation: Anatomic Consequences of Mind-Heart Interactions Anatomic and structural changes in the heart and the brain accompany states of mental stress as well as different states of concentration and meditation. These anatomic changes solidify the physical connection between the mind and body further demonstrating the reality of these interactions. In the myocardium, psychological stress has been demonstrated to produce classic changes of contraction band necrosis. Studies of hypothalamic stimulation in animal models demonstrated ECG changes resembling those seen in humans with central nervous system hemorrhage or infarction followed by arrhythmic death. Examination of the myocardium in these animals demonstrated what may be interpreted as contraction band necrosis resembling the lesions seen in ischemic infarction.5,6,94,95 Similar lesions have been pro- duced without central nervous stimulation but with psychic stress.5,96 Studies in human subjects have reported these myocardial lesions in patients with psychiatric illness or subarachnoid hemorrhage.97,98 The finding of increased troponin levels in patients with intracerebral hemorrhage and the demonstration of wall motion abnormalities in patients without coronary artery disease who have had an insular stroke further speak to the structural myocardial damage that can be mediated by the central nervous system.38,39 Conversely, structural changes in the central nervous system have been shown to accompany differing psychological states. Chronic depression has been associated with decreased hippocampal volume, which is related to the duration of depression.99,100 In contrast to the damage and volume loss that may accompany stress, practitioners of various forms of meditation have increased cortical thickening, especially in centers involved with attention and sensory processing including the prefrontal cortex and the right insular cortex.101,102 Corresponding to these observations, functional magnetic resonance studies have shown increased activity in specific regions of the brain in subjects who have practiced mediation for differing periods of time as compared with control subjects.102 Associated with these anatomic changes is evidence for a remodeling of mind-body interactions, which evolves with repeated or sustained stress. This remodeling may “prime” the systems governing mind-body interactions to produce an exaggerated responses to stressful stimuli (Figure). The existence of this remodeling process is supported by studies showing that subjects with early life trauma have significant increases in baseline and stress-induced neuroimmune activation.71 A variety of investigations have shown that episodes of depression are not isolated but demonstrate a pattern of repetition suggesting evolution of pathways that progres- Emani and Binkley sively facilitate depressed mood.10 Indeed, many of the same mediators of mind-heart and mind-body interactions are operative in central nervous system structural remodeling. Chief among them are cytokines that are known to act as neural trophic factors but which can over time mediate apoptosis and reduction of tissue volume.55 It may be speculated that remodeling of mind-heart interactions results in an increasing magnitude of stress responses that lead to permanent detrimental end organ damage. As an example, if repeated stress produces even small areas of contraction band necrosis over time, could this ultimately result in ventricular systolic dysfunction and dilation? Further, would such remodeling of mind-heart interactions make patients less susceptible to the potential beneficial effects of interventions such as biofeedback, meditation, or other mindbody therapies? Downloaded from http://circheartfailure.ahajournals.org/ by guest on June 15, 2017 Interventions Targeting Mind-Heart Interactions A rich mechanistic foundation for mind-body and mind-heart interactions has now been established. This then raises the question as to whether there are volitional modifications of these interactions that can prevent and treat disease states. There is now a wealth of clinical, mechanistic and outcome trials that attempt to address this issue although the quality of these investigations is highly variable.103 Relatively few of these specifically address prevention or treatment of congestive heart failure, although many have addressed risk factors for cardiovascular diseases in general, and may lead to further observations in the setting of ventricular failure. The mind-body interventions that have been explored include biofeedback methods, meditation techniques, and relaxation therapies. Biofeedback Biofeedback interventions can be broadly defined as those in which the subject learns to consciously regulate a given physiological “target” variable.104 Often, the ability to regulate this specific variable is accompanied by modification of other elements of the mind-heart interaction. One of the most detailed studies of biofeedback is an investigation by Moser et al105 performed in patients with advanced congestive heart failure. Participants were randomized to either biofeedback intervention or to control conditions. The biofeedback cohort successfully increased skin temperature, and compared with control subjects, significantly increased cardiac output, reduced systemic vascular resistance, and decreased respiratory frequency. The mechanism by which the biofeedback intervention produced these changes in hemodynamic variables is not certain but may have resulted from biofeedback associated alterations in autonomic vascular control. Similarly, short-term studies of slow breathing in patients with congestive heart failure have shown immediate changes in baroreflex sensitivity measured by the interaction of heart rate and blood pressure variability.106 For the congestive heart failure group as a whole, there was a decrease in systolic and diastolic blood pressure during slow breathing. This and other studies suggest that there is the capacity to consciously regulate autonomically governed mind-heart interactions through alteration of baroreflex function.104,107–109 Mind-Body Medicine in CHF 719 Meditation and Relaxation Techniques Meditation and relaxation techniques have been investigated as other methods to beneficially alter mind-body interactions. Meditation techniques may be broadly classified in three categories. First are those techniques that require concentration on a specific external object or internal sensation (such as breathing) in preparation for focused reflection, exclusion of unwanted thoughts, or a quiet state of awareness.103,110,111 Transcendental meditation may be the most commonly recognized form of this category of meditation. Second are those that rely on increased awareness or mindfulness of the external and internal environment and exclusion of conscious interpretations or evaluations of events and sensations in these environments. Third is compassion mediation which incorporates stages of the above practices with the ultimate goal of eliminating negative evaluations and fostering positive attitudes toward the self and progressively to others in one’s surroundings.110 All of these require self-monitoring and progressive practice to achieve a desired state of awareness. Other techniques rely on eliciting the relaxation response, which shares many features of the above mediation techniques. In essence, relaxation techniques consist of focused attention, a passive nonevaluative approach to thoughts, relaxation of muscle tone, and a nondistracting environment.112–114 The hallmark of the relaxation response is a reduction in sympathetic nervous system activity. Only a relatively small number of outcome studies have examined the above or related mind-body interventions in patients with congestive heart failure. However, a number of studies have investigated both cardiovascular and clinical outcomes following programs of meditation or relaxation techniques. For example, it is estimated that there have been more than 600 studies published examining the impact of transcendental meditation on cardiovascular disease.115 A review of selected studies of these techniques in patients without heart failure provides proof of concept that they may be effective in altering mind-heart interactions in patients with ventricular failure. Barnes et al116 examined blood pressure and noninvasively measured cardiac output in adults without known cardiovascular disease who practiced transcendental meditation. Compared with a control group using relaxation methods, those practicing transcendental meditation had decreases in systolic and diastolic blood pressures, increases in cardiac output, and decreases in systemic vascular resistance during meditation. Similar results have been reported in adolescents with blood pressures in the upper percentiles of normal.117,118 The capacity to alter vascular tone and blood pressure may extend to perhaps all forms of meditation. A 6-week trial of yoga and meditation demonstrated significant reductions in heart rate and blood pressure and evidence for endothelium-dependent vasodilation in the intervention group.119 It is probable that mediation exerts its effect on vascular control through autonomic mechanisms. This has been specifically examined by measurement of heart rate variability and noninvasive measures of the preejection period (a surrogate for sympathetic activity) in a study of mindfulness meditation.119 In subjects practicing this form of meditation, there was coactivation of the sympathetic and parasympa- 720 Circ Heart Fail November 2010 Downloaded from http://circheartfailure.ahajournals.org/ by guest on June 15, 2017 thetic nervous systems, a relative unusual event. This demonstrates the profound effect of this form of meditation on autonomic function which has been suggested in other studies and for other forms of meditation.49,120,121 In addition to their influence on autonomic function, meditation and related techniques appear to influence the immune component of mind-body interactions. In a recent study, investigators measured markers of immune function in healthy women stratified by their expertise in the practice of hatha yoga122 and found that experienced practitioners had lower levels of IL-6 and that novices had a greater odds of having detectable C-reactive protein. Similar results have been reported in a study of compassion mediation, in which expert practitioners were found to have lower social stressinduced levels of IL-6.110 These representative studies demonstrate that the various elements governing mind-body and mind-heart interactions can be consciously influenced by practices such as meditation. Even the immune system, which may appear to be far beyond the influence of conscious thought, can be regulated through conscious effort and meditative practices. The studies that have targeted patients with congestive heart failure suggest that this may be the case in at least selected patients with ventricular dysfunction. Can Mind-Body Interventions Alter the Course of Congestive Heart Failure? Does the fact that meditation and relaxation techniques modify mind-body interactions in non– heart failure populations imply that these techniques can serve as effective complementary therapies in patients with ventricular dysfunction? As the severity of ventricular dysfunction progresses, is the remodeling of mind-body interactions advanced to the degree that they are irreversible? In severely ill patients, including those with heart failure, heart rate and blood pressure do not correlate with the severity of anxiety.123 This implies that the underlying disease process of congestive heart failure may have already established a fixed autonomic set point which is not readily altered by meditation or relaxation therapies. Among the relatively small studies that have specifically addressed patients with heart failure, Jayadevappa et al111 examined 23 African American subjects hospitalized for heart failure who were randomly assigned to a program of transcendental meditation or health education. After 6 months, the transcendental mediation group had a significant increase in the 6-minute walk distance as well as improvement in depression scores and measures of quality of life. In addition, the meditation group was found to have a reduction in hospitalizations over the 6-month study period. Yeh et al124,125 used Tai Chi as a specific meditative style in heart failure patients in 2 different studies and found significant improvement in 6-minute walk distances, improved quality of life, and reduction of brain natriuretic peptide. A prospective study of body scan mediation in patients with heart failure demonstrated improved quality-of-life scores, improved measures of exercise performance, and reduction in plasma norepinephrine.126 Related to meditation techniques are stress management therapies designed to provoke the relaxation response. In a study of patients with New York Heart Association class II and III symptoms, cognitive therapy and stress management improved exercise stress duration as well depression scores and were associated with significant weight loss.127 Guided imagery offers another approach to elicit the relaxation response and has been examined in a small uncontrolled pilot study of patients with heart failure but only demonstrated trends to improved quality-of-life measures and no change in exercise capacity.128 Other relatively small studies ranging from 14 to 83 participants have examined a variety of relaxation therapies in patients with congestive heart failure and have found only changes in subjective measures of perceived wellness but not more objective physiological measures.129 –132 The recently published SEARCH trial enrolled a comparatively large number of patients with relatively severe left ventricular dysfunction.133 Participants in the treatment arm were enrolled in a program of instruction in mindfulnessbased stress reduction, coping skills, and participation in expressive support group discussions. At 12 months, the participants in the intervention program reported a perception of symptomatic improvement and had improved scores on anxiety, depression, and quality-of-life scales. This study represents one of the strongest demonstrations that mindbody interventions can produce a positive impact in at least a subset of patients with congestive heart failure and provides a foundation for future investigations (Table). Summary and Conclusions Evidence shows that there is a genuine physical and reciprocal connection between the mind and the body defined by physiological pathways and organic structural remodeling of the elements of these interactions. Further, interventions and practices such as biofeedback, relaxation therapies, and meditation clearly alter at least acutely if not chronically the effector systems governing mind-body and mind-heart interactions. Less clear is the role these interventions may play in the immediate or future management of patients with ventricular failure. There is at this time a paucity of studies that directly address these questions in patients with congestive heart failure. Is it possible that mind-heart intervention techniques can reverse the remodeling of many of these pathways, including the known aberrations of autonomic balance that evolve early in the course of ventricular failure and that may contribute to the progression of the disease process?25 Can mind-body and mind-heart interactions address the significant depression and anxiety that are prevalent in patients with congestive heart failure and reverse the neuroimmune activation operative in both conditions?9,13,27,28,55,69,80 The evidence-based medicine to address these questions is lacking. As can be seen from the literature discussed in this review, the clinical studies of mind-heart interventions are often uncontrolled and underpowered owing to small sample sizes. This has been recognized as a major limitation faced by a large number of studies investigating mind-body interventions.103,134 In an era of translational investigation, this appears to be a field ideally suited to the evolving scientific Emani and Binkley Table. Mind-Body Medicine in CHF 721 Representative Studies Examining Mind-Body Interventions in Congestive Heart Failure Intervention Author and Reference No. Downloaded from http://circheartfailure.ahajournals.org/ by guest on June 15, 2017 n (Treatment Arm) Biofeedback Moser et al105 Follow-Up Outcomes With Intervention Prospective Randomized controlled 40 (20) Immediate Increased cardiac output and decreased systemic vascular resistance No changes in catecholamine levels or O2 consumption Biofeedback Swanson et al109 Prospective Randomized controlled 29 (15) 6 weeks Improved 6MWD for subgroup with ejection fraction ⬎30% (n⫽9 vs 8) No significant change in HRV or QoL Slow breathing Bernardi et al106 Prospective NR Self-matched and controlled 102 (81) Immediate Increased baroreflex sensitivity and BP decrease in heart failure patients pre intervention vs postintervention (self-matched) No significant difference between heart failure and control populations Transcendental Meditation Jayadevappa et al111 Prospective Randomized controlled 23 (13) 6 mo Improved 6MWD, depression scores, and QoL Meditation Curiati et al126 Prospective Randomized controlled 19 (10) 14 wk Reduced NE levels and improved QoL Left ventricular ejection fraction not significantly changed Tai Chi Yeh et al124,125 Prospective Randomized controlled 30 (15) 12 wk Improved QoL, 6MWD, decreased brain natriuretic peptide Stress management Kostis et al127 Prospective Randomized controlled 19 (7) 12 wk Improved exercise time, QoL, depression, and weight loss 6MWD not statistically improved Stress management Luskin et al132 Prospective Incomplete Randomization controlled 33 (14) 10 wk Improved 6MWD, depression, perceived stress, and emotional distress HRV not statistically improved Mindfulness-based stress reduction Sullivan et al (SEARCH Trial)133 Prospective NR 217 (117) 12 mo Improved symptoms, anxiety, depression, and QoL No differences in death and rehospitalization Klaus et al128 Prospective NR Self-matched 8 6 wk No statistically significant improvements in exercise or dyspnea measures QoL measures trended towards but not significant for improvement Progressive muscle relaxation training Yu et al129 Prospective Randomized controlled 121 (59) 14 wk Trend toward symptom improvement Relaxation response Chang et al130 Prospective Randomized controlled 83 (33) Approx 4 mo Improved spiritual QoL Trend toward improved emotional QoL Physical QoL and exercise capacity not improved by relaxation response Guided imagery Type NR indicates nonrandomized; 6MWD, 6-minute walk distance; QoL, quality of life; HRV, heart rate variability; and NE, norepinephrine. methods that connect fundamental scientific discovery to clinical practice. It is possible that these interventions will constitute important therapies complementary to current standard care. As an example, a population-based study examining the impact of spirituality on autonomic function and cardiovascular disease found that an increase in the aggregate score of spirituality measures highly correlated with autonomic control.3 This is relevant to patients with congestive heart failure, who, with progressive severity of disease, lose diurnal variation of parasympathetic/sympathetic balance, which in effect represents a lack of what has been defined as autonomic control.135–138 Therefore, is it possible that mind-body interventions can restore normal autonomic control in patients with congestive heart failure? Could these interventions increase responsiveness to pharmacological treatment? The role that mind-heart interventions will play in the future treatment of patients with congestive heart failure is yet to be defined. Although there is the clear indication that the field of behavioral cardiology is one that is likely to continue its evolution and play a significant role in the advancement of patient care, it is also clear that this must be preceded by further studies confirming benefit and defining this field of practice.134 Further, although complementary and alternative therapies are embraced by many patients, they require commitment of time and to lifestyle change.139 Nevertheless, the reality of the mind-heart connection cannot be ignored, and cardiovascular specialists must continue to engage in the understanding, translational research, and application of this field. Translational science must now meet the challenge to build on the intriguing studies that have established the mechanistic 722 Circ Heart Fail November 2010 basis for mind-heart interactions. There are a wide variety of investigations that must follow. The authors suggest a few: ● ● ● ● Downloaded from http://circheartfailure.ahajournals.org/ by guest on June 15, 2017 ● Investigate the capacity of mind-heart interactions to increase susceptibility to pharmacological therapy and to cardiac resynchronization therapy. Test whether the response to drug administration coordinated with mind-heart interventions is augmented compared with standard dosing regimens. Test the capacity of mind-heart interventions to alleviate comorbid conditions such as sleep disorders that commonly accompany ventricular failure are themselves influenced by states of stress and anxiety.140 Evaluate the capacity of mind-heart interventions to improve ventricular function through interruption of the cascade of autonomic and proinflammatory pathways activated by depression and stress.141,142 Investigate the response to mind-body interventions in the context of different genetic backgrounds similar to the pharmacogenetic impact on drug response. Conversely, evaluate the impact of mind-heart interventions on gene function based on preliminary studies showing the plausibility of “mind/gene” interactions.143,144 These constitute just a few of the exciting possibilities for translational research in mind-heart medicine and adapting this field to the overall clinical and investigative approach to patients with congestive heart failure. It is hoped that the field of translational cardiovascular medicine will explore research questions such as these and others to allow mind-heart interventions to take a place in the growing armamentarium of heart failure therapies. Sources of Funding Dr Philip F. Binkley is supported by the James H. and Ruth J. Wilson Professorship. Disclosures None. References 1. Chan CL, Ng SM, Ho RT, Chow AY. East meets West: applying eastern spirituality in clinical practice. J Clin Nurs. 2006;15:822– 832. 2. Honderich T, editor. The Oxford Companion to Philosophy. Oxford: Oxford University Press; 1995:1009. 3. Berntson GG, Norman GJ, Hawkley LC, Cacioppo JT. Spirituality and autonomic cardiac control. Ann Behav Med. 2008;35:198 –208. 4. Penn MS, Bakken EE. Heart-brain medicine: where we go from here and why. Cleve Clin J Med. 2007;74(Suppl 1):S4 –S6. 5. Samuels MA. The brain-heart connection. Circulation. 2007;116:77– 84. 6. Samuels MA. ‘Voodoo’ death revisited: the modern lessons of neurocardiology. Cleve Clin J Med. 2007;74(Suppl 1):S8 –S16. 7. Cannon WB. Voodoo death. Am Anthropologist. 1942;44(new series): 169 –181; Am J Public Health. 2002;92:1593–1595. 8. Sgoifo A, De Boer SF, Buwalda B, Korte-Bouws G, Tuma J, Bohus B, Zaagsma J, Koolhaas JM. Vulnerability to arrhythmias during social stress in rats with different sympathovagal balance. Am J Physiol. 1998;275(2 Pt 2):H460 –H466. 9. Grippo AJ, Johnson AK. Stress, depression and cardiovascular dysregulation: a review of neurobiological mechanisms and the integration of research from preclinical disease models. Stress. 2009;12:1–21. 10. Kubzansky LD. Sick at heart: the pathophysiology of negative emotions. Cleve Clin J Med. 2007;74(Suppl 1):S67–S72. 11. Skinner JE. Role of the brain in ventricular fibrillation and hypertension: from animal models to early human studies. Cleve Clin J Med. 2007; 74(Suppl 1):S73–S78. 12. Wittstein IS. The broken heart syndrome. Cleve Clin J Med. 2007; 74(Suppl 1):S17–S22. 13. Joynt KE, Whellan DJ, O’Connor CM. Why is depression bad for the failing heart? A review of the mechanistic relationship between depression and heart failure. J Card Fail. 2004;10:258 –271. 14. Esler M, Kaye D. Sympathetic nervous system activation in essential hypertension, cardiac failure and psychosomatic heart disease. J Cardiovasc Pharmacol. 2000;35(7 Suppl 4):S1–S7. 15. Esler M, Turbott J, Schwarz R, Leonard P, Bobik A, Skews H, Jackman G. The peripheral kinetics of norepinephrine in depressive illness. Arch Gen Psychiatry. 1982;39:295–300. 16. Rechlin T, Weis M, Spitzer A, Kaschka WP. Are affective disorders associated with alterations of heart rate variability? J Affect Disord. 1994;32:271–275. 17. Carney RM, Saunders RD, Freedland KE, Stein P, Rich MW, Jaffe AS. Association of depression with reduced heart rate variability in coronary artery disease. Am J Cardiol. 1995;76:562–564. 18. Krittayaphong R, Cascio WE, Light KC, Sheffield D, Golden RN, Finkel JB, Glekas G, Koch GG, Sheps DS. Heart rate variability in patients with coronary artery disease: differences in patients with higher and lower depression scores. Psychosom Med. 1997;59:231–235. 19. Watkins LL, Grossman P. Association of depressive symptoms with reduced baroreflex cardiac control in coronary artery disease. Am Heart J. 1999;137:453– 457. 20. Barton DA, Dawood T, Lambert EA, Esler MD, Haikerwal D, Brenchley C, Socratous F, Kaye DM, Schlaich MP, Hickie I, Lambert GW. Sympathetic activity in major depressive disorder: identifying those at increased cardiac risk? J Hypertens. 2007;25:2117–2124. 21. Brown AD, Barton DA, Lambert GW. Cardiovascular abnormalities in patients with major depressive disorder: autonomic mechanisms and implications for treatment. CNS Drugs. 2009;23:583– 602. 22. Hausberg M, Hillebrand U, Kisters K. Addressing sympathetic overactivity in major depressive disorder. J Hypertens. 2007;25:2004 –2005. 23. Luu M, Stevenson WG, Stevenson LW, Baron K, Walden J. Diverse mechanisms of unexpected cardiac arrest in advanced heart failure. Circulation. 1989;80:1675–1680. 24. Binkley PF, Nunziata E, Haas GJ, Nelson SD, Cody RJ. Parasympathetic withdrawal is an integral component of autonomic imbalance in congestive heart failure: demonstration in human subjects and verification in a paced canine model of ventricular failure. J Am Coll Cardiol. 1991;18:464 – 472. 25. Eaton GM, Cody RJ, Nunziata E, Binkley PF. Early left ventricular dysfunction elicits activation of sympathetic drive and attenuation of parasympathetic tone in the paced canine model of congestive heart failure. Circulation. 1995;92:555–561. 26. Ferketich AK, Binkley PF. Psychological distress and cardiovascular disease: results from the 2002 national health interview survey. Eur Heart J. 2005;26:1923–1929. 27. Abramson J, Berger A, Krumholz HM, Vaccarino V. Depression and risk of heart failure among older persons with isolated systolic hypertension. Arch Intern Med. 2001;161:1725–1730. 28. Williams SA, Kasl SV, Heiat A, Abramson JL, Krumholz HM, Vaccarino V. Depression and risk of heart failure among the elderly: a prospective community-based study. Psychosom Med. 2002;64:6 –12. 29. Cheung RT, Hachinski V. The insula and cerebrogenic sudden death. Arch Neurol. 2000;57:1685–1688. 30. Dikshit BB. The production of cardiac irregularities by excitation of the hypothalmic centres. J Physiol. 1934;81:382–394. 31. Armour JA. The little brain on the heart. Cleve Clin J Med. 2007; 74(Suppl 1):S48 –S51. 32. Bennett MR, Hacker PM. Emotion and cortical-subcortical function: conceptual developments. Prog Neurobiol. 2005;75:29 –52. 33. Buijs RM, Van Eden CG. The integration of stress by the hypothalamus, amygdala and prefrontal cortex: balance between the autonomic nervous system and the neuroendocrine system. Prog Brain Res. 2000;126: 117–132. 34. Furness JB. The organisation of the autonomic nervous system: Peripheral connections. Auton Neurosci. 2006;130:1–5. 35. Ulrich-Lai YM, Herman JP. Neural regulation of endocrine and autonomic stress responses. Nat Rev Neurosci. 2009;10:397– 409. Emani and Binkley Downloaded from http://circheartfailure.ahajournals.org/ by guest on June 15, 2017 36. Groenewegen HJ, Uylings HB. The prefrontal cortex and the integration of sensory, limbic and autonomic information. Prog Brain Res. 2000; 126:3–28. 37. Cheshire WP Jr, Saper CB. The insular cortex and cardiac response to stroke. Neurology. 2006;66:1296 –1297. 38. Hays A, Diringer MN. Elevated troponin levels are associated with higher mortality following intracerebral hemorrhage. Neurology. 2006; 66:1330 –1334. 39. Laowattana S, Zeger SL, Lima JA, Goodman SN, Wittstein IS, Oppenheimer SM. Left insular stroke is associated with adverse cardiac outcome. Neurology. 2006;66:477– 483. 40. Cechetto DF, Saper CB. Role of the cerebral cortex in autonomic function. In: Loewy AD, Spyer KM, editors. Central Regulation of Autonomic Function. New York, New York: Oxford University Press; 1990:208. 41. Hoff EC, Kell JF Jr, Carroll MN Jr. Effects of cortical stimulation and lesions on cardiovascular function. Physiol Rev. 1963;43:68 –114. 42. Oppenheimer S. Cortical control of the heart. Cleve Clin J Med. 2007; 74(Suppl 1):S27–S29. 43. Oppenheimer S. Cerebrogenic cardiac arrhythmias: cortical lateralization and clinical significance. Clin Auton Res. 2006;16:6 –11. 44. Oppenheimer S. The anatomy and physiology of cortical mechanisms of cardiac control. Stroke. 1993;24(12 Suppl):I3–I5. 45. Oppenheimer SM, Gelb A, Girvin JP, Hachinski VC. Cardiovascular effects of human insular cortex stimulation. Neurology. 1992;42: 1727–1732. 46. Oppenheimer SM, Kedem G, Martin WM. Left-insular cortex lesions perturb cardiac autonomic tone in humans. Clin Auton Res. 1996;6: 131–140. 47. Ay H, Koroshetz WJ, Benner T, Vangel MG, Melinosky C, Arsava EM, Ayata C, Zhu M, Schwamm LH, Sorensen AG. Neuroanatomic correlates of stroke-related myocardial injury. Neurology. 2006;66: 1325–1329. 48. Allman JM, Hakeem A, Erwin JM, Nimchinsky E, Hof P. The anterior cingulate cortex. the evolution of an interface between emotion and cognition. Ann N Y Acad Sci. 2001;935:107–117. 49. Tang YY, Ma Y, Fan Y, Feng H, Wang J, Feng S, Lu Q, Hu B, Lin Y, Li J, Zhang Y, Wang Y, Zhou L, Fan M. Central and autonomic nervous system interaction is altered by short-term meditation. Proc Natl Acad Sci U S A. 2009;106:8865– 8870. 50. Rapp MA, Rieckmann N, Lessman DA, Tang CY, Paulino R, Burg MM, Davidson KW. Persistent depressive symptoms after acute coronary syndrome are associated with compromised white matter integrity in the anterior cingulate: a pilot study. Psychother Psychosom. 2010;79: 149 –155. 51. Besedovsky H, del Rey A, Sorkin E, Dinarello CA. Immunoregulatory feedback between interleukin-1 and glucocorticoid hormones. Science. 1986;233:652– 6524. 52. Blalock JE. Shared ligands and receptors as a molecular mechanism for communication between the immune and neuroendocrine systems. Ann N Y Acad Sci. 1994;741:292–298. 53. Blalock JE. The immune system as a sensory organ. J Immunol. 1984; 132:1067–1070. 54. Tracey KJ. The inflammatory reflex. Nature. 2002;420:853– 859. 55. Miller AH, Maletic V, Raison CL. Inflammation and its discontents: the role of cytokines in the pathophysiology of major depression. Biol Psychiatry. 2009;65:732–741. 56. Besedovsky HO, del Rey A. Immune-neuro-endocrine interactions: facts and hypotheses. Endocr Rev. 1996;17:64 –102. 57. Raison CL, Borisov AS, Majer M, Drake DF, Pagnoni G, Woolwine BJ, Vogt GJ, Massung B, Miller AH. Activation of central nervous system inflammatory pathways by interferon-alpha: relationship to monoamines and depression. Biol Psychiatry. 2009;65:296 –303. 58. Raison CL, Miller AH. The neuroimmunology of stress and depression. Semin Clin Neuropsychiatry. 2001;6:277–294. 59. Rankine EL, Hughes PM, Botham MS, Perry VH, Felton LM. Brain cytokine synthesis induced by an intraparenchymal injection of LPS is reduced in MCP-1-deficient mice prior to leucocyte recruitment. Eur J Neurosci. 2006;24:77– 86. 60. Anisman H, Merali Z, Hayley S. Neurotransmitter, peptide and cytokine processes in relation to depressive disorder: comorbidity between depression and neurodegenerative disorders. Prog Neurobiol. 2008; 85:1–74. 61. Felger JC, Alagbe O, Hu F, Mook D, Freeman AA, Sanchez MM, Kalin NH, Ratti E, Nemeroff CB, Miller AH. Effects of interferon-alpha on 62. 63. 64. 65. 66. 67. 68. 69. 70. 71. 72. 73. 74. 75. 76. 77. 78. 79. 80. 81. Mind-Body Medicine in CHF 723 rhesus monkeys: a nonhuman primate model of cytokine-induced depression. Biol Psychiatry. 2007;62:1324 –1333. Goehler LE, Gaykema RP, Hansen MK, Anderson K, Maier SF, Watkins LR. Vagal immune-to-brain communication: a visceral chemosensory pathway. Auton Neurosci. 2000;85:49 –59. Goehler LE, Relton JK, Dripps D, Kiechle R, Tartaglia N, Maier SF, Watkins LR. Vagal paraganglia bind biotinylated interleukin-1 receptor antagonist: a possible mechanism for immune-to-brain communication. Brain Res Bull. 1997;43:357–364. Hansen MK, Nguyen KT, Goehler LE, Gaykema RP, Fleshner M, Maier SF, Watkins LR. Effects of vagotomy on lipopolysaccharide-induced brain interleukin-1beta protein in rats. Auton Neurosci. 2000;85: 119 –126. Bierhaus A, Wolf J, Andrassy M, Rohleder N, Humpert PM, Petrov D, Ferstl R, von Eynatten M, Wendt T, Rudofsky G, Joswig M, Morcos M, Schwaninger M, McEwen B, Kirschbaum C, Nawroth PP. A mechanism converting psychosocial stress into mononuclear cell activation. Proc Natl Acad Sci U S A. 2003;100:1920 –1925. Pavlov VA, Tracey KJ. The cholinergic anti-inflammatory pathway. Brain Behav Immunol. 2005;19:493– 499. Sloan RP, McCreath H, Tracey KJ, Sidney S, Liu K, Seeman T. RR interval variability is inversely related to inflammatory markers: the CARDIA study. Mol Med. 2007;13:178 –184. Godbout JP, Moreau M, Lestage J, Chen J, Sparkman NL, O’Connor J, Castanon N, Kelley KW, Dantzer R, Johnson RW. Aging exacerbates depressive-like behavior in mice in response to activation of the peripheral innate immune system. Neuropsychopharmacology. 2008;33: 2341–2351. Dantzer R, O’Connor JC, Freund GG, Johnson RW, Kelley KW. From inflammation to sickness and depression: when the immune system subjugates the brain. Nat Rev Neurosci. 2008;9:46 –56. Steptoe A, Hamer M, Chida Y. The effects of acute psychological stress on circulating inflammatory factors in humans: a review and meta-analysis. Brain Behav Immun. 2007;21:901–912. Pace TW, Mletzko TC, Alagbe O, Musselman DL, Nemeroff CB, Miller AH, Heim CM. Increased stress-induced inflammatory responses in male patients with major depression and increased early life stress. Am J Psychiatry. 2006;163:1630 –1633. Capuron L, Pagnoni G, Demetrashvili M, Woolwine BJ, Nemeroff CB, Berns GS, Miller AH. Anterior cingulate activation and error processing during interferon-alpha treatment. Biol Psychiatry. 2005;58:190 –196. Kiecolt-Glaser JK, Loving TJ, Stowell JR, Malarkey WB, Lemeshow S, Dickinson SL, Glaser R. Hostile marital interactions, proinflammatory cytokine production, and wound healing. Arch Gen Psychiatry. 2005; 62:1377–1384. Benedetti F, Lucca A, Brambilla F, Colombo C, Smeraldi E. Interleukine-6 serum levels correlate with response to antidepressant sleep deprivation and sleep phase advance. Prog Neuropsychopharmacol Biol Psychiatry. 2002; 26:1167–1170. Glaser R, Robles TF, Sheridan J, Malarkey WB, Kiecolt-Glaser JK. Mild depressive symptoms are associated with amplified and prolonged inflammatory responses after influenza virus vaccination in older adults. Arch Gen Psychiatry. 2003;60:1009 –1014. Kiecolt-Glaser JK, Preacher KJ, MacCallum RC, Atkinson C, Malarkey WB, Glaser R. Chronic stress and age-related increases in the proinflammatory cytokine IL-6. Proc Natl Acad Sci U S A. 2003;100: 9090 –9095. Kiecolt-Glaser JK, Glaser R, Cacioppo JT, Malarkey WB. Marital stress: immunologic, neuroendocrine, and autonomic correlates. Ann N Y Acad Sci. 1998;840:656 – 663. Gullestad L, Aass H, Fjeld JG, Wikeby L, Andreassen AK, Ihlen H, Simonsen S, Kjekshus J, Nitter-Hauge S, Ueland T, Lien E, Froland SS, Aukrust P. Immunomodulating therapy with intravenous immunoglobulin in patients with chronic heart failure. Circulation. 2001;103: 220 –225. Aukrust P, Yndestad A, Damas JK, Gullestad L. Inflammation and chronic heart failure-potential therapeutic role of intravenous immunoglobulin. Autoimmun Rev. 2004;3:221–227. Ferketich AK, Ferguson JP, Binkley PF. Depressive symptoms and inflammation among heart failure patients. Am Heart J. 2005;150: 132–136. Cooke GE, Doshi A, Binkley PF. Endothelial nitric oxide synthase gene: prospects for treatment of heart disease. Pharmacogenomics. 2007;8: 1723–1734. 724 Circ Heart Fail November 2010 Downloaded from http://circheartfailure.ahajournals.org/ by guest on June 15, 2017 82. Schultz HD. Nitric oxide regulation of autonomic function in heart failure. Curr Heart Fail Rep. 2009;6:71– 80. 83. Hirooka Y, Shigematsu H, Kishi T, Kimura Y, Ueta Y, Takeshita A. Reduced nitric oxide synthase in the brainstem contributes to enhanced sympathetic drive in rats with heart failure. J Cardiovasc Pharmacol. 2003;42(Suppl 1):S111–S115. 84. Wang Y, Patel KP, Cornish KG, Channon KM, Zucker IH. nNOS gene transfer to RVLM improves baroreflex function in rats with chronic heart failure. Am J Physiol Heart Circ Physiol. 2003;285:H1660–H1667. 85. Chowdhary S, Ng GA, Nuttall SL, Coote JH, Ross HF, Townend JN. Nitric oxide and cardiac parasympathetic control in human heart failure. Clin Sci (Lond). 2002;102:397– 402. 86. Li YF, Roy SK, Channon KM, Zucker IH, Patel KP. Effect of in vivo gene transfer of nNOS in the PVN on renal nerve discharge in rats. Am J Physiol Heart Circ Physiol. 2002;282:H594 –H601. 87. Zucker IH, Pliquett RU. Novel mechanisms of sympatho-excitation in chronic heart failure. Heart Fail Monit. 2002;3:2–7. 88. Binkley PF, Nunziatta E, Liu-Stratton Y, Cooke G. A polymorphism of the endothelial nitric oxide synthase promoter is associated with an increase in autonomic imbalance in patients with congestive heart failure. Am Heart J. 2005;149:342–348. 89. Ariza ME, Glaser R, Kaumaya PT, Jones C, Williams MV. The EBVencoded dUTPase activates NF-kappa B through the TLR2 and MyD88dependent signaling pathway. J Immunol. 2009;182:851– 859. 90. Waldman WJ, Williams MV Jr, Lemeshow S, Binkley P, Guttridge D, Kiecolt-Glaser JK, Knight DA, Ladner KJ, Glaser R. Epstein-Barr virus-encoded dUTPase enhances proinflammatory cytokine production by macrophages in contact with endothelial cells: evidence for depression-induced atherosclerotic risk. Brain Behav Immun. 2008;22: 215–223. 91. Glaser R, Litsky ML, Padgett DA, Baiocchi RA, Yang EV, Chen M, Yeh PE, Green-Church KB, Caligiuri MA, Williams MV. EBV-encoded dUTPase induces immune dysregulation: Implications for the pathophysiology of EBV-associated disease. Virology. 2006;346:205–218. 92. Padgett DA, Hotchkiss AK, Pyter LM, Nelson RJ, Yang E, Yeh PE, Litsky M, Williams M, Glaser R. Epstein-Barr virus-encoded dUTPase modulates immune function and induces sickness behavior in mice. J Med Virol. 2004;74:442– 448. 93. Williams MV, Holliday J, Glaser R. Induction of a deoxyuridine triphosphate nucleotidohydrolase activity in Epstein-Barr virus-infected cells. Virology. 1985;142:326 –333. 94. Melville KI, Blum B, Shister HE, Silver MD. Cardiac ischemic changes and arrhythmias induced by hypothalamic stimulation. Am J Cardiol. 1963;12:781–791. 95. Melville KI, Garvey HL, Shister HE, Knaack J. Central nervous system stimulation and cardiac ischemic changes in monkeys. Ann N Y Acad Sci. 1969;156:241–260. 96. Selye H. The chemical prevention of cardiac necrosis. New York, New York: Ronald Press; 1958. 97. Cebelin MS, Hirsch CS. Human stress cardiomyopathy. myocardial lesions in victims of homicidal assaults without internal injuries. Hum Pathol. 1980;11:123–132. 98. Koskelo P, Punsar S, Sipilae W. Subendocardial haemorrhage and ECG changes in intracranial bleeding. BMJ. 1964;1:1479 –1480. 99. Nair A, Vadodaria KC, Banerjee SB, Benekareddy M, Dias BG, Duman RS, Vaidya VA. Stressor-specific regulation of distinct brain-derived neurotrophic factor transcripts and cyclic AMP response elementbinding protein expression in the postnatal and adult rat hippocampus. Neuropsychopharmacology. 2007;32:1504 –1519. 100. Vaidya VA. Stress, depression and hippocampal damage. J Biosci. 2000;25:123–124. 101. Lazar SW, Kerr CE, Wasserman RH, Gray JR, Greve DN, Treadway MT, McGarvey M, Quinn BT, Dusek JA, Benson H, Rauch SL, Moore CI, Fischl B. Meditation experience is associated with increased cortical thickness. Neuroreport. 2005;16:1893–1897. 102. Brefczynski-Lewis JA, Lutz A, Schaefer HS, Levinson DB, Davidson RJ. Neural correlates of attentional expertise in long-term meditation practitioners. Proc Natl Acad Sci U S A. 2007;104:11483–11488. 103. Barrows KA, Jacobs BP. Mind-body medicine. an introduction and review of the literature. Med Clin North Am. 2002;86:11–31. 104. Moravec CS. Biofeedback therapy in cardiovascular disease: rationale and research overview. Cleve Clin J Med. 2008;75(Suppl 2):S35–S38. 105. Moser DK, Dracup K, Woo MA, Stevenson LW. Voluntary control of vascular tone by using skin-temperature biofeedback-relaxation in 106. 107. 108. 109. 110. 111. 112. 113. 114. 115. 116. 117. 118. 119. 120. 121. 122. 123. 124. 125. 126. patients with advanced heart failure. Altern Ther Health Med. 1997;3: 51–59. Bernardi L, Porta C, Spicuzza L, Bellwon J, Spadacini G, Frey AW, Yeung LY, Sanderson JE, Pedretti R, Tramarin R. Slow breathing increases arterial baroreflex sensitivity in patients with chronic heart failure. Circulation. 2002;105:143–145. Weiner P, Waizman J, Magadle R, Berar-Yanay N, Pelled B. Effect of specific inspiratory muscle training on dyspnea and exercise tolerance in congestive heart failure. Harefuah. 1999;136:774 –777, 843. Mangin L, Monti A, Medigue C, Macquin-Mavier I, Lopes M, Gueret P, Castaigne A, Swynghedauw B, Mansier P. Altered baroreflex gain during voluntary breathing in chronic heart failure. Eur J Heart Fail. 2001;3:189 –195. Swanson KS, Gevirtz RN, Brown M, Spira J, Guarneri E, Stoletniy L. The effect of biofeedback on function in patients with heart failure. Appl Psychophysiol Biofeedback. 2009;34:71–91. Pace TW, Negi LT, Adame DD, Cole SP, Sivilli TI, Brown TD, Issa MJ, Raison CL. Effect of compassion meditation on neuroendocrine, innate immune and behavioral responses to psychosocial stress. Psychoneuroendocrinology. 2009;34:87–98. Jayadevappa R, Johnson JC, Bloom BS, Nidich S, Desai S, Chhatre S, Raziano DB, Schneider R. Effectiveness of transcendental meditation on functional capacity and quality of life of African Americans with congestive heart failure: a randomized control study. Ethnic Dis. 2007;17: 72–77. Benson H, Kotch JB, Crassweller KD. The relaxation response: a bridge between psychiatry and medicine. Med Clin North Am. 1977;61: 929 –938. Benson H, Greenwood MM, Klemchuk H. The relaxation response: psychophysiologic aspects and clinical applications. Int J Psychiatry Med. 1975;6:87–98. Benson H, Beary JF, Carol MP. The relaxation response. Psychiatry. 1974;37:37– 46. Walton KG, Schneider RH, Nidich S. Review of controlled research on the transcendental meditation program and cardiovascular disease. risk factors, morbidity, and mortality. Cardiol Rev. 2004;12:262–266. Barnes VA, Treiber FA, Turner JR, Davis H, Strong WB. Acute effects of transcendental meditation on hemodynamic functioning in middle-aged adults. Psychosom Med. 1999;61:525–531. Barnes VA, Treiber FA, Davis H. Impact of transcendental meditation on cardiovascular function at rest and during acute stress in adolescents with high normal blood pressure. J Psychosom Res. 2001;51:597– 605. Wenneberg SR, Schneider RH, Walton KG, Maclean CR, Levitsky DK, Salerno JW, Wallace RK, Mandarino JV, Rainforth MV, Waziri R. A controlled study of the effects of the transcendental meditation program on cardiovascular reactivity and ambulatory blood pressure. Int J Neurosci. 1997;89:15–28. Sivasankaran S, Pollard-Quintner S, Sachdeva R, Pugeda J, Hoq SM, Zarich SW. The effect of a six-week program of yoga and meditation on brachial artery reactivity: do psychosocial interventions affect vascular tone? Clin Cardiol. 2006;29:393–398. Phongsuphap S, Pongsupap Y, Chandanamattha P, Lursinsap C. Changes in heart rate variability during concentration meditation. Int J Cardiol. 2008;130:481– 484. Wu SD, Lo PC. Inward-attention meditation increases parasympathetic activity: a study based on heart rate variability. Biomed Res. 2008;29: 245–250. Kiecolt-Glaser JK, Christian L, Preston H, Houts CR, Malarkey WB, Emery CF, Glaser R. Stress, inflammation, and yoga practice. Psychosom Med. 2010;72:113–121. De Jong MJ, Moser DK, An K, Chung ML. Anxiety is not manifested by elevated heart rate and blood pressure in acutely ill cardiac patients. Eur J Cardiovasc Nurs. 2004;3:247–253. Yeh GY, Wayne PM, Phillips RS. T’ai chi exercise in patients with chronic heart failure. Med Sport Sci. 2008;52:195–208. Yeh GY, Wood MJ, Lorell BH, Stevenson LW, Eisenberg DM, Wayne PM, Goldberger AL, Davis RB, Phillips RS. Effects of tai chi mind-body movement therapy on functional status and exercise capacity in patients with chronic heart failure: a randomized controlled trial. Am J Med. 2004;117:541–548. Curiati JA, Bocchi E, Freire JO, Arantes AC, Braga M, Garcia Y, Guimaraes G, Fo WJ. Meditation reduces sympathetic activation and improves the quality of life in elderly patients with optimally treated heart failure: a prospective randomized study. J Altern Complement Med. 2005;11:465– 472. Emani and Binkley Downloaded from http://circheartfailure.ahajournals.org/ by guest on June 15, 2017 127. Kostis JB, Rosen RC, Cosgrove NM, Shindler DM, Wilson AC. Nonpharmacologic therapy improves functional and emotional status in congestive heart failure. Chest. 1999;106:996 –1001. 128. Klaus L, Beniaminovitz A, Choi L, Greenfield F, Whitworth GC, Oz MC, Mancini DM. Pilot study of guided imagery use in patients with severe heart failure. Am J Cardiol. 2000;86:101–104. 129. Yu DS, Lee DT, Woo J. Effects of relaxation therapy on psychologic distress and symptom status in older Chinese patients with heart failure. J Psychosom Res. 2007;62:427– 437. 130. Chang BH, Hendricks A, Zhao Y, Rothendler JA, LoCastro JS, Slawsky MT. A relaxation response randomized trial on patients with chronic heart failure. J Cardiopulm Rehabil. 2005;25:149 –157. 131. Luskin F, Reitz M, Newell K, Quinn TG, Haskell W. A controlled pilot study of stress management training of elderly patients with congestive heart failure. Prev Cardiol. 2002;5:168 –172. 132. Pischke CR, Weidner G, Elliott-Eller M, Ornish D. Lifestyle changes and clinical profile in coronary heart disease patients with an ejection fraction of 40% in the multicenter lifestyle demonstration project. Eur J Heart Fail. 2007;9:928 –934. 133. Sullivan MJ, Wood L, Terry J, Brantley J, Charles A, McGee V, Johnson D, Krucoff MW, Rosenberg B, Bosworth HB, Adams K, Cuffe MS. The support, education, and research in chronic heart failure study (SEARCH): a mindfulness-based psychoeducational intervention improves depression and clinical symptoms in patients with chronic heart failure. Am Heart J. 2009;157:84 –90. 134. Rozanski A, Blumenthal JA, Davidson KW, Saab PG, Kubzansky L. The epidemiology, pathophysiology, and management of psychosocial risk factors in cardiac practice: the emerging field of behavioral cardiology. J Am Coll Cardiol. 2005;45:637– 651. 135. Aquilante CL, Terra SG, Schofield RS, Pauly DF, Hatton PS, Binkley PF, Johnson JA. Sustained restoration of autonomic balance with longbut not short-acting metoprolol in patients with heart failure. J Card Fail. 2006;12:171–176. 136. Panina G, Khot UN, Nunziata E, Cody RJ, Binkley PF. Role of spectral measures of heart rate variability as markers of disease progression in 137. 138. 139. 140. 141. 142. 143. 144. Mind-Body Medicine in CHF 725 patients with chronic congestive heart failure not treated with angiotensin-converting enzyme inhibitors. Am Heart J. 1996;131:153–157. Panina G, Khot UN, Nunziata E, Cody RJ, Binkley PF. Assessment of autonomic tone over a 24-hour period in patients with congestive heart failure: relation between mean heart rate and measures of heart rate variability. Am Heart J. 1995;129:748 –753. Binkley PF, Nunziata E, Cody RJ. Influence of flosequinan on autonomic tone in congestive heart failure: implications for the mechanism of the positive chronotropic effect and survival influence of long-term vasodilator administration. Am Heart J. 1994;128:1147–1156. Yeh GY, Davis RB, Phillips RS. Use of complementary therapies in patients with cardiovascular disease. Am J Cardiol. 2006;98:673– 680. Haynes PL. The role of behavioral sleep medicine in the assessment and treatment of sleep disordered breathing. Clin Psychol Rev. 2005;25: 673–705. Jiang W, O’Connor C, Silva SG, Kuchibhatla M, Cuffe MS, Callwood DD, Zakhary B, Henke E, Arias RM, Krishnan R, SADHART-CHF Investigators. Safety and efficacy of sertraline for depression in patients with CHF (SADHART-CHF): a randomized, double-blind, placebocontrolled trial of sertraline for major depression with congestive heart failure. Am Heart J. 2008;156:437– 444. O’Connor CM. Safety and efficacy of sertraline for depression in patients with congestive heart failure (SADHART-CHF; Abstract). Heart Failure Society of American 2008 scientific meeting: September 22, 2008; Toronto, Ontario. Late-Breaking Clinical Trials 1. Bozzini S, Gambelli P, Boiocchi C, Schirinzi S, Falcone R, Buzzi P, Storti C, Falcone C. Coronary artery disease and depression: possible role of brain-derived neurotrophic factor and serotonin transporter gene polymorphisms. Int J Mol Med. 2009;2:813– 818. Ornish D, Lin J, Daubenmier J, Weidner G, Epel E, Kemp C, Magbanua MJ, Marlin R, Yglecias L, Carroll PR, Blackburn EH. Increased telomerase activity and comprehensive lifestyle changes: a pilot study. Lancet Oncol. 2008;9:1048 –1057. KEY WORDS: Vagus nerve 䡲 sympathetic nervous system nervous system 䡲 inflammation 䡲 autonomic function 䡲 autonomic Mind-Body Medicine in Chronic Heart Failure: A Translational Science Challenge Sitaramesh Emani and Philip F. Binkley Downloaded from http://circheartfailure.ahajournals.org/ by guest on June 15, 2017 Circ Heart Fail. 2010;3:715-725 doi: 10.1161/CIRCHEARTFAILURE.110.951509 Circulation: Heart Failure is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231 Copyright © 2010 American Heart Association, Inc. All rights reserved. Print ISSN: 1941-3289. Online ISSN: 1941-3297 The online version of this article, along with updated information and services, is located on the World Wide Web at: http://circheartfailure.ahajournals.org/content/3/6/715 Permissions: Requests for permissions to reproduce figures, tables, or portions of articles originally published in Circulation: Heart Failure can be obtained via RightsLink, a service of the Copyright Clearance Center, not the Editorial Office. Once the online version of the published article for which permission is being requested is located, click Request Permissions in the middle column of the Web page under Services. Further information about this process is available in the Permissions and Rights Question and Answer document. Reprints: Information about reprints can be found online at: http://www.lww.com/reprints Subscriptions: Information about subscribing to Circulation: Heart Failure is online at: http://circheartfailure.ahajournals.org//subscriptions/