Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Discovery and development of beta-blockers wikipedia , lookup
Drug interaction wikipedia , lookup
Norepinephrine wikipedia , lookup
Psychopharmacology wikipedia , lookup
Neuropharmacology wikipedia , lookup
Neuropsychopharmacology wikipedia , lookup
Discovery and development of ACE inhibitors wikipedia , lookup
Discovery and development of angiotensin receptor blockers wikipedia , lookup
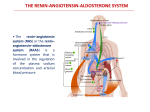
Antihypertensive agents Introduction • Hypertension is the most common CV disease • Definition: either a sustained SBP of greater than 140 mm Hg or a sustained DBP of greater than 90 mm Hg • HTN can lead to cerebrovascular accidents (strokes), CHF, MI, and renal damage • The incidence of morbidity and mortality significantly decreases when HTN is diagnosed early and is properly treated JNC 7 Blood Pressure (BP) Classification BP Classification Normal Systolic BP, mm Hg* Diastolic BP, mm Hg Lifestyle Modification <120 and <80 Encourage Prehypertension 120-139 or 80-89 Yes Stage 1 hypertension 140-159 or 90-99 Yes Stage 2 hypertension ≥160 or ≥100 Yes JNC 7 = seventh report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure. *Classification for ages 18 years and older. JNC 7. JAMA. 2003;289:2560-2572. Differing influence of hypertension on absolute and relative risk of stroke and MI 20 5 Year Risk (%) Normotensives Hypertensives 15 10 Stroke MI 5 0 0 20 40 60 80 100 120 140 160 180 200 220 240 260 280 300 Systolic Blood Pressure (mmHg) Brown, M.J. Lancet 2000; 355: 659 - 660 CV Disease Risk Doubles with Each 20/10 mm Hg BP Increment* 8 7 6 5 CV disease 4 3 risk 2 1 0 115/75 135/85 155/95 SBP/DBP (mm Hg) 175/105 *Individuals aged 40-70 years, starting at BP 115/75 mm Hg. CV, cardiovascular; SBP, systolic blood pressure; DBP, diastolic blood pressure 1. Lewington S, Cardiovascular Issues in Ageing Pilots. et al. Lancet. 2002; 60:1903-1913 2. The Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, And Treatment of High Blood Pressure. http://jama.ama-assn.org/cgi/content/full/289.19.2560v1. Assessed 5-1-08 Proportion of deaths attributable to leading risk factors worldwide (2000) High mortality, developing region Lower mortality, developing region Developed region 0 1 2 3 4 5 6 7 8 Attributable Mortality (In millions; total 55,861,000) Ezzati et al. WHO 2000 Report. Lancet. 2002;360:1347-1360. Etiology of HTN I. Essential or primary hypertension – Accounts for ˃90% of cases – No single identifiable cause (idiopathic) – It is usually caused by a combination of several (multifactorial) abnormalities – A number of factors increase the risk of developing essential HTN: age, genetics, environment (e.g. stress, sodium intake, alcohol), weight, and race Etiology of HTN II. Secondary hypertension – Account for 10-15% of cases – Secondary to a known organic disease, such as renovascular disease or pheochromocytoma – Correction of the underlying may result in a fall in BP Normal regulation of blood pressure • Arterial blood pressure is regulated within a narrow range to provide adequate perfusion of the tissues without causing damage to the vascular system, particularly the arterial intima (endothelium) • Arterial blood pressure is directly proportional to the product of the cardiac output and the peripheral vascular resistance • BP is maintained by moment-to-moment regulation of cardiac output and peripheral vascular resistance, exerted at four anatomic sites: arterioles, postcapillary venules (capacitance vessels), heart, & the kidney Determinants of Arterial Pressure Mean Arterial Pressure = Cardiac output X Peripheral resistance Heart Rate Contractility Filling Pressure Blood Volume Venous Tone Arteriolar Diameter Normal regulation of blood pressure • The function of these four control sites is controlled/coordinated mainly by two overlapping control mechanisms: a) The baroreflexes, which are mediated by the sympathetic nervous system b) The renin-angiotensin-aldosterone system • Regulation of blood pressure in hypertensive patients differs from healthy patients in that the baroreceptors and the renal blood volume-pressure control systems appear to be "set" at a higher level of blood pressure Activation of Baroreceptor Reflexes Renal Sympathetic Nerve Activity BLOOD PRESSURE BLOOD VOLUME Beta-adrenergic Stimulation RENIN SECRECTION Renal Artery Pressure Renal Baroreceptor Plasma Ang I Plasma Ang II Systemic Vasoconstriction Aldosterone Secretion BLOOD PRESSURE BLOOD VOLUME Ang, angiotensin. Reid IA. Adv Physiol Edu. 1998;20:S236-S245. Treatment Aims • The aim of therapy is straightforward: 1) Reduction of blood pressure to within the normal range 2) Reduction of CV and renal mortality & morbidity Population-Based Strategy SBP Distributions After Intervention Before Intervention Reduction in BP Reduction in SBP mmHg 2 3 5 % Reduction in Mortality Total CHD Stroke –3 –4 –7 –4 –5 –9 –6 –8 –14 Antihypertensive agents • Drugs lower blood pressure by actions on peripheral resistance, cardiac output, or both • All antihypertensive agents act at one or more of four anatomic control (arterioles, postcapillary venules, heart, & the kidney) and produce their effects by interfering with normal mechanisms of blood pressure regulation Antihypertensive agents • Antihypertensive agents can be categorized according to the principal regulatory site or mechanism on which they act: 1. Diuretics 2. Direct vasodilators 3. Sympathoplegic agents 4. Agents that block production or action of angiotensin Treatment strategies • Monotherapy of hypertension (treatment with a single drug) is desirable because compliance is likely to be better and cost is lower, and because in some cases adverse effects are fewer • Most patients with HTN require two or more drugs (polypharmacy), if BP is inadequately controlled with a monotherapy, with the selection based on minimizing the adverse effects of the combined regimen Treatment strategies • It is important to match antihypertensive drugs to the particular patient • It is important to enhance compliance by carefully selecting a drug regimen that both reduces adverse effects and minimizes the number of doses required daily • HTN may coexist with other diseases that can be aggravated by some of the antihypertensive drugs JNC 7: Compelling Indications for Individual Drug Classes High-Risk Condition With Compelling Indication* Heart failure Recommended Drugs Diuretic x Post-MI BetaACE Blocker Inhibitor x x x x ARB x x x x Diabetes x x x x x x Recurrent stroke prevention x Aldo Ant x x High CAD risk Chronic kidney disease CCB x x x MI = myocardial infarction; CAD=coronary artery disease; Aldo Ant = aldosterone antagonist. *Based on benefits from outcome studies or existing guidelines, the compelling indication is managed in parallel with the BP. JNC 7. JAMA. 2003;289:2560-2672. Treatment strategies • In the general nonblack population initial antihypertensive treatment should include a thiazide-type diuretic, CCB, ACEI, or ARB* • In the general black population initial antihypertensive treatment should include a thiazide-type diuretic or CCB* * I. Diuretics Diuretics • Diuretics alone often provide adequate treatment for mild or moderate essential HTN • Low-dose diuretic therapy is safe, inexpensive, and effective in preventing stroke, MI, and CHF, all of which can cause mortality • Diuretics are used in combination with sympathoplegic and vasodilator drugs to reverse Na+ and H2O retention observed with other antihypertensive agents Diuretics • Thiazides are the most frequently used class of antihypertensive agents • Thiazide diuretics are appropriate for most patients with mild or moderate hypertension and normal renal and cardiac function • Loop diuretics (e.g. furosemide) are used in moderate, severe, and malignant hypertension • K+-sparing duiretics can be employed in conjunction with other types of diuretics to help alleviate the K+ loss caused by thiazide and loop diuretics Diuretics Mechanism of action I. Initially, diuretics lower BP by increasing Na+ and H2O excretion, causing a decrease in blood volume and cardiac output II. With long-term treatment, cardiac output returns toward normal while peripheral vascular resistance declines. The explanation for the long-term vasodilation induced by these drugs is unknow Na+, H2O retention Blood volume Perpheral resistance Decreased in blood pressure Cardiac output II. Sympathoplegic agents Drugs that Alter Sympathetic Nervous System Function • Sympathoplegics are drugs that reduce BP by depressing the function of the sympathetic control of CV function • Are subdivided by anatomic site of action: 1. CNS-active agents: they reduce sympathetic outflow from vasomotor centers in the brainstem and allow these centers to retain or even increase their sensitivity to baroreceptor control 2. Ganglionic blocking drugs (e.g. hexamethonium and trimethophan) Drugs that Alter Sympathetic Nervous System Function 3. Postganglionic sympathetic nerve terminal blockers: either by inhibiting neurotransmitter release (e.g. guanithidine) or by depleting the stores of norepinephrine (e.g. reserpine) 4. Adrenoceptor blockers: by antagonizing the actions of norepinephrine on effector cells Brain Brain Stem (Cardiovascular Control Center) a2 Receptors Sympathetic ganglion b1 Receptors Heart b1 Receptors Kidney a1 Receptors Drugs that Alter Sympathetic Nervous System Function • All can elicit compensatory effects through mechanisms that are not dependent on adrenergic nerves • The antihypertensive effect of any of these agents used alone may be limited by retention of sodium by the kidney and expansion of blood volume • Sympathoplegic antihypertensive drugs are effective when used concomitantly with a diuretic most Centrally acting sympathoplegic drugs Clonidine • It stimulate the α2A subtype of α2 adrenergic receptors in the brainstem, resulting in a reduction in sympathetic outflow from the CNS & increase in the parasympathetic tone • Blood pressure lowering results by an effect on both cardiac output and peripheral resistance • Clonidine decreases renal vascular resistance and maintenance of renal blood flow and, therefore, is useful in the treatment of HTN complicated by renal disease Centrally acting sympathoplegic drugs Clonidine • The most common: sedation, dry mouth, and drowsiness • Severe hypertensive crisis mediated when clonidine is suddenly withdrawn • Concomitant treatment with TCA may block the antihypertensive effect of clonidine Centrally acting sympathoplegic drugs α-Methyldopa • • • • • It is now used primarily for HTN during pregnancy It rapidly enters the brain, where it accumulates in noradrenergic nerves, is converted to αmethylnorepinephrine (α2 adrenergic receptors agonist), and is released Renal blood flow and GFR are not reduced The most common undesirable effect of methyldopa is sedation and drawsiness Other side effects include hyperprolactinemia Postganglionic sympathatic nerve terminal blockers Guanethidine • Powerful antihypertensive agent • It exerts its effects at peripheral sympathetic nerve endings • Guanethidine is transported across the sympathetic nerve membrane by the same mechanism that transports norepinephrine itself (NET, uptake 1), and uptake is essential for the drug's action Postganglionic sympathatic nerver terminal blockers Guanethidine • Once it has entered the nerve, it is concentrated in transmitter vesicles, where it replaces norepinephrine, causing a gradual depletion of norepinephrine stores in the nerve ending • The onset of sympathoplegia is gradual (maximal effect in 1–2 weeks), and sympathoplegia persists for a comparable period after cessation of therapy Postganglionic sympathatic nerver terminal blockers Guanethidin • Undesirable effects that are related entirely to sympathetic blockade: postural hypotension, sexual dysfunction, and diarrhea • Drugs that block the catecholamine uptake process block guanethidine effects: cocaine and TCA • Sympathomimetic agents, at doses available in OTC cold preparations, can produce hypertension in patients taking guanethidine • Guanethidine can produce releasing catecholamines pheochromocytoma hypertensive crisis by in patients with Postganglionic sympathatic nerver terminal blockers Reserpin • Reserpine binds tightly to vesicular membraneassociated transporter (VMAT) in central and peripheral adrenergic neurons resulting in depletion of norepinephrine, dopamine, and serotonin • SE effects: – CNS: sedation, severe mental depression, & extrapyramidal effects resembling Parkinson's disease – PNS: nasal congestion, postural hypotension, diarrhea, bradycardia, increased gastric secretion, and impotence Adrenoceptor antagonist • Agents: β-blockers and α1-blockers • Useful for lowering BP in mild to moderate HTN • Especially useful in preventing the reflex tachycardia that often results from treatment with direct vasodilators • Beta-blockers are recommended first-line drug therapy for HTN when concomitant disease is present (e.g. MI and CHF) III. Vasodilators Vasodilators • All of these agents relax smooth muscle of arterioles, thereby decreasing systemic vascular resistance • The induced vasodilation is associated with powerful stimulation of the sympathetic nervous system, likely due to baroreceptor-mediated reflexes • Vasodilators act by four major mechanisms: 1) Release of nitric oxide 2) Opening of potassium channels 3) Blockade of calcium channels 4) Activation of D1 dopamine receptors Sites of action of drugs that relax vascular smooth muscle a-Adrenoceptor antagonists Prazosin Terazosin Activators of the NO/guanylate cyclase pathway Hydralazine Nitroglycerin Nitroprusside Ca2+-channel blockers Dihydropyridines Verapamil Ca2+ Diltiazem NO K+ Angiotensin II receptor antagonists Losartan Valsartan K+-channel activators Minoxidil Diazoxide Vasodilators • 1. 2. 3. Vasodilators include: Oral vasodilators (e.g. hydralazine and minoxidil): used for long-term outpatient therapy of HTN Parenteral vasodilators (e.g. nitroprusside, diazoxide, and fenoldopam): used to treat hypertensive emergencies Calcium channel blockers (CCBs) (e.g. amlodipine, diltiazem, felodipine,..etc) Oral Vasodilators Hydralazine • Its actions are largely confined to vascular smooth muscle and occur predominantly on the arteries & arteriole • Hydralazine apparently acts through the release of NO from endothelial cells • Its toxicity include compensatory responses (tachycardia, water and salt retention) and immunological reactions chiefly in slow acetylator the drug (arthralgia, myalgia, skin rashes, and fever that resembles lupus erythematosus) Oral Vasodilators Minoxidill • Minoxidil sulfate, the active metabolite, activates the ATP-modulated K+ channel • By opening K+ channels in smooth muscle and thereby permitting K+ efflux, it causes hyperpolarization and relaxation of smooth muscle • The use of minoxidil is associated with severe compensetary responses (reflex tachycardia, sodium and fluid retention) and hypertrichosis (hirsutism) Parenteral Vasodilators Sodium Nitroprusside • Used in treating hypertensive emergencies: its onset of action is within 30 seconds; the peak hypotensive effect occurs within 2 minutes • Nitroprusside is a nitrovasodilator that acts by releasing NO, which activates the guanylyl cyclasecyclic GMP-PKG pathway, leading to vasodilation • Nitroprusside dilates both arterial and venous vessels, resulting in reduced peripheral vascular resistance and venous return Parenteral Vasodilators Sodium Nitroprusside • • In the absence of heart failure, blood pressure decreases, owing to decreased vascular resistance, whereas cardiac output does not change or decreases slightly Sodium nitroprusside is an unstable molecule that decomposes under strongly alkaline conditions or when exposed to light. Infusion solutions should be changed after several hours Parenteral Vasodilators Sodium Nitroprusside 1) Excessive hypotension: close monitoring of blood pressure and the use of a continuous variable-rate infusion pump will prevent an excessive hemodynamic response 2) Accumulation of cyanide (metabolic acidosis, arrhythmias, excessive hypotension): usually occurs when sodium nitroprusside is infused at a rate greater than 5 mg/kg per minute. Concomitant administration of sodium thiosulfate can prevent accumulation of cyanide Parenteral Vasodilators Sodium Nitroprusside 3) Accumulation of thiocyanate (weakness, disorientation, psychosis, muscle spasms, convulsions, and rarely hypothroidism) particularly in patients with renal insufficiency: thiocyanate can be removed readily by hemodialysis Parenteral Vasodilators Diazoxide • • • • • Diazoxide is an effective and relatively long-acting parenterally administered that is occasionally used to treat hypertensive emergencies Its onset of action is within 5 minutes and lasts for 4–12 hours Diazoxide opens potassium channels, thus hyperpolarizing and relaxing smooth muscle cells Diazoxide inhibits insulin release from the pancreas and is used to treat hypoglycemia secondary to insulinoma Diazoxide toxicities include has been excessive hypotension, hyperglycemia, and salt and water retention Parenteral Vasodilators Fenoldopam • • • • It is a peripheral arteriolar dilator used for hypertensive emergencies and postoperative hypertension It acts primarily as an agonist of dopamine D1 receptors, resulting in dilation of peripheral arteries and natriuresis Administered by continuous intravenous infusion The major ADEs are reflex tachycardia, headache, flushing, and an increase intraocular pressure (avoided in patients with glaucoma) Vasodilators Calcium channel blockers (CCBs) • Agents: verapamil, diltiazem, and dihydropyridine • Dihydropyridines include: amlodipine, felodipine, isradipine, nicardipine, nifedipine, and nisoldipine • All of the Ca2+ channel blockers lower blood pressure by relaxing arteriolar smooth muscle and decreasing peripheral vascular resistance • Verapamil and diltiazem have depressant effect on the heart and may decrease heart rate and cardiac output. Therefore, tachycardia is typically minimal to absent with verapamil and diltiazem Vasodilators Calcium channel blockers (CCBs) • Dihydropyridine agents are more selective as vasodilators and have less cardiac depressant effect than verapamil and diltiazem • Reflex sympathetic activation with slight tachycardia maintains or increases cardiac output in most patients given dihydropyridines IV. Inhibitors of angiotensin Introduction • The renin–angiotensin system (RAS) is important for the regulation of vascular smooth muscle tone, fluid and electrolyte balance, and the growth of cardiac and vascular smooth muscle • It participates significantly in the pathophysiology of HTN, CHF, MI, diabetic nephropathy, and atherosclerosis Introduction • RAS comprises a series of biochemical steps leading to the production of a family of structurally related peptides (e.g., angiotensin II, angiotensin III, and other smaller peptides with bioactivity) • Renin is a proteolytic enzyme that is secreted by the juxtaglomerular apparatus Angiotensinogen NH2-Asp-Arg-Val…Pro-Phe-Hist-Leu…COOH 1 2 3 7 8 9 10 Renin None-ACE pathways (eg. Chymase) Angiotensin I NH2-Asp-Arg-Val…Pro-Phe-COOH 1 2 3 7 8 9 10 ACE Angiotensin II NH2-Asp-Arg-Val…Pro-Phe-COOH 1 2 3 7 8 aminopeptidase Angiotensin III NH2-Arg-Val…Pro-Phe-COOH 2 Angiotensinases Peptide fragments 3 7 8 Introduction • Three generally accepted mechanisms are involved in the regulation of renin secretion: 1. Reduced renal arterial pressure 2. Sympathetic neural stimulation 3. Reduced Na+ delivery at the distal renal tubule Blood Pressure Rises Blood Volume Rises Blood Pressure Falls - Renin Release + Na+ Retention Vasoconstriction Aldosterone Secretion Blood Volume Falls Na+ Depletion Angiotensin Formation A schematic portrayal of the homeostatic roles of the renin-angiotensin system Angiotensin II receptors • The effects of ang II are exerted through specific G protein-coupled receptors • Angiotensin receptors have been classified into two subtypes: AT1 and AT2 • The major biological functions of ang II (CV regulation) are mediated through the AT1 receptor • AT1 is located predominantly in vascular and myocardial tissue and also in brain, kidney, and adrenal glomerulosa cells Angiotensin II receptors • Effects mediated by AT1 receptors include: 1. Generalized vasoconstriction, especially marked in efferent arterioles of the kidney 2. Increased release of noradrenaline from sympathetic nerve terminals, reinforcing vasoconstriction and increasing the rate and force of contraction of the heart 3. Stimulation of proximal tubular reabsorption of Na+ 4. Secretion of aldosterone from the adrenal cortex 5. Cell growth in the heart and in arteries Inhibitors of angiotensin • Three classes of drugs act specifically on the reninangiotensin system: I. Angiotensin-converting enzyme inhibitors (ACEI) II. Angiotensin II receptor antagonists (sartans) III. Renin inhibitors (e.g. aliskiren) Inhibitors of angiotensin Angiotensin-converting enzyme (ACE) inhibitors • Agents: captopril, enalapril, lisinopril, benazepril, fosinopril, moexipril, perindopril, quinapril, ramipril, and trandolapril • Vasodilatory activity results both from an inhibitory action on the renin-angiotensin system (lower vasoconstriction) and a stimulating action on the kallikrein-kinin system (increased bradykinin) • ACEIs decrease the secretion of aldosteronem resulting in decreased sodium and water retention Angiotensinogen Bradykinin Renin None-ACE pathways (eg. Chymase) Angiotensin I Bradykinin ACE Inactive peptide Angiotensin II vasodilation of vascular smooth muscles ACEI AT2R AT1R Aldosterone Vasoconstriction ↑ sympathatic activity Sympathatic output Na+, H2O retention Inhibitors of angiotensin Angiotensin-converting enzyme (ACE) inhibitors • ACEIs do not result in reflex sympathetic activation and can be used safely in persons with IHD • Because the renal vessels are extremely sensitive to the vasoconstrictor actions of AngII, ACEIs increase renal blood flow via vasodilation of the afferent and efferent arterioles • The ACE inhibitors appear to confer a special advantage in the treatment of patients with diabetes, slowing the development and progression of diabetic glomerulopathy Inhibitors of angiotensin ACE inhibitors- ADRs 1) Hypotention: after initial doses of any ACE inhibitor in patients who are hypovolemic (e.g. diuretics) 2) Dry cough (5% to 20% of patients) due to increased level of bradykinin in the pulmonary tree • Thromboxane antagonism, aspirin, and iron supplementation reduce cough induced by ACE inhibitors • ACE dose reduction or switching to an ARB is sometimes effective 3) Angioedema (0.1% to 0.5% of patients) Inhibitors of angiotensin ACE inhibitors- ADRs 4) Hyperkalemia: patients with renal insufficiency or in patients taking K+-sparing diuretics, K+ supplements, βblockers, or NSAIDs 5) Acute renal failure: Captopril, particularly when given in high doses to patients with renal insufficiency, may cause neutropenia or proteinuria • ACEI are contraindicated during the 2nd and 3rd trimesters of pregnancy because of the risk of fetal hypotension, anuria, and renal failure, sometimes associated with fetal malformations or death Inhibitors of angiotensin Angiotensin Receptor–Blockers (ARBs) • Agents: losartan, valsartan, candesartan, eprosartan, irbesartan, telmisartan, and olmesartan • Non-peptide competitive angiotensin II receptor antagonists of the AT1 • Their pharmacologic effects are similar to those of ACEI in that they produce vasodilation and block aldosterone secretion • More selective blockers of angiotensin effects than ACEI and have no effect on bradykinin metabolism Renin Angiotensinogen Angiotensin I ACE X X Aldosterone secretion Renal tubular reabsorption of sodium and water Angiotensin II Non-ACE alternate pathways (eg, chymase) ARB Vasoconstriction AT1 receptors Catecholamine secretion Antidiuretic hormone (vasoprressin) secretion X X X X Stimulation of thirst center BP Inhibitors of angiotensin Angiotensin Receptor–Blocking Agents • Provide benefits similar to those of ACE inhibitors in patients with HF and chronic kidney disease • Their ADEs are simillar to those of ACEI • Unlike ACE inhibitors, ARBs do not cause cough, and the incidence of angioedema with ARBs is much less than with ACE inhibitors Inhibitors of angiotensin Selective renin inhibitor: Aliskiren • Aliskiren functions by blocking the catalytic functions of this enzyme by binding to the active site of renin, which inhibits the conversion of angiotensinogen to angiotensin I and reduces angiotensin II concentrations • It lowers BP as effectively as ARBs, ACEI, and thiazides • It can also be combined other antihypertensives, such diuretics, ACEIs, ARBs, or CCBs Direct renin inhibitor Angiotensinogen Renin Ang I Heart Non ACE pathways Kidney ACE Vessels ACEIs Feedback Loop Vasoconstriction Remodelling Ang II ARBs AT1 Receptor ACEI ARB Aliskiren Ang I Ang II Renin PRA ↑ ↑ ↓ ↓ ↑ ↓ ↑ ↑ ↑ ↑ ↑ ↓ Azizi M et al. 2006; Adapted from: Müller DN & Luft FC. 2006 Inhibitors of angiotensin Selective renin inhibitor: Aliskiren • Adverse effects include: 1) Mild GIT symptoms: diarrhea observed at high doses (600 mg daily), abdominal pain, dyspepsia, and gastroesophageal reflux 2) Others: headache; nasopharyngitis; dizziness; fatigue; upper-respiratory tract infection; back pain; angiodema; cough (cough was much less common than with ACE inhibitors, rash, hypotension, hyperkalemia in diabetics on combination therapy, elevated uric acid, renal stones, and gout • It is contraindicated during pregnancy