Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
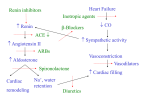
Management of CHF Diagnosis of CHF The clinical features of heart failure include symptoms such as: ankle swelling exertional breathlessness fatigue orthopnoea paroxysmal nocturnal dyspnoea (PND) nocturia anorexia weight loss And signs such as: tachycardia reduced pulse volume pulsus alternans raised JVP - in right heart failure oedema rales, or basal crepitations hepatomegaly ascites Investigations for Heart Failure chest radiology the ECG may elucidate the cause of heart failure: o left ventricular hypertrophy which may be caused by chronic hypertension or aortic stenosis o evidence of ischaemic heart disease o p-mitrale of mitral stenosis echocardiography identifies: o focal or diffuse myocardial dysfunction o valvular disease o pericardial disease o left ventricular systolic dysfunction biochemistry, haematology and urinalysis: o defines electrolyte disturbances and assesses renal function o excludes anaemia o exclude thyrotoxicosis in patients with atrial fibrillation o excludes causes of oedema such as liver disease, nephrotic syndrome and acute renal failure o natriuretic peptides - testing for Brain-type natriuretic peptide (BNP), atrial natriuretic peptide (ANP), and N-terminal (NT)-ANP has been shown to increase the reliability of diagnosis of heart failure in primary care these peptides are released from ventricular myocytes in response to volume overload (stretch), and their concentration has been shown to an extremely sensitive marker for heart failure Other possible investigations include: o radionuclide ventriculography e.g. MUGA scan o a myocardial biopsy to obtain histological data NICE suggest that BNP measurement be undertaken in conjunction with ECG and history and examination, before referral from primary care for echocardiography to confirm the diagnosis of heart failure (1): the NICE clinical guideline on CHF recommends that those suspected of having heart failure because of their history, signs and symptoms should have a 12-lead ECG and/or BNP, with echocardiography being performed where the result of either is abnormal (2) General management of CHF the primary cause of heart failure should be treated where this is appropriate: o hypertension o anaemia o hypoxia o valve disease bed rest: o erect posture and exercise exacerbate renal vasoconstriction dietary modification: o salt restriction: daily intake of 20-30 mmol is optimal but unpleasant daily intake of 100 mmol is more realistic measure daily urinary sodium to monitor intake o alcohol in moderation only fluid restriction 500-1000 ml/day may be beneficial in severe heart failure stop smoking maintain optimal weight Three types of drug treatment have been shown to reduce morbidity and mortality in patients with heart failure: angiotensin converting enzyme (ACE) inhibitors the aldosterone antagonist spironolactone beta-blockers Treatment of mild to moderate congestive cardiac failure consists of: diuretics, for symptom control ACE inhibitor * o NICE recommends that all patients with left ventricular dysfunction should be taking an ACE inhibitor (1,2): ACE inhibitor therapy should be initiated before beta blockade specialist referral is required for patients requiring high doses of diuretics, or exhibiting worsening renal function at any stage - note that some degree of detioration of renal function after initiating ACE inhibitors is inevitable, but if this is only small only monitoring is necessary beta-blocker o beta-blockers should only be prescribed for chronic heart failure patients after stabilisation on ACE inhibitor therapy - beta-blocker therapy should be started at a very low dose (e.g. carvedilol 3.125mg once daily) and titrated slowly over a period of weeks or months. The beta-blocker should be up-titrated at fortnightly intervals (or longer in more sensitive patients) to a target dose of carvedilol 25-50mg bd or bisoprolol 10mg od (1,2) spironolactone o NICE recommend spironolactone to be prescribed to patients with moderately-severely compromised left ventricular dysfunction, as an addon to other therapies, with careful monitoring of serum potassium (1) angiotensin receptor blocker o NICE recommend that angiotensin receptor blockers are not used as primary therapy for heart failure, but are reserved for use in patients who are intolerant of ACE inhibitors (1) o there may also be a role for angiotensin receptor blockers as 'add-on' therapy in management of refractory heart failure (1,2) Other therapies include: digoxin o NICE recommends digoxin for use in patients with atrial fibrillation and heart failure, or those in whom symptoms are progressing on ACE inhibitors, beta-blocker and diuretic therapy Implantable cardiac defibrillators (ICDs) : the Sudden Cardiac Death in Heart Failure (SCD-HeFT) (4) provides evidence for the prophylactic use of ICDs in patients with congestive heart failure (CHF). This trial showed that in patients with CCF, a conservatively programmed, shock only ICF reduced all cause mortality. In comparison with placebo, ICD reduced mortality in New York Heart Association (NYHA) class II but not class III CHF. The SCD-HeFT also included an amiodarone arm, which showed no benefit in the primary prevention of cardiac death *ACE inhibitors in cardiac failure: they improve symptoms and signs, such as exercise capacity they decrease systemic vascular resistance, venous pressure and levels of circulating catecholamines they prolong survival in patients with mild to moderate severe heart failure (CONSENSUS and SOLVD trials). In addition V-HeFT II showed improved survival with enalapril over a hydralazine and isosorbide dinitrate regimen (24 months follow up) These drugs actually reduce mortality by up to 50%; this is the reason the consensus trial was prematurely halted. There is also reduced number of "events", which includes prevention of hospitalisation and premature deaths, with obvious economic benefits. Management of Severe Heart failure Patients with severe chronic heart failure may be receiving a treatment regime including diuretics, ACE inhibitors, beta-blockers and spironolactone. Patients with extremely resistant oedema may also be given additional therapies. These may include: loop diuretic potentiated with a thiazide diuretic such as metolazone nitrate vasodilator digoxin Heart transplantation is a treatment of last resort in selected patients with severe heart failure