Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Amino acid synthesis wikipedia , lookup
Lipid signaling wikipedia , lookup
Biosynthesis wikipedia , lookup
Metalloprotein wikipedia , lookup
Basal metabolic rate wikipedia , lookup
Evolution of metal ions in biological systems wikipedia , lookup
Specialized pro-resolving mediators wikipedia , lookup
Glyceroneogenesis wikipedia , lookup
Citric acid cycle wikipedia , lookup
Butyric acid wikipedia , lookup
Biochemistry wikipedia , lookup
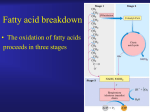
Review Cardiovascular Research (2008) 79, 259–268 doi:10.1093/cvr/cvn130 The malonyl CoA axis as a potential target for treating ischaemic heart disease John R. Ussher and Gary D. Lopaschuk* Cardiovascular Research Group, Department of Pediatrics, University of Alberta, Edmonton, Canada Received 23 January 2008; revised 11 May 2008; accepted 16 May 2008; online publish-ahead-of-print 22 May 2008 Time for primary review: 20 days KEYWORDS Ischaemic heart disease; Malonyl CoA; Malonyl CoA decarboxylase; Acetyl CoA carboxylase; AMP-activated protein kinase; Fatty acid oxidation Cardiovascular disease is the leading cause of death and disability for people living in western societies, with ischaemic heart disease accounting for the majority of this health burden. The primary treatment for ischaemic heart disease consists of either improving blood and oxygen supply to the heart or reducing the heart’s oxygen demand. Unfortunately, despite recent advances with these approaches, ischaemic heart disease still remains a major health problem. Therefore, the development of new treatment strategies is still required. One exciting new approach is to optimize cardiac energy metabolism, particularly by decreasing the use of fatty acids as a fuel and by increasing the use of glucose as a fuel. This approach is beneficial in the setting of ischaemic heart disease, as it allows the heart to produce energy more efficiently and it reduces the degree of acidosis associated with ischaemia/reperfusion. Malonyl CoA is a potent endogenous inhibitor of cardiac fatty acid oxidation, secondary to inhibiting carnitine palmitoyl transferase-I, the rate-limiting enzyme in the mitochondrial uptake of fatty acids. Malonyl CoA is synthesized in the heart by acetyl CoA carboxylase, which in turn is phosphorylated and inhibited by 50 AMP-activated protein kinase. The degradation of myocardial malonyl CoA occurs via malonyl CoA decarboxylase (MCD). Previous studies have shown that inhibiting MCD will significantly increase cardiac malonyl CoA levels. This is associated with an increase in glucose oxidation, a decrease in acidosis, and an improvement in cardiac function and efficiency during and following ischaemia. Hence, the malonyl CoA axis represents an exciting new target for the treatment of ischaemic heart disease. 1. Introduction Cardiovascular disease (CVD) is a major health problem worldwide, and it is predicted to be the number one killer by 2010.1 The underlying cause for the majority living with CVD is a diminished oxygen supply to the cardiac muscle, termed ‘ischaemic heart disease’. Fortunately, epidemiological studies and randomized clinical trials have provided compelling evidence that ischaemic heart disease is largely manageable.2 Current treatment regimens, which consist of either percutaneous or surgical techniques to improve myocardial blood supply, or pharmacotherapy to limit myocardial oxygen demand, have greatly aided in the overall prognosis of ischaemic heart disease patients. Yet, there are still patients who prove to be ineligible or refractory to conventional treatment, and percutaneous or surgical revascularization is associated with a distinct set of risks. Therefore, new approaches to treat such patients are necessary. One such * Corresponding author: 423 Heritage Medical Research Center, University of Alberta, Edmonton, Canada T6G 2S2. Tel: þ1 780 492 2170; fax: þ1 780 492 9753. E-mail address: [email protected] exciting new therapy is the optimization of cardiac energy metabolism. In the setting of ischaemic heart disease, the general premise for the optimization of cardiac energy metabolism is to either stimulate the oxidation of glucose or inhibit the oxidation of fatty acids for energy production.3 As the oxidation of one molecule of glucose consumes less oxygen than that of a fatty acid, this allows the heart to produce energy more efficiently. Furthermore, stimulating glucose oxidation either directly, or secondarily due to an inhibition of fatty acid oxidation, results in improved coupling between glycolysis and glucose oxidation, which decreases proton production and alleviates myocardial acidosis, improving cardiac efficiency.4,5 There are numerous ways to inhibit cardiac fatty acid oxidation, some of which include2 the inhibition of fatty acid transport into the cardiac myocyte,3 the inhibition of fatty acid uptake into the mitochondria,4 and the inhibition of the enzymatic machinery of the b-oxidative pathway itself. Although there are existing agents that target all three of these approaches, this review will focus on the inhibition of mitochondrial fatty acid uptake approach,3 and in particular, the use of agents that increase levels of Published on behalf of the European Society of Cardiology. All rights reserved. & The Author 2008. For permissions please email: [email protected]. 260 malonyl CoA, a potent endogenous inhibitor of carnitine palmitoyltransferase I (CPT-I), the rate-limiting enzyme in the mitochondrial uptake of fatty acids.6 We will review the literature on the regulation of malonyl CoA via both its synthesis and degradation, how the malonyl CoA axis has been manipulated in animal models of ischaemia/ reperfusion (focusing on the most recent studies involving transgenic mice to manipulate malonyl CoA), and the potential for this axis to be manipulated in humans. 2. Cardiac energy metabolism In the normal healthy heart, almost all (.95%) ATP generated in the heart comes from mitochondrial oxidative phosphorylation, with the remainder derived from glycolysis.7 Despite producing more ATP than carbohydrates, fatty acids are not as oxygen-efficient, requiring 10% more oxygen to produce an equivalent amount of ATP.8 This is of particular importance when oxygen becomes a limiting factor for oxidative metabolism, as seen with ischaemic heart disease. In addition, fatty acids directly inhibit the oxidation of carbohydrates through a phenomenon termed the ‘Randle cycle’.9 This uncouples glycolysis from glucose oxidation, which results in an increased proton production that reduces cardiac efficiency during reperfusion following ischaemia10 (see 11,12 for review). As will be discussed, an emerging approach to optimizing cardiac energy metabolism is to keep levels of malonyl CoA high in the heart. This inhibits the mitochondrial uptake of fatty acids, leading to a subsequent inhibition of fatty acid b-oxidation and secondary increase in glucose oxidation, thereby making oxygen utilization and cardiac energy production more efficient, while preventing the production of protons and development of acidosis.10,11 3. Cardiac carbohydrate metabolism The metabolism of glucose can be separated into two major components, glycolysis and glucose oxidation (see 3,8 for review). Glycolysis results in the production of pyruvate and accounts for ,10% of the total ATP produced by the aerobic heart.13 If glycolysis is coupled to glucose oxidation, the pyruvate generated from glycolysis is converted to acetyl-CoA (which is subsequently oxidized in the TCA cycle) by the enzymatic action of the multi-enzyme complex, pyruvate dehydrogenase (PDH). The PDH complex is under tight regulation by an upstream kinase, PDH kinase, which phosphorylates and inhibits its activity.9 This PDH kinase is positively regulated by acetyl CoA and NADH. As mitochondrial acetyl CoA/CoA and NADH/NAD ratios are increased by elevated rates of fatty acid oxidation, it leads to a potent inhibition of PDH and glucose oxidation. This phenomenon was first described by Randle et al.9 in the 1960s and has been termed the ‘Randle cycle’. 4. Cardiac fatty acid metabolism Fatty acids enter the cardiac myocyte by either passive diffusion or protein-mediated transport across the sarcolemma14 (see 3,8 for review). Once transported across the sarcolemma, fatty acids are subsequently activated by esterification to fatty acyl CoA by fatty acyl CoA synthetase. J.R. Ussher and G.D. Lopaschuk This acyl CoA can either be esterified to intracellular lipids or converted to long-chain fatty acyl carnitine by CPT-I.7 Fatty acid b-oxidation occurs predominantly in the mitochondria and to a smaller extent in the peroxisomes.15 For mitochondrial fatty acid b-oxidation to begin, the cytoplasmic long-chain fatty acyl CoA must first be transported into the mitochondrial matrix through a carnitinedependent transport system.8,16 This carnitine transport system involves three enzymes: CPT-I, carnitine acyltranslocase, and CPT-II. Of these three enzymes, CPT-I is rate limiting in regard to mitochondrial fatty acid uptake and is subject to potent inhibition via malonyl CoA, the compound whose regulation will be the major focus of this review.6 Once in the mitochondria, b-oxidation repeatedly cleaves off two carbon acetyl CoA units from fatty acyl CoA, generating NADH and reduced flavine adenine dinucleotide in the process. The b-oxidation process involves four enzymatically catalysed reactions, with the last step regenerating acyl CoA for another round of b-oxidation and releasing acetyl CoA for the citric acid cycle. As mentioned earlier, oxidation of fatty acids increases the acetyl CoA/CoA ratio, which inhibits PDH and glucose oxidation. 5. Regulation of malonyl CoA As mentioned previously, malonyl CoA is a potent endogenous inhibitor of CPT-I, the rate-limiting enzyme in the mitochondrial uptake of fatty acids. Thus, malonyl CoA decreases the uptake of fatty acids into the mitochondria, thereby reducing mitochondrial fatty acid b-oxidation. Because the turnover of malonyl CoA is quite rapid, with a half life of 1.25 min,17 both the production and the degradation of malonyl CoA control its levels, and therefore of fatty acid oxidation rates. The production of malonyl CoA is primarily attributed to the enzymatic activity of acetyl CoA carboxylase (ACC), which catalyses the carboxylation of acetyl CoA to malonyl CoA (Figure 1).18,19 There are two isoforms of ACC in the heart, a and b, with a predominance of ACCb.19 This leads to the suggestion that the malonyl CoA produced by this isoform is more involved in the regulation of fatty acid oxidation, as opposed to the high abundance of ACCa in the liver, where the malonyl CoA produced by this isoform is more involved in the regulation of fatty acid synthesis. Studies from our laboratory have confirmed the key role of ACCb in regulating cardiac fatty acid oxidation.20 The regulation of ACC is under phosphorylation/dephosphorylation control, with 50 AMP-activated protein kinase (AMPK) having a major role in its regulation in the heart (Figure 1).21,22 As will be discussed in the following section, this AMPK regulation of ACC becomes very important during times of energy starvation in the heart, as seen in ischaemia/reperfusion. Until recently, it was much less clear as to what enzymes might be responsible for the degradation of malonyl CoA. One enzyme that has emerged as being important in controlling cardiac malonyl CoA degradation is malonyl CoA decarboxylase (MCD), whose catalytic activity is responsible for the decarboxylation of malonyl CoA back into acetyl CoA (Figure 1).23 Studies in both rat and mouse have demonstrated that MCD is indeed involved in regulating cardiac malonyl CoA levels, and that inhibition of MCD can limit rates of fatty acid oxidation, leading to a secondary increase in glucose oxidation (Figure 2). This decrease in fatty acid Malonyl CoA and ischaemic heart disease 261 Figure 1 The regulation of malonyl CoA in the heart and its alterations during ischaemia/reperfusion. Malonyl CoA is synthesized via acetyl CoA carboxylase, which carboxylates acetyl CoA into malonyl CoA. Malonyl CoA is degraded via malonyl CoA decarboxylase, which decarboxylates malonyl CoA back into acetyl CoA. In addition, acetyl CoA carboxylase is negatively regulated by phosphorylation via 50 AMP-activated protein kinase. Increased production of malonyl CoA inhibits mitochondrial uptake of fatty acids through carnitine palmitoyltransferase I, thereby reducing rates of fatty acid b-oxidation. During ischaemia, decreased ATP production and a subsequent increase in AMP lead to a rapid activation of 50 AMP-activated protein kinase, which phosphorylates and inhibits acetyl CoA carboxylase, resulting in a dramatic drop in malonyl CoA levels. Following aerobic reperfusion of the ischaemic heart, 50 AMP-activated protein kinase activity is sustained, while malonyl CoA decarboxylase activity is maintained. This keeps malonyl CoA levels low, allowing fatty acids to dominate as the main source of oxidative ATP production, at the expense of glucose oxidation, which increases the production of lactate and protons observed during reperfusion. oxidation and increase in glucose oxidation are also associated with an improvement in the functional recovery of the heart during ischaemia/reperfusion injury.12,24–26 In addition, peroxisome proliferators-activated receptor alpha (PPARa), which is a major transcription factor involved in the regulation of fatty acid oxidation, has been shown to regulate the expression of MCD.27,28 Previous work in our laboratory has demonstrated that the high rates of fatty acid oxidation observed during reperfusion are attributed to a dramatic reduction in the levels of 262 J.R. Ussher and G.D. Lopaschuk Figure 2 Targeting of the malonyl CoA axis to improve ischaemia/reperfusion injury. Novel malonyl CoA decarboxylase inhibitors prevent the degradation of malonyl CoA, keeping malonyl CoA levels high during reperfusion, thereby preventing the uptake and subsequent oxidation of fatty acids in the mitochondria. This reduces mitochondrial acetyl CoA/CoA and NADH/NAD ratios, thus alleviating the fatty acid-induced inhibition of pyruvate dehydrogenase via the ‘Randle cycle’. Increased pyruvate dehydrogenase activity increases the oxidation of pyruvate, improving the coupling between glycolysis and glucose oxidation, reducing lactate and proton production. This decrease in proton production alleviates the acidosis seen during reperfusion, allowing ATP in the heart to be used for contractile purposes as opposed to restoring ionic homeostasis, which improves cardiac functional recovery and overall efficiency. malonyl CoA, as opposed to direct alterations in the characteristics of CPT-I.21 In addition, we have shown that this reduction in malonyl CoA levels is associated with a rapid activation of AMPK during ischaemia, which persists into reperfusion, causing the phosphorylation-induced inactivation of ACC (Figure 1).21 It has also been suggested that MCD is a direct target of AMPK, but our laboratory has been unable to reproduce that data.29 In summary, decreased ACC activity via AMPK phosphorylation, coupled with a maintained MCD activity, is a key factor responsible for the rapid decrease in cardiac malonyl CoA levels observed during ischaemia/reperfusion. 263 Malonyl CoA and ischaemic heart disease Cardiac malonyl CoA levels can also increase secondary to an increase in glucose oxidation. Previous work demonstrated that the acetyl CoA produced by PDH was more accessible to carnitine acetyltransferase than that produced from fatty acid b-oxidation.30 Thus, we hypothesized and showed that increased glucose oxidation could increase cytosolic acetyl CoA supply for ACCb, increasing malonyl CoA levels that then inhibit fatty acid b-oxidation.20 It is of interest to note that although malonyl CoA is a potent inhibitor of CPT-I, the majority of malonyl CoA in the heart is inaccessible to CPT-I. The cytosolic concentration of malonyl CoA in the heart is 5 mM, whereas the IC50 of CPT-I inhibition via malonyl CoA is between 50 and 100 nM.20,31 Therefore, if all the malonyl CoA in the heart were accessible to CPT-I, fatty acid oxidation would always be completely inhibited, which of course is not the case. The reason why the majority of malonyl CoA is not accessible to CPT-I is not known, but may have to do with compartmentation of malonyl CoA. Recent evidence supporting this may come from the observation that a large proportion of MCD exists in the peroxisomes.32 In addition, it has been suggested that the majority of malonyl CoA produced in the heart originates from the peroxisomes.33 6. Cardiac energy metabolism during ischaemia/reperfusion Cardiac energy metabolism is drastically altered during ischaemia, starting with an acceleration of glycolysis, in an attempt to provide an anaerobic source of ATP to make up for the reduction in oxidative ATP production. Also of importance is that fatty acids dominate as the substrate for what residual oxidative metabolism remains in the oxygen-deprived ischaemic heart,34 at the expense of glucose oxidation. This results in an uncoupling between glycolysis and glucose oxidation, contributing to the acidosis observed in the ischaemic heart, which reduces cardiac efficiency.4,10 During reperfusion of the ischaemic heart, glycolytic rates remain elevated, while fatty acids dominate as a source for oxidative energy production.10 These high rates of fatty acid metabolism can account for .90% of energy production in the reperfused heart, and this results in a drastic inhibition of glucose oxidation. Thus, similar to ischaemia, reperfusion of the ischaemic heart is accompanied by an increased production of protons that lowers cardiac efficiency. A major focus of this review has been the emphasis that high rates of fatty acid oxidation can cause myocardial acidosis by uncoupling glucose oxidation from glycolysis. Although other studies have suggested that acidosis may protect the heart during reperfusion by reducing contractile force35–38 to preserve the viability of hibernating myocardium, or keeping the mitochondrial permeability transition pore in a closed state,39,40 such matters are beyond the scope of this review. The reason for the excessive use of fatty acids as a source of fuel during and following ischaemia is primarily the result of two factors: (1) plasma levels of fatty acids increase dramatically during and following ischaemia,41–44 and (2) subcellular changes occur in the heart itself, resulting in a decreased control over fatty acid oxidation.21,45 In particular, the levels of malonyl CoA decrease in the heart due to the rapid activation of AMPK during ischaemia, which persists into reperfusion, resulting in the phosphorylation induced inhibition of ACC.11,21,23,45 This leads to the accelerated mitochondrial uptake of fatty acids and subsequent oxidation. 7. Targeting the malonyl CoA axis to treat cardiac ischaemia There are a number of ways to manipulate malonyl CoA in the heart, which include manipulation of the enzymes involved in regulating its production, i.e. AMPK, ACC, and MCD. The following sections will examine each of the latter three enzymes individually as potential treatments for ischaemia/reperfusion in more detail. 7.1 Targeting 50 AMP-activated protein kinase to treat ischaemia/reperfusion Since its initial identification in 1988 by Sim and Hardie,46 AMPK has become a protein, with wide interest among many investigators, due to its ability to increase energy metabolism in times of stress. In regard to the stress of ischaemia/reperfusion injury, many groups have postulated that AMPK activation would be beneficial in this scenario via increasing glucose uptake to provide an anaerobic source of ATP for the energy-starved heart.47–49 However, our group previously showed that AMPK activity can decrease cardiac malonyl CoA and increase fatty acid oxidation in the ischaemic heart.21 We therefore hypothesized that inhibition of AMPK would be beneficial for ischaemia/ reperfusion injury by increasing malonyl CoA levels and reducing fatty acid oxidation rates, thereby alleviating myocardial acidosis. Supporting the former proposal, isolated working heart studies in a transgenic mouse model of a dominant negative (DN) AMPKa2 with nearly a complete loss of myocardial AMPK activity have been shown to recover worse during reperfusion following a low-flow ischaemia.50 Hearts from the transgenic DN-AMPKa2 mice were unable to increase GLUT4 translocation and glucose uptake during the low-flow ischaemia or reperfusion periods, and they had accelerated rates of apoptosis as indicated by increased caspase 3 cleavage and TUNEL staining. However, DN-AMPKa2 transgenic mice had significant contractile dysfunction compared with wild-type mice in the normal setting, which may explain why they did not recover as well during ischaemia/reperfusion. Furthermore, there were no differences in myocardial metabolism between the control and DN-AMPKa2 transgenic mice, which suggests that there may have been no differences in malonyl CoA levels from the hearts of these animals. Another study investigating the beneficial effects of adiponectin during ischaemia/reperfusion injury noted a reduced phosphorylation of AMPK at its threonine 172 residue (which is necessary for AMPK activation) in an adiponectin-deficient mouse model 48 h after a 30 min occlusion of the left anterior descending (LAD) coronary artery.51 The authors demonstrated that inhibition of AMPK prevented the anti-apoptotic effects of adiponectin on cardiac myocytes and fibroblasts subjected to hypoxia/reoxygenation. Nonetheless, the anti-apoptotic effects of AMPK were performed only in culture, and the beneficial effects of adiponectin during reperfusion following LAD occlusion 264 could also be explained via cyclooxygenase II-dependent effects. More recently, a study in an AMPKa2 subunit-deficient mouse model reported that although AMPKa2 deficiency accelerated the appearance of contracture during ischaemia, there was no effect on reperfusion recovery of these hearts, suggesting that inhibition of AMPK is not detrimental in the heart as an earlier study had reported.52 Moreover, the perfusions in this study were glucose-only perfusions, and thus high rates of fatty acid oxidation would not be a problem in ischaemia/reperfusion. It is possible that the beneficial effect of reducing the extremely high rates of fatty acid oxidation during reperfusion may have been masked because of this. The regulation of AMPK by its upstream kinases, the AMPK kinases (AMPKKs), likely plays an important role in activating AMPK during ischaemia/reperfusion. Previous work in our laboratory has shown that although AMPK is activated in the rat heart during reperfusion following ischaemia, myocardial levels of AMP quickly return to normal. Thus, alternative mechanisms of AMPK activation likely exist outside of changes in AMP levels. One possibility is AMPKK, which phosphorylates and activates AMPK. Identified AMPKKs include the tumour-suppressor LKB1, calmodulindependent protein kinase kinase b (CamKKb), and more recently, transforming growth factor-activated kinase-1.22,53,54 Our group55 and others47 have shown that AMPKK is rapidly activated in the ischaemic heart. To date, the only AMPKK that has been extensively studied in the heart is LKB1. We have shown that AMPKK activation during ischemia is not due to LKB1 activation.55 In contrast, a previous study investigating the role of LKB1 on AMPK activation in the heart during ischaemia and anoxia reported that LKB1 was responsible for phosphorylating and activating the AMPKa2 subunit at its threonine 172 residue, but not the AMPKa1 subunit.56 Although hearts from these mice had enlarged atria and reduced weights, echocardiographic assessment revealed no cardiac dysfunction. However, these studies did not examine functional differences during reperfusion, and perfusions were again performed with glucose as the sole substrate. Further studies are therefore required to determine what role LKB1 and the other AMPKKs have on AMPK during ischaemia/reperfusion, malonyl CoA levels, and functional recovery. Another way to inhibit AMPK is via insulin administration. A number of studies have examined the role of glucose– insulin–potassium (GIK) for the treatment of acute myocardial infarction.57–59 We initially hypothesized that insulin would benefit the aerobically reperfused ischaemic heart. This would arise from the inhibition of myocardial AMPK during ischaemia and subsequent reperfusion, thereby reducing rates of fatty acid oxidation and increasing glucose oxidation rates, alleviating myocardial acidosis and improving functional recovery. Unfortunately, the majority of studies examining the beneficial effects of insulin on functional recovery of the heart during reperfusion have performed their perfusions with glucose as the sole substrate. A recent study in our laboratory has demonstrated that fatty acids in the perfusate interfere with insulin’s ability to inhibit AMPK, and although insulin is still able to reduce fatty acid oxidation, a greater stimulation of glycolysis than glucose oxidation actually increases proton production and worsens functional recovery during reperfusion.60 J.R. Ussher and G.D. Lopaschuk Therefore, it is unlikely that any beneficial effects of insulin during reperfusion involve an inhibition of AMPK, and it is possible that our previous results can explain the lack of mortality benefit with GIK for patients undergoing an acute myocardial infarction during the recent CREATEECLA trial.61 In fact, a recent study suggests that GIK may actually increase mortality in the early post-AMI period.62 Owing to the limitations of the first two studies, and the results of the aforementioned third study, we believe that there is insufficient evidence to state that AMPK activation is beneficial during ischaemia/reperfusion injury. What is needed to reconcile these discrepancies is more studies done using in vivo ischaemia/reperfusion models investigating the effect of AMPK on myocardial function, as well as actual measurements of myocardial malonyl CoA in these systems. 7.2 Targeting acetyl CoA carboxylase to treat ischaemia/reperfusion In regard to ACC, there is very little literature investigating its effects on ischaemia/reperfusion, as the majority of literature on ACC modulation has focused on inhibiting ACC in the liver and adipose tissue. It has been postulated that inhibiting ACC in these tissues to decrease malonyl CoA would decrease fatty acid biosynthesis.63–65 Unfortunately, no studies have investigated the effects of ACC inhibition on cardiac function. There are no selective pharmacological inhibitors of ACC available, and they would have to be specific to the b-isoform, which predominates in the heart and is more tightly linked to the regulation of fatty acid oxidation.20 Nonetheless, mice deficient for ACCb are available and have been characterized and show significant increases in fatty acid oxidation.66 It would be of interest to conduct ischaemia/reperfusion studies in these mice, as it is possible that hearts from these mice would have a depressed recovery of cardiac function during ischaemia/reperfusion due to high rates of fatty acid oxidation and subsequent acidosis. 7.3 Targeting malonyl CoA decarboxylase to treat ischaemia/reperfusion Recent studies in our laboratory have shown that MCD is a major regulator of fatty acid oxidation rates in the heart, and that inhibition of this enzyme is a viable target for the treatment of ischaemia/reperfusion injury.25,26 First, using novel inhibitors of MCD, we have shown that inhibition of MCD in an isolated working rat heart perfusion system significantly increases malonyl CoA levels.26 This was associated with a significant decrease in fatty acid oxidation rates and a subsequent increase in glucose oxidation rates. These metabolic effects induced via inhibition of MCD caused a significant reduction in proton production during both the aerobic setting and during low-flow ischaemia. Furthermore, inhibition of MCD resulted in a significant improvement in cardiac functional recovery of aerobically reperfused ischaemic rat hearts. Another study from our laboratory and Stanley’s demonstrated in an in vivo pig model of demand-induced ischaemia that MCD inhibition once again significantly increased malonyl CoA levels and glucose oxidation rates.24,26 Moreover, this was accompanied by a significant reduction in myocardial lactate production and a complete restoration of left ventricular work. Last, a third study from our laboratory 265 Malonyl CoA and ischaemic heart disease investigated the effects of chronic MCD inhibition in a whole-body MCD-deficient mouse model.25 Although hearts from these animals had a significant increase in malonyl CoA levels, isolated aerobic working heart perfusions demonstrated no differences in glucose and fatty acid metabolism compared with control hearts. This may have been attributed to the significant upregulation in the mRNA of a number of different PPARa target transcripts such as CD36 and CPT-I. Nonetheless, when hearts from the MCD-deficient mice were subjected to the stress of ischaemia/reperfusion injury, a significant improvement in the recovery of cardiac power and function was observed. This enhanced recovery was associated with a significant increase in glucose oxidation rates, whereby glucose oxidation became the major source of ATP production in the heart. Thus, hearts from the MCD-deficient mice had improved coupling between glycolysis and glucose oxidation, reduced proton production, and less myocardial acidosis. As mentioned earlier, although the inhibition of fatty acid oxidation in the heart improves function in the setting of ischaemic heart disease, others have postulated that the inhibition of fatty acid oxidation in peripheral tissues, such as the muscle and liver, will exacerbate insulin resistance and type 2 diabetes.67 This is an important point to consider, a significant number of patients with ischaemic heart disease are also obese/type 2 diabetic. From a clinical standpoint, oral delivery of MCD inhibitors for the prophylactic treatment of ischaemic heart disease would be practical. However, this would affect the peripheral tissues such as the muscle, and could cause insulin resistance or worsen the diabetic state. A recent collaboration by our laboratory and that of Muoio and colleagues68 has shown that this is not the case. Obesity and insulin resistance induced by high-fat diet are actually accompanied by increased rates of incomplete fatty acid oxidation as opposed to impaired fatty acid oxidation.68 In fact, we demonstrated that the MCD-deficient mouse was protected from obesity-induced insulin resistance, which was associated with decreased rates of incomplete fatty acid oxidation. Furthermore, potential toxic intramuscular fatty acid metabolites that have been postulated to cause insulin resistance due to impaired fatty acid oxidation, such as long-chain acyl CoAs, actually trended to increase in the MCD KO mice, suggesting that they are not direct mediators of insulin resistance. As mentioned earlier, MCD expression is transcriptionally regulated by PPARa.27,28 Thus, manipulating PPARa offers another approach to regulating malonyl CoA levels and rates of fatty acid oxidation. Indeed, previous work in our laboratory has shown that hearts from mice deficient for PPARa have reduced expression of MCD and increased levels of malonyl CoA.69 These animals subsequently have lower rates of fatty acid oxidation and increased rates of glucose oxidation. Moreover, PPARa-deficient mice have an improved recovery of cardiac power during reperfusion following a global no-flow ischaemia, whereas mice overexpressing PPARa have a worse recovery of cardiac power under identical conditions.70 These results are contrary to reports utilizing acute systemic activation of PPARa with ligands that caused beneficial effects against ischaemia/ reperfusion injury.71,72 The benefit seen with PPARa inhibition could be due to the optimization of cardiac energy metabolism during reperfusion, whereas the benefit seen with PPARa activation could be the result of its antiinflammatory properties.73–75 Because PPARa has antiinflammatory properties and regulates the expression of many genes involved in fatty acid uptake and oxidation besides MCD,73,76,77 inhibiting MCD to decrease fatty acid oxidation in the heart may be a more plausible approach than inhibiting PPARa. 8. The potential for malonyl CoA axis manipulation in humans Currently, there are a number of agents used clinically that optimize cardiac energy metabolism. This includes, trimetazidine, a 3-ketoacyl CoA thiolase inhibitor. The Cochrane collaboration meta-analysis recently showed trimetazidine to be an effective therapy for stable angina compared with placebo (40% reduction in the mean number of angina attacks per week), alone or combined with conventional antianginal agents.78 In addition, perhexiline, a CPT-1 inhibitor, has been shown to have clinical utility in refractory angina pectoris,79 aortic stenosis,80 and chronic heart failure,81 where it improves symptomatic status, left ventricular ejection fraction, and quality of life. Direct stimulation of glucose oxidation with dichloroacetate, a PDH kinase inhibitor, improves left ventricular stroke volume and cardiac efficiency in the setting of heart failure.82 To date, there are no agents clinically available for the treatment of ischaemia/reperfusion injury that target the malonyl CoA axis to optimize cardiac energy metabolism. On the basis of the positive human trials with trimetazidine, a direct fatty acid b-oxidation inhibitor, and the positive results seen with both acute and chronic MCD inhibition in animals, manipulating the malonyl CoA axis in humans appears plausible and could yield positive effects for the treatment of ischaemia/reperfusion injury. In regard to MCD inhibition, two potential setbacks are that CPT-1 inhibition has been shown in past studies to cause hypertrophy, and that MCD deficiency in humans is associated with cardiomyopathy.83 A number of studies in the early 1980s reported that chronic treatment in dogs and rats with the CPT-1 inhibitor, oxfenicine, results in the development of cardiac hypertrophy.84,85 However, more recent studies have actually shown that the CPT-1 inhibitors, oxfenicine and etomoxir, can actually delay adverse left ventricular modelling in a dog model of pacing-induced heart failure86 and rat model of aortic constriction.87 Some of the reported discrepancy may lie in the fact that the earlier studies did not address whether physiological or pathological hypertrophy was occurring. Furthermore, these inhibitors of CPT-1 were irreversible, whereas manipulating malonyl CoA via MCD would be an indirect inhibition of CPT-1. In addition, MCD-deficient mice have normal cardiac function and show no signs of cardiac hypertrophy.26 To address the cardiomyopathy issue, only 18 patients with MCD deficiency have been reported in the literature,88 and of these 18, only five developed a cardiomyopathy.83,88–92 Of further interest, in those patients who completely lack MCD, no cardiomyopathies were observed, and those patients deficient in MCD that developed cardiomyopathies often possessed mutations in the gene that result in subcellular mistargeting and not the complete absence of MCD protein.92 Therefore, 266 inhibition of MCD in the heart appears to be safe, and future studies are warranted to explore the role of MCD inhibition as a therapy for ischaemic heart disease. As of yet, there are no studies looking at regulating the malonyl CoA axis via ACC in the heart to warrant manipulation of this enzyme in human studies of ischaemia/reperfusion. Moreover, animal studies of AMPK manipulation have yet to investigate the effects of AMPK on malonyl CoA levels in the heart, and results of AMPK’s effects on cardiac function are mixed. Thus, further work in animal models is necessary before AMPK manipulation is used as a therapeutic target in humans for ischaemia/reperfusion injury. 9. Summary The optimization of cardiac energy metabolism represents an exciting new therapeutic approach for the treatment of ischaemia/reperfusion injury. One approach to optimize cardiac energy metabolism is to regulate the levels of malonyl CoA, a potent endogenous inhibitor of cardiac fatty acid oxidation, secondary to its inhibition of CPT-1, the rate-limiting enzyme in the mitochondrial uptake of fatty acids. A number of studies have recently been published showing that the inhibition of MCD increases cardiac malonyl CoA levels. These studies reported improved functional recovery of the heart during ischaemia/reperfusion injury, which was attributed to increased glucose oxidation and decreased proton production. Thus, targeting the malonyl CoA axis in the heart represents a potential exciting new therapy for the treatment of ischaemic heart disease. Conflict of interest: J.R.U. is a trainee of the Alberta Heritage Foundation for Medical Research and Tomorrow’s Research Cardiovascular Health Professionals (TORCH). G.D.L. is a medical scientist of the Alberta Heritage Foundation for Medical Research. J.R.U. has no conflicts to declare. G.D.L. is the President and CEO of Metabolic Modulators Research Ltd, a company which has interests in developing metabolic drugs to treat heart disease. This includes agents that modify the malonyl CoA axis. Funding Supported by a grant from the Canadian Institutes for Health Research Grant to G.D.L. References 1. NHLBI Morbidity and Mortality Chart-book. Bethesda, MD: National Heart, Lung, and Blood Institute; 2004. http://www.nhlbi.nih.gov/ resources/docs/cht-book.htm (23 August 2007). 2. Cooper R, Cutler J, Desvigne-Nickens P, Fortmann SP, Friedman L, Havlik R et al. Trends and disparities in coronary heart disease, stroke, and other cardiovascular diseases in the United States: findings of the national conference on cardiovascular disease prevention. Circulation 2000;102:3137–3147. 3. Ussher JR, Lopaschuk GD. Clinical implications of energetic problems in cardiovascular disease. Heart Metab 2006;32:9–17. 4. Liu Q, Docherty JC, Rendell JC, Clanachan AS, Lopaschuk GD. High levels of fatty acids delay the recovery of intracellular pH and cardiac efficiency in post-ischemic hearts by inhibiting glucose oxidation. J Am Coll Cardiol 2002;39:718–725. 5. Folmes CD, Clanachan AS, Lopaschuk GD. Fatty acid oxidation inhibitors in the management of chronic complications of atherosclerosis. Curr Atheroscler Rep 2005;7:63–70. J.R. Ussher and G.D. Lopaschuk 6. Folmes CD, Lopaschuk GD. Role of malonyl-CoA in heart disease and the hypothalamic control of obesity. Cardiovasc Res 2007;73:278–287. 7. Lopaschuk GD, Belke DD, Gamble J, Itoi T, Schonekess BO. Regulation of fatty acid oxidation in the mammalian heart in health and disease. Biochim Biophys Acta 1994;1213:263–276. 8. Stanley WC, Recchia FA, Lopaschuk GD. Myocardial substrate metabolism in the normal and failing heart. Physiol Rev 2005;85:1093–1129. 9. Randle PJ, Garland PB, Hales CN, Newsholme EA. The glucose fatty-acid cycle. Its role in insulin sensitivity and the metabolic disturbances of diabetes mellitus. Lancet 1963;1:785–789. 10. Liu B, Clanachan AS, Schulz R, Lopaschuk GD. Cardiac efficiency is improved after ischemia by altering both the source and fate of protons. Circ Res 1996;79:940–948. 11. Dyck JR, Lopaschuk GD. Malonyl CoA control of fatty acid oxidation in the ischemic heart. J Mol Cell Cardiol 2002;34:1099–1109. 12. Cuthbert KD, Dyck JR. Malonyl-CoA decarboxylase is a major regulator of myocardial fatty acid oxidation. Curr Hypertens Rep 2005;7:407–411. 13. Neely JM, Morgan HE. Relationship between carbohydrate metabolism and energy balance of heart muscle. Annu Rev Physiol 1974;36:413–459. 14. van der Vusse GJ, van Bilsen M, Glatz JF. Cardiac fatty acid uptake and transport in health and disease. Cardiovasc Res 2000;45:279–293. 15. Kunau WH, Dommes V, Schulz H. Beta-oxidation of fatty acids in mitochondria, peroxisomes, and bacteria: a century of continued progress. Prog Lipid Res 1995;34:267–342. 16. Schulz H. Regulation of fatty acid oxidation in heart. J Nutr 1994;124: 165–171. 17. Reszko AE, Kasumov T, Comte B, Pierce BA, David F, Bederman IR et al. Assay of the concentration and 13C-isotopic enrichment of malonylcoenzyme A by gas chromatography-mass spectrometry. Anal Biochem 2001;298:69–75. 18. Bianchi A, Evans JL, Iverson AJ, Nordlund AC, Watts TD, Witters LA. Identification of an isozymic form of acetyl-CoA carboxylase. J Biol Chem 1990;265:1502–1509. 19. Thampy KG. Formation of malonyl coenzyme A in rat heart. Identification and purification of an isozyme of A carboxylase from rat heart. J Biol Chem 1989;264:17631–17634. 20. Saddik M, Gamble J, Witters LA, Lopaschuk GD. Acetyl-CoA carboxylase regulation of fatty acid oxidation in the heart. J Biol Chem 1993;268: 25836–25845. 21. Kudo N, Barr AJ, Barr RL, Desai S, Lopaschuk GD. High rates of fatty acid oxidation during reperfusion of ischemic hearts are associated with a decrease in malonyl-CoA levels due to an increase in 50 -AMP-activated protein kinase inhibition of acetyl-CoA carboxylase. J Biol Chem 1995; 270:17513–17520. 22. Dyck JR, Lopaschuk GD. AMPK alterations in cardiac physiology and pathology: enemy or ally? J Physiol 2006;574:95–112. 23. Dyck JR, Barr AJ, Barr RL, Kolattukudy PE, Lopaschuk GD. Characterization of cardiac malonyl-CoA decarboxylase and its putative role in regulating fatty acid oxidation. Am J Physiol 1998;275:H2122–H2129. 24. Stanley WC, Morgan EE, Huang H, McElfresh TA, Sterk JP, Okere IC et al. Malonyl-CoA decarboxylase inhibition suppresses fatty acid oxidation and reduces lactate production during demand-induced ischemia. Am J Physiol Heart Circ Physiol 2005;289:H2304–H2309. 25. Dyck JR, Hopkins TA, Bonnet S, Michelakis ED, Young ME, Watanabe M et al. Absence of malonyl coenzyme A decarboxylase in mice increases cardiac glucose oxidation and protects the heart from ischemic injury. Circulation 2006;114:1721–1728. 26. Dyck JR, Cheng JF, Stanley WC, Barr R, Chandler MP, Brown S et al. Malonyl coenzyme a decarboxylase inhibition protects the ischemic heart by inhibiting fatty acid oxidation and stimulating glucose oxidation. Circ Res 2004;94:e78–e84. 27. Lee GY, Kim NH, Zhao ZS, Cha BS, Kim YS. Peroxisomal-proliferatoractivated receptor alpha activates transcription of the rat hepatic malonyl-CoA decarboxylase gene: a key regulation of malonyl-CoA level. Biochem J 2004;378:983–990. 28. Young ME, Goodwin GW, Ying J, Guthrie P, Wilson CR, Laws FA et al. Regulation of cardiac and skeletal muscle malonyl-CoA decarboxylase by fatty acids. Am J Physiol Endocrinol Metab 2001;280:E471–E479. 29. Saha AK, Schwarsin AJ, Roduit R, Masse F, Kaushik V, Tornheim K et al. Activation of malonyl-CoA decarboxylase in rat skeletal muscle by contraction and the AMP-activated protein kinase activator 5-aminoimidazole-4-carboxamide-1-beta-D-ribofuranoside. J Biol Chem 2000;275:24279–24283. 30. Lysiak W, Toth PP, Suelter CH, Bieber LL. Quantitation of the efflux of acylcarnitines from rat heart, brain, and liver mitochondria. J Biol Chem 1986;261:13698–13703. Malonyl CoA and ischaemic heart disease 31. McGarry JD, Mills SE, Long CS, Foster DW. Observations on the affinity for carnitine, and malonyl-CoA sensitivity, of carnitine palmitoyltransferase I in animal and human tissues. Demonstration of the presence of malonylCoA in non-hepatic tissues of the rat. Biochem J 1983;214:21–28. 32. Sacksteder KA, Morrell JC, Wanders RJ, Matalon R, Gould SJ. MCD encodes peroxisomal and cytoplasmic forms of malonyl-CoA decarboxylase and is mutated in malonyl-CoA decarboxylase deficiency. J Biol Chem 1999;274:24461–24468. 33. Reszko AE, Kasumov T, David F, Jobbins KA, Thomas KR, Hoppel CL et al. Peroxisomal fatty acid oxidation is a substantial source of the acetyl moiety of malonyl-CoA in rat heart. J Biol Chem 2004;279:19574–19579. 34. Whitmer JT, Idell-Wenger JA, Rovetto MJ, Neely JR. Control of fatty acid metabolism in ischemic and hypoxic hearts. J Biol Chem 1978;253: 4305–4309. 35. Lorkovic H. Influence of changes in pH on the mechanical activity of cardiac muscle. Circ Res 1966;19:711–720. 36. Pannier JL, Leusen I. Contraction characteristics of papillary muscle during changes in acid–base composition of the bathing-fluid. Arch Int Physiol Biochim 1968;76:624–634. 37. Poole-Wilson PA, Langer GA. Effect of pH on ionic exchange and function in rat and rabbit myocardium. Am J Physiol 1975;229:570–581. 38. Solaro RJ, Lee JA, Kentish JC, Allen DG. Effects of acidosis on ventricular muscle from adult and neonatal rats. Circ Res 1988;63:779–787. 39. Halestrap AP, Clarke SJ, Javadov SA. Mitochondrial permeability transition pore opening during myocardial reperfusion—a target for cardioprotection. Cardiovasc Res 2004;61:372–385. 40. Lemasters JJ, Nieminen AL, Qian T, Trost LC, Elmore SP, Nishimura Y et al. The mitochondrial permeability transition in cell death: a common mechanism in necrosis, apoptosis and autophagy. Biochim Biophys Acta 1998; 1366:177–196. 41. Wisneski JA, Gertz EW, Neese RA, Mayr M. Myocardial metabolism of free fatty acids. Studies with 14C-labeled substrates in humans. J Clin Invest 1987;79:359–366. 42. Lopaschuk GD, Collins-Nakai R, Olley PM, Montague TJ, McNeil G, Gayle M et al. Plasma fatty acid levels in infants and adults after myocardial ischemia. Am Heart J 1994;128:61–67. 43. Kurien VA, Oliver MF. Free fatty acids during acute myocardial infarction. Prog Cardiovasc Dis 1971;13:361–373. 44. Mueller HS, Ayres SM. Metabolic response of the heart in acute myocardial infarction in man. Am J Cardiol 1978;42:363–371. 45. Kudo N, Gillespie JG, Kung L, Witters LA, Schulz R, Clanachan AS et al. Characterization of 50 AMP-activated protein kinase activity in the heart and its role in inhibiting acetyl-CoA carboxylase during reperfusion following ischemia. Biochim Biophys Acta 1996;1301:67–75. 46. Sim AT, Hardie DG. The low activity of acetyl-CoA carboxylase in basal and glucagon-stimulated hepatocytes is due to phosphorylation by the AMP-activated protein kinase and not cyclic AMP-dependent protein kinase. FEBS Lett 1988;233:294–298. 47. Baron SJ, Li J, Russell RR III, Neumann D, Miller EJ, Tuerk R et al. Dual mechanisms regulating AMPK kinase action in the ischemic heart. Circ Res 2005;96:337–345. 48. Beauloye C, Marsin AS, Bertrand L, Krause U, Hardie DG, Vanoverschelde JL et al. Insulin antagonizes AMP-activated protein kinase activation by ischemia or anoxia in rat hearts, without affecting total adenine nucleotides. FEBS Lett 2001;505:348–352. 49. Russell R III. Stress signaling in the heart by AMP-activated protein kinase. Curr Hypertens Rep 2006;8:446–450. 50. Russell RR III, Li J, Coven DL, Pypaert M, Zechner C, Palmeri M et al. AMP-activated protein kinase mediates ischemic glucose uptake and prevents postischemic cardiac dysfunction, apoptosis, and injury. J Clin Invest 2004;114:495–503. 51. Shibata R, Sato K, Pimentel DR, Takemura Y, Kihara S, Ohashi K et al. Adiponectin protects against myocardial ischemia–reperfusion injury through AMPK- and COX-2-dependent mechanisms. Nat Med 2005;11: 1096–1103. 52. Zarrinpashneh E, Carjaval K, Beauloye C, Ginion A, Mateo P, Pouleur AC et al. Role of the alpha2-isoform of AMP-activated protein kinase in the metabolic response of the heart to no-flow ischemia. Am J Physiol Heart Circ Physiol 2006;291:H2875–H2883. 53. Momcilovic M, Hong SP, Carlson M. Mammalian TAK1 activates Snf1 protein kinase in yeast and phosphorylates AMP-activated protein kinase in vitro. J Biol Chem 2006;281:25336–25343. 54. Xie M, Zhang D, Dyck JR, Li Y, Zhang H, Morishima M et al. A pivotal role for endogenous TGF-beta-activated kinase-1 in the LKB1/AMP-activated protein kinase energy-sensor pathway. Proc Natl Acad Sci USA 2006; 103:17378–17383. 267 55. Altarejos JY, Taniguchi M, Clanachan AS, Lopaschuk GD. Myocardial ischemia differentially regulates LKB1 and an alternate 50 -AMP-activated protein kinase kinase. J Biol Chem 2005;280:183–190. 56. Sakamoto K, Zarrinpashneh E, Budas GR, Pouleur AC, Dutta A, Prescott AR et al. Deficiency of LKB1 in heart prevents ischemia-mediated activation of AMPKalpha2 but not AMPKalpha1. Am J Physiol Endocrinol Metab 2006; 290:E780–E788. 57. Fath-Ordoubadi F, Beatt KJ. Glucose–insulin–potassium therapy for treatment of acute myocardial infarction: an overview of randomized placebo-controlled trials. Circulation 1997;96:1152–1156. 58. Timmer JR, van der Horst IC, Ottervanger JP, De Luca G, van’t Hof AW, Bilo HJ et al. Glucose–insulin–potassium infusion as adjunctive therapy in myocardial infarction: current evidence and potential mechanisms. Ital Heart J 2004;5:727–731. 59. Yusuf S, Mehta SR, Diaz R, Paolasso E, Pais P, Xavier D et al. Challenges in the conduct of large simple trials of important generic questions in resource-poor settings: the CREATE and ECLA trial program evaluating GIK (glucose, insulin and potassium) and low-molecular-weight heparin in acute myocardial infarction. Am Heart J 2004;148:1068–1078. 60. Folmes CD, Clanachan AS, Lopaschuk GD. Fatty acids attenuate insulin regulation of 50 -AMP-activated protein kinase and insulin cardioprotection after ischemia. Circ Res 2006;99:61–68. 61. Mehta SR, Yusuf S, Diaz R, Zhu J, Pais P, Xavier D et al. Effect of glucose– insulin–potassium infusion on mortality in patients with acute ST-segment elevation myocardial infarction: the CREATE-ECLA randomized controlled trial. JAMA 2005;293:437–446. 62. Diaz R, Goyal A, Mehta SR, Afzal R, Xavier D, Pais P et al. Glucose– insulin–potassium therapy in patients with ST-segment elevation myocardial infarction. JAMA 2007;298:2399–2405. 63. Choi CS, Savage DB, Abu-Elheiga L, Liu ZX, Kim S, Kulkarni A et al. Continuous fat oxidation in acetyl-CoA carboxylase 2 knockout mice increases total energy expenditure, reduces fat mass, and improves insulin sensitivity. Proc Natl Acad Sci USA 2007;104:16480–16485. 64. Mao J, DeMayo FJ, Li H, Abu-Elheiga L, Gu Z, Shaikenov TE et al. Liverspecific deletion of acetyl-CoA carboxylase 1 reduces hepatic triglyceride accumulation without affecting glucose homeostasis. Proc Natl Acad Sci USA 2006;103:8552–8557. 65. Oh W, Abu-Elheiga L, Kordari P, Gu Z, Shaikenov T, Chirala SS et al. Glucose and fat metabolism in adipose tissue of acetyl-CoA carboxylase 2 knockout mice. Proc Natl Acad Sci USA 2005;102:1384–1389. 66. Abu-Elheiga L, Matzuk MM, Abo-Hashema KA, Wakil SJ. Continuous fatty acid oxidation and reduced fat storage in mice lacking acetyl-CoA carboxylase 2. Science 2001;291:2613–2616. 67. Zhang D, Liu ZX, Choi CS, Tian L, Kibbey R, Dong J et al. Mitochondrial dysfunction due to long-chain acyl-CoA dehydrogenase deficiency causes hepatic steatosis and hepatic insulin resistance. Proc Natl Acad Sci USA 2007;104:17075–17080. 68. Koves TR, Ussher JR, Noland RC, Slentz D, Mosedale M, Ilkayeva O et al. Mitochondrial overload and incomplete fatty acid oxidation contribute to skeletal muscle insulin resistance. Cell Metab 2008;7:45–56. 69. Campbell FM, Kozak R, Wagner A, Altarejos JY, Dyck JR, Belke DD et al. A role for peroxisome proliferator-activated receptor alpha (PPARalpha) in the control of cardiac malonyl-CoA levels: reduced fatty acid oxidation rates and increased glucose oxidation rates in the hearts of mice lacking PPARalpha are associated with higher concentrations of malonylCoA and reduced expression of malonyl-CoA decarboxylase. J Biol Chem 2002;277:4098–4103. 70. Sambandam N, Morabito D, Wagg C, Finck BN, Kelly DP, Lopaschuk GD. Chronic activation of PPARalpha is detrimental to cardiac recovery after ischemia. Am J Physiol Heart Circ Physiol 2006;290:H87–H95. 71. Khandoudi N, Delerive P, Berrebi-Bertrand I, Buckingham RE, Staels B, Bril A. Rosiglitazone, a peroxisome proliferator-activated receptorgamma, inhibits the Jun NH(2)-terminal kinase/activating protein 1 pathway and protects the heart from ischemia/reperfusion injury. Diabetes 2002;51:1507–1514. 72. Yue TL, Bao W, Jucker BM, Gu JL, Romanic AM, Brown PJ et al. Activation of peroxisome proliferator-activated receptor-alpha protects the heart from ischemia/reperfusion injury. Circulation 2003;108:2393–2399. 73. Han SH, Quon MJ, Koh KK. Beneficial vascular and metabolic effects of peroxisome proliferator-activated receptor-alpha activators. Hypertension 2005;46:1086–1092. 74. Yamauchi T, Nio Y, Maki T, Kobayashi M, Takazawa T, Iwabu M et al. Targeted disruption of AdipoR1 and AdipoR2 causes abrogation of adiponectin binding and metabolic actions. Nat Med 2007;13:332–339. 268 75. Marx N, Duez H, Fruchart JC, Staels B. Peroxisome proliferator-activated receptors and atherogenesis: regulators of gene expression in vascular cells. Circ Res 2004;94:1168–1178. 76. Jay MA, Ren J. Peroxisome proliferator-activated receptor (PPAR) in metabolic syndrome and type 2 diabetes mellitus. Curr Diabetes Rev 2007;3:33–39. 77. Sugden MC, Holness MJ. Potential role of peroxisome proliferatoractivated receptor-alpha in the modulation of glucose-stimulated insulin secretion. Diabetes 2004;53(Suppl. 1):S71–S81. 78. Ciapponi A, Pizarro R, Harrison J. Trimetazidine for stable angina. Cochrane Database Syst Rev 2005; CD003614. 79. Cole PL, Beamer AD, McGowan N, Cantillon CO, Benfell K, Kelly RA et al. Efficacy and safety of perhexiline maleate in refractory angina. A doubleblind placebo-controlled clinical trial of a novel antianginal agent. Circulation 1990;81:1260–1270. 80. Unger SA, Robinson MA, Horowitz JD. Perhexiline improves symptomatic status in elderly patients with severe aortic stenosis. Aust N Z J Med 1997;27:24–28. 81. Lee L, Campbell R, Scheuermann-Freestone M, Taylor R, Gunaruwan P, Williams L et al. Metabolic modulation with perhexiline in chronic heart failure: a randomized, controlled trial of short-term use of a novel treatment. Circulation 2005;112:3280–3288. 82. Wargovich TJ, MacDonald RG, Hill JA, Feldman RL, Stacpoole PW, Pepine CJ. Myocardial metabolic and hemodynamic effects of dichloroacetate in coronary artery disease. Am J Cardiol 1988;61:65–70. 83. Yano S, Sweetman L, Thorburn DR, Mofidi S, Williams JC. A new case of malonyl coenzyme A decarboxylase deficiency presenting with cardiomyopathy. Eur J Pediatr 1997;156:382–383. J.R. Ussher and G.D. Lopaschuk 84. Greaves P, Martin J, Michel MC, Mompon P. Cardiac hypertrophy in the dog and rat induced by oxfenicine, an agent which modifies muscle metabolism. Arch Toxicol Suppl 1984;7:488–493. 85. Higgins AJ, Faccini JM, Greaves P. Coronary hyperemia and cardiac hypertrophy following inhibition of fatty acid oxidation. Evidence of a regulatory role for cytosolic phosphorylation potential. Adv Myocardiol 1985;6: 329–338. 86. Lionetti V, Linke A, Chandler MP, Young ME, Penn MS, Gupte S et al. Carnitine palmitoyl transferase-I inhibition prevents ventricular remodeling and delays decompensation in pacing-induced heart failure. Cardiovasc Res 2005;66:454–461. 87. Turcani M, Rupp H. Modification of left ventricular hypertrophy by chronic etomixir treatment. Br J Pharmacol 1999;126:501–507. 88. de Wit MC, de Coo IF, Verbeek E, Schot R, Schoonderwoerd GC, Duran M et al. Brain abnormalities in a case of malonyl-CoA decarboxylase deficiency. Mol Genet Metab 2006;87:102–106. 89. Ficicioglu C, Chrisant MR, Payan I, Chace DH. Cardiomyopathy and hypotonia in a 5-month-old infant with malonyl-coa decarboxylase deficiency: potential for preclinical diagnosis with expanded newborn screening. Pediatr Cardiol 2005;26:881–883. 90. Gao J, Waber L, Bennett MJ, Gibson KM, Cohen JC. Cloning and mutational analysis of human malonyl-coenzyme A decarboxylase. J Lipid Res 1999;40:178–182. 91. Matalon R, Michaels K, Kaul R, Whitman V, Rodriguez-Novo J, Goodman S et al. Malonic aciduria and cardiomyopathy. J Inherit Metab Dis 1993;16: 571–573. 92. Wightman PJ, Santer R, Ribes A, Dougherty F, McGill N, Thorburn DR et al. MLYCD mutation analysis: evidence for protein mistargeting as a cause of MLYCD deficiency. Hum Mutat 2003;22:288–300.