Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Heritability of autism wikipedia , lookup
Gene therapy wikipedia , lookup
History of genetic engineering wikipedia , lookup
Fetal origins hypothesis wikipedia , lookup
Biology and consumer behaviour wikipedia , lookup
Genetic engineering wikipedia , lookup
Population genetics wikipedia , lookup
Genetic testing wikipedia , lookup
Pharmacogenomics wikipedia , lookup
Neuronal ceroid lipofuscinosis wikipedia , lookup
Epigenetics of diabetes Type 2 wikipedia , lookup
Epigenetics of neurodegenerative diseases wikipedia , lookup
Human genetic variation wikipedia , lookup
Microevolution wikipedia , lookup
Designer baby wikipedia , lookup
Behavioural genetics wikipedia , lookup
Medical genetics wikipedia , lookup
Quantitative trait locus wikipedia , lookup
Genome (book) wikipedia , lookup
Heritability of IQ wikipedia , lookup
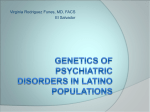
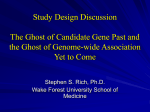
ME62CH02-Hirschhorn ARI ANNUAL REVIEWS 4 December 2010 Further Annu. Rev. Med. 2011.62:11-24. Downloaded from www.annualreviews.org by University of Oxford - Bodleian Library on 05/27/11. For personal use only. Click here for quick links to Annual Reviews content online, including: • Other articles in this volume • Top cited articles • Top downloaded articles • Our comprehensive search 11:3 Genome-Wide Association Studies: Results from the First Few Years and Potential Implications for Clinical Medicine Joel N. Hirschhorn and Zofia K. Z. Gajdos Department of Genetics, Harvard Medical School, Boston, Massachusetts 02115; Program in Genomics and Divisions of Genetics and Endocrinology, Children’s Hospital, Boston, Massachusetts 02115; Broad Institute, Cambridge, Massachusetts 02142; email: [email protected], zofi[email protected] Annu. Rev. Med. 2011. 62:11–24 The Annual Review of Medicine is online at med.annualreviews.org This article’s doi: 10.1146/annurev.med.091708.162036 c 2011 by Annual Reviews. Copyright All rights reserved 0066-4219/11/0218-0011$20.00 Keywords human genetics, common disease, quantitative traits, personalized medicine, biological pathways, common variants Abstract Most common diseases and quantitative traits are heritable: determined in part by genetic variation within the population. The inheritance is typically polygenic in that combined effects of variants in numerous genes, plus nongenetic factors, determine outcome. The genes influencing common disease and quantitative traits remained largely unknown until the implementation in 2006 of genome-wide association (GWA) studies that comprehensively surveyed common genetic variation (frequency >5%). By 2010, GWA studies identified >1,000 genetic variants for polygenic traits. Typically, these variants together account for a modest fraction (10%–30%) of heritability, but they have highlighted genes in both known and new biological pathways and genes of unknown function. This initial effort prefigures new studies aimed at rarer variation and decades of functional work to decipher newly glimpsed biology. The greatest impact of GWA studies may not be in predictive medicine but rather in the development over the next decades of therapies based on novel biological insights. 11 ME62CH02-Hirschhorn ARI 4 December 2010 11:3 DISEASE GENETICS: SINGLE-GENE DISORDERS AND POLYGENIC DISEASES Annu. Rev. Med. 2011.62:11-24. Downloaded from www.annualreviews.org by University of Oxford - Bodleian Library on 05/27/11. For personal use only. Most diseases have an inherited component to susceptibility, meaning that genetic variation influences disease risk. The influence of genetics is clearest for Mendelian, single-gene disorders, where mutations in a particular gene are necessary and sufficient to cause the disease. The transmission of these mutations from parents to children typically results in clearly recognizable familial patterns of inheritance, because the penetrance of disease-causing mutations (the probability of being affected with disease) is usually quite high, even though clinical presentation and severity can vary. These highly penetrant mutations are usually evolutionarily deleterious and hence quite rare, and many—but not all—are coding changes that significantly disrupt or alter the protein encoded by the disease gene. Because of these characteristics, genetic linkage analysis with follow-up sequencing, which is particularly well suited to finding highly penetrant mutations with clear functional consequences, was highly successful for mapping and identifying many Mendelian disease genes (1, 2). Most common diseases (for example, cancer, coronary heart disease, diabetes, and hypertension) and even quantitative traits (such as height, weight, blood pressure, and blood chemistries) also have an inherited component. For most common diseases, heritability—the fraction of variation in risk in a population that is attributable to inherited factors—typically ranges from 30% to well over 50% (for example, see 3–5). For quantitative traits, heritability estimates are often above 50% and can approach 80%–90% (6–8). These diseases and traits are polygenic, meaning that variation in many genes typically combine to influence phenotype (as do nongenetic factors such as environmental exposures). Because no single gene carries mutations that are sufficient to determine the outcome, families do not display clearly recognizable patterns of inheritance. 12 Hirschhorn · Gajdos Given the success of linkage analysis in Mendelian disorders, it was natural to attempt linkage analysis for polygenic disorders. However, with a few exceptions, large linkage studies were unsuccessful at identifying regions that met stringent statistical thresholds (2). These important negative results suggested that, for most polygenic diseases and quantitative traits, no individual gene contains variants that together account for a substantial fraction of heritability. Because linkage has low power to detect genetic variants with modest effects (9), especially if, as had been hypothesized, they are common in the population (10–13), a different approach was proposed to uncover the genetic basis of common disease: association studies (see sidebar “Comparison of Association and Linkage Analysis”). GENETIC ASSOCIATION STUDIES FOR POLYGENIC DISEASES AND TRAITS The initial association studies were candidate gene studies, in which one or a handful of sequence variants from a single gene were tested for correlation with disease. Associations with human leukocyte antigen (HLA) were among the first that could be readily reproduced, in part because these often turned out to have large effects on disease risk that could be reproducibly demonstrated even in small samples of tens or hundreds of patients. For example, nearly half of the excess risk to siblings of patients with type 1 diabetes is explained by variation at multiple genes within the HLA locus (see 14, 15 and references therein). A few early associations with type 1 diabetes and inflammatory bowel disease (IBD) reflected effect sizes that were large enough to produce signals in linkage analysis (14–16), and perhaps created expectations that many common diseases would have variants with large effect sizes. Although several common variants outside of the HLA locus turned out to have moderate or large effects on diseases and quantitative traits (17–23), most associated common variants have modest Annu. Rev. Med. 2011.62:11-24. Downloaded from www.annualreviews.org by University of Oxford - Bodleian Library on 05/27/11. For personal use only. ME62CH02-Hirschhorn ARI 4 December 2010 11:3 effects that require large association studies for reliable detection (24, 25) and do not produce readily apparent signals even in extremely large linkage studies (2, 9). The modest effect sizes of common variants meant that early association studies, which were limited by logistical considerations to handfuls of variants tested in hundreds of samples, typically did not provide strong evidence of association. Furthermore, nominally significant ( p < 0.05) results were often interpreted as definitive, when in fact much lower p values are required to demonstrate that an association is likely valid (2, 25–27). Thus, false positive and false negative results of association studies were commonplace (24), and and the problem was likely exacerbated by technical artifacts and the presence of multiple genetic ancestries within individual studies (population stratification) (28, 29). Gradually, well-powered and well-controlled studies emerged that employed large samples, methods to detect and correct for population stratification (30), appropriate statistical thresholds, and robust genotyping methods. With these new standards in place, association studies slowly began to yield more reproducible results. With the development of genome-wide association (GWA) studies, a more comprehensive approach became available that could greatly accelerate progress. RESULTS OF THE FIRST WAVES OF GENOME-WIDE ASSOCIATION (GWA) STUDIES The transition from candidate gene association studies to GWA studies required four key technical and scientific advances: the discovery of widespread correlation (linkage disequilibrium) between groups of nearby common variants (31); catalogues of common variants and their correlations (32, 33); the development of highthroughput genotyping methods that could assay hundreds of thousands of genetic markers, typically single-nucleotide polymorphisms (SNPs) (34); and statistical methods to use the correlations between common variants to COMPARISON OF ASSOCIATION AND LINKAGE ANALYSIS Association studies, like linkage studies, are designed to identify regions of the genome that, when inherited, influence phenotype. In a genetic association study of disease, DNA sequence variants are genotyped in affected individuals and in controls (who can be relatives or unrelated individuals of similar genetic ancestry). The frequencies of genotypes (e.g., C/C versus C/T versus T/T) or alleles (C versus T) are compared, and if one genotype or allele is statistically significantly more frequent in cases than in controls, the variant is said to be associated with the disease. Association studies of quantitative traits are identical, except that variants are tested for a correlation between genotype and trait values. The fundamental difference between association and linkage studies is that linkage analysis tests for correlation between a genomic region and phenotype in families, whereas association analysis searches for correlation in the population (essentially treating the population as a single large family with an unknown pedigree). A major consequence of this difference is that association analysis is better suited to finding common genetic variants with more modest effects, whereas linkage analysis is better powered to identify regions that contain variants (common or rare) that in aggregate have a more substantial effect (see 2, 9). Furthermore, because close relatives share stretches of genetic material over a larger distance than do unrelated individuals, association analysis can map disease-causing variants to a smaller region, defined by the extent of correlation between variants in the population (linkage disequilibrium, or LD). Although these regions are smaller, they often contain multiple genes; thus, association studies often can highlight a small region but often cannot pinpoint a causal gene within that region. impute genotypes at additional variants not directly assayed by the genotyping platforms (35, 36). With the dramatic increase in scale from candidate to GWA studies, increasing rigor and sample sizes were essential to avoid a flood of false positive and false negative results. Fortunately, the importance of stringent statistical thresholds, high-quality data, and careful avoidance of artifacts were already becoming widely accepted when GWA studies became feasible. Consequently, most of the results from GWA studies that surpass these stringent thresholds of significance—“genome-wide significance,” www.annualreviews.org • Genome-Wide Association Studies 13 ARI 4 December 2010 11:3 typically a p value threshold of 5 × 10−8 (25, 27)—have been replicable. The first widely replicable result from GWA studies was the association between variation at the complement factor H (CFH) gene and age-related macular degeneration (AMD) (18). This discovery was the earliest of its kind in part because variation at CFH has a large effect—greater than fourfold—on AMD risk. Identification of associated variants for other diseases and traits, where effect sizes are generally much more modest, awaited more robust genotyping methods that could be applied in large samples. The first such studies, published in 2006 and the first half of 2007, typically involved at most a few thousand individuals. Although some of these did not identify any clear associations, most identified one or a few common genetic variants that were associated at genome-wide levels of significance with common diseases such as IBD (26, 37–39), prostate cancer (40, 41), type 2 diabetes (26, 42–46), obesity (47), coronary heart disease (26, 48), breast cancer (49, 50), and type 1 diabetes (26, 51). The GWA studies successfully completed by the end of 2007 are too numerous to list here, but these identified many more novel associations between common variants and polygenic diseases or quantitative traits. These initial discoveries established several themes. First, many of the associated common genetic variants did not alter any predicted proteins, and some were hundreds of kilobases away from the nearest gene, suggesting that variation in the regulation of gene expression— perhaps exerted over long distances—was likely to be important in polygenic diseases and traits. These results largely contrast with those of single-gene disorders: Variants known to underlie single-gene disorders often are in the coding region and severely alter protein function (52). Second, the individual effect sizes of the variants from GWA studies were modest, typically explaining <1% of the population variation in phenotype. Thus, the initial GWA studies did not substantially improve prediction of disease risk (53), again in contrast to the experience from single-gene disorders. Annu. Rev. Med. 2011.62:11-24. Downloaded from www.annualreviews.org by University of Oxford - Bodleian Library on 05/27/11. For personal use only. ME62CH02-Hirschhorn 14 Hirschhorn · Gajdos Third, the GWA results were largely replicable in additional studies (25, 27), demonstrating the utility of combining careful study design with sufficient power to achieve rigorous statistical thresholds, despite recent assertions that many GWA results are artifactual (54). Finally, although some associated variants were in or near known candidate genes, most associations highlighted genomic regions that contained no genes with previously known biological relevance, suggesting that these unbiased, genome-wide genetic studies were providing insights into novel biology (55). This pattern is similar to the experience from single-gene disorders, where the identification of diseasecausing genes often opened up new windows into disease biology (2). With the recognition that modest effect sizes meant that large sample sizes were critical to achieve genome-wide statistical significance, the next two years saw the formation of multiple consortia. Multiple groups with individual GWA studies joined forces to increase sample size through meta-analysis of association results from each component study. These efforts required a different, team-based scientific culture that recognized not only the efforts of key individuals but also the valuable and substantial contributions of large numbers (typically >100) of investigators. The result of these collaborations was an explosion in new associations. More than 1,000 genome-wide significant associations between common genetic variants and polygenic traits and diseases have been cataloged by Manolio’s group at the National Human Genome Research Institute (56; http://www.genome.gov/gwastudies/), and most of these were published in 2009 and 2010. The list of associations is too extensive and too rapidly expanding to capture comprehensively here; instead, we briefly review the status (as of August 2010) of an illustrative group of diseases and quantitative traits: IBD, type 2 diabetes, autism, lipid levels, height, and hemoglobin F concentrations (Table 1). Given the rate of discovery, the numbers of associations will no doubt continue to grow rapidly, 15 Abbreviations: N/A: Not applicable, as precise sites of action of therapies are not known or no therapies are available, or no known Mendelian forms of disease exist. UC: ulcerative colitis; CD: Crohn’s disease. Yes Yes ∼35% 3 Hemoglobin F levels Height www.annualreviews.org • Genome-Wide Association Studies Identification of previously unsuspected key regulator of globin switching, new potential drug targets N/A Additional pathways emerge after identification of >100 loci; direct evidence for role of common variants Yes Many 180 ∼12% Yes Previously unsuspected genes validated as regulating lipid levels, providing new potential drug targets Yes Near complete 95 across 3 traits Lipid levels 1–2 Autism ∼25–30% Yes Rare variants, especially structural variants, more prominent in initial genetic studies No N/A ∼10% 32 Type 2 diabetes No Yes ∼20% >40 Inflammatory bowel disease Low Yes Comments locus? within loci? N/A (August 2010) (August 2010) Disease/trait disorders Multiple variants per Drug targets Overlap with Mendelian Heritability explained Like IBD, type 2 diabetes had been associated with a few common variants prior to GWA studies (see 63 and references therein). Nearly a Number of loci in GWA studies Type 2 Diabetes Characteristics of genome-wide association (GWA) discoveries for several exemplar common diseases and quantitative traits Prior to GWA studies, several common or moderately common variants had been associated with IBD. These were found by association studies that focused on genes within regions highlighted by linkage studies or by large-scale studies of nonsynonymous coding variants (see 16, 57 and references therein). Subsequent GWA studies identified 32 loci associated with Crohn’s disease (CD) and additional loci associated with ulcerative colitis (UC), with partial overlap between the CD- and UC-associated loci (see 16, 57 and references therein, and 58–62). The CD-associated loci account for ∼20% of the heritable portion of disease risk, raising the theoretical possibility of predictive and/or diagnostic genetic testing. However, the greater impact of these studies has been to generate new understanding of the pathogenesis of IBD. The associated loci define several biological pathways as causally involved in pathophysiology, including innate immunity, IL23 signaling/Th17 lymphocytes, autophagy, epithelial barrier integrity, and the secondary immune response (16, 57). Critically, several of these pathways were not appreciated as being involved in the pathogenesis of IBD until the GWA results emerged. Some of these pathways are active areas of research that may accelerate the development of new therapies. The comparison between the UC- and CDassociated loci has defined both common and distinct pathways across these two related diseases (57), and the loci that are uniquely associated with UC or CD might eventually help distinguish these two diseases, which in some patients can be hard to distinguish clinically. Table 1 Annu. Rev. Med. 2011.62:11-24. Downloaded from www.annualreviews.org by University of Oxford - Bodleian Library on 05/27/11. For personal use only. Inflammatory Bowel Disease Yes but the principles illustrated by these examples are likely to remain relevant. Cell cycle only statistically significant pathway, but genes in loci suggest multiple known and novel processes 11:3 Several clear, novel pathways guiding new therapeutic research; variants might aid in distinguishing UC versus CD 4 December 2010 Yes ARI No ME62CH02-Hirschhorn ARI 4 December 2010 11:3 dozen GWA studies identified a total of 32 loci that together account for ∼10% of the heritable portion of disease risk (see 64 and references therein). Although the fraction of variability in disease risk explained by these variants is still low, the variants can add information to known risk factors, particularly earlier in life (65). The variants are also beginning to outline known and novel aspects of disease pathogenesis. Some of the loci highlight known genes, such as those encoding monogenic forms of diabetes (neonatal diabetes, mature-onset diabetes of youth, or Wolfram syndrome), genes involved in insulin signaling (IRS1), or genes encoding the sites of action of antidiabetic medications (KCNJ11, PPARG). Few pathways other than the cell cycle were unamibiguously defined by the genes within associated loci, but some of the genes suggest the involvement of less well-studied biological processes such as circadian rhythms, beta cell zinc transport, and RNA binding proteins. These results suggest that many of the pathways underlying the pathophysiology of type 2 diabetes have yet to be defined or annotated. Examination of the effects of these variants in nondiabetic individuals demonstrated that many associated variants increase diabetes risk through diminished beta cell function, although some clearly affect insulin action. Another interesting finding was that many of the type 2 diabetes loci overlap with loci associated with other diseases or traits. In some cases the associated variants are the same (and have pleiotropic effects), but in many other cases the associated variants differ, suggesting that the variants exert different regulatory effects on genes that play a role in the pathogenesis of multiple diseases (64). Similar overlaps have been seen with variants that influence the risk of different autoimmune diseases (15) or different types of cancer, most notably at several locations tens to hundreds of kilobases upstream of the MYC gene (66). Finally, many of the variants that influence diabetes risk are quite distant from any known genes, raising the possibility of long-range regulation. Indeed, at the MYC cancer-associated locus looping between elements separated by hundreds of kilobases has Annu. Rev. Med. 2011.62:11-24. Downloaded from www.annualreviews.org by University of Oxford - Bodleian Library on 05/27/11. For personal use only. ME62CH02-Hirschhorn 16 Hirschhorn · Gajdos been documented, providing a possible mechanism for regulation over large distances (67). Autism Initial GWA studies of autism did not identify any associated common variants, and only recently have two common variant associations reached (or nearly reached) genome-wide levels of significance (68, 69). By contrast, several studies have shown that rare structural variants (deletions or duplications) or point mutations can have substantial effects on disease risk (70–72). The contrast between autism and most other common diseases suggests that the genetic architecture of autism, and perhaps other neuropsychiatric disorders such as schizophrenia (70, 71), may be somewhat different from that of type 2 diabetes, IBD, and many other common disorders. Lipid Levels Prior to the advent of GWA studies, several genetic associations had already been identified with levels of HDL cholesterol, LDL cholesterol, and triglycerides, including both common and rare variants in known candidate genes (73, 74). GWA studies have since identified nearly 100 genetic loci with common variants that together explain 25%–30% of the population variation in these lipid levels (see 73, 75 and references therein). Almost every gene known to underlie a single-gene disorder of lipid metabolism has also been identified by the GWA studies, not only demonstrating that GWA studies are recapitulating the known biology, but also suggesting that many of the other genes identified by GWA studies will be novel regulators of lipid metabolism and have rare as well as common variants that influence lipid levels. Indeed, of the many genes that are new candidates for playing a role in lipid metabolism, several have recently been validated. By using in vitro and in vivo models, four genes identified in GWA studies, PPP1R3B, SORT1, TTC39B, and GALNT2, have been confirmed as regulating human lipid levels (75, 76). In the case of SORT1, there is Annu. Rev. Med. 2011.62:11-24. Downloaded from www.annualreviews.org by University of Oxford - Bodleian Library on 05/27/11. For personal use only. ME62CH02-Hirschhorn ARI 4 December 2010 11:3 compelling evidence that a particular regulatory variant is responsible for the variation in LDL cholesterol levels (76). Two genes encoding sites of action of lipid-lowering medications were highlighted in the GWA studies, suggesting that some of the other genes with no previously suspected connections to known lipid metabolism pathways may provide suitable new drug targets. The variants discovered by GWA studies of population-based samples have also been examined for their ability to predict clinical disease, and have been shown to explain part of the risk for clinically defined hypertriglyceridemia (77). Furthermore, some of these variants contribute to the risk of myocardial infarction, and, together with other variants that are associated with coronary heart disease, they provide nearly the same discriminatory power for risk of coronary heart disease as do individual traditional clinical risk factors such as blood pressure (78). (We note that when assessing predictive models, it is important that the outcomes being predicted align well with the phenotypes associated with the variants used in the model.) single GWA study, suggested that about half of the heritability of height can be accounted for by additive effects of a large number of common (>5% frequency) variants (81). At least 19 height-associated loci have multiple independently associated common variants, suggesting that many of the as-yet-unidentified variants may lie in already-identified loci. An enrichment of associated common missense variants showed that, at least for some of the associated loci, common variants themselves—rather than collections of rare variants—were responsible for the signals of association. Finally, the studies of height also confirmed that, if enough loci are identified, GWA studies can highlight biological pathways. For height, these include groups of genes involved in chromatin structure, hedgehog signaling, TGF-β signaling, growth hormone/IGF-1 pathways, BMP/noggin signaling, and the extracellular matrix (80). Interestingly, some of these highly relevant pathways emerged only after hundreds of associations were identified, suggesting that very large numbers of loci may have a greater impact on implicating biological processes than on explaining a larger fraction of phenotypic variation. Height Height is the classic polygenic trait (79), is highly heritable (8), and is routinely measured in large populations. Thus, quite large GWA studies of height are feasible and may provide early general insights into the genetic architecture of complex traits. Prior to GWA studies, no common variants were known to be associated with height, but a series of increasingly large GWA studies has now been completed. The most recent involved a first stage of 129,000 individuals and a replication stage of up to ∼50,000 individuals; it identified variants at 180 loci that together explain ∼12% of the heritable variation in height (80). Power considerations suggested that there are several hundred more common variants yet to be discovered that have similar effect sizes on height, and that together these common variants will explain at least ∼2% of heritability. A separate analysis, using data from all the SNPs in a Hemoglobin F Levels During human development, globin gene expression shifts from the fetal form (hemoglobin F, HbF) to the adult form (hemoglobin A), but detectable levels of HbF can still be found in adults due to residual expression of the gamma globin gene. HbF levels are an important modifier of the severity of sickle-cell disease, thalassemia, and other hemoglobinopathies, and are under genetic regulation, partially explained by rare and common cis-acting variation at the globin locus (21). However, despite decades of intensive efforts, the genes responsible for regulating the switch from gamma to beta globin expression were not known. The first GWA studies identified common variants that accounted for >30% of the population variability in HbF levels, including variation at the globin locus and multiple variants at two other loci, near BCL11A and MYB-HBS1L (19, 20, 22). These www.annualreviews.org • Genome-Wide Association Studies 17 ME62CH02-Hirschhorn ARI 4 December 2010 11:3 variants can account for some of the variability in severity of sickle-cell disease or thalassemia (22, 82), but the major impact of these discoveries is likely to be through the new understanding of globin regulation. Specifically, the BCL11A protein was rapidly shown to be a key regulator of globin switching in vitro and in vivo (83, 84). Thus, GWA studies have opened new areas of research that could plausibly lead to new therapies targeting these proteins. Annu. Rev. Med. 2011.62:11-24. Downloaded from www.annualreviews.org by University of Oxford - Bodleian Library on 05/27/11. For personal use only. THE NEXT WAVE OF GENETIC STUDIES OF POLYGENIC TRAITS AND DISEASES The first three years’ worth of GWA studies discovered numerous associated genetic loci for many different polygenic traits and diseases. However, the variants identified thus far generally explain less than half (and in a number of cases less than 5%) of the heritability. Several possible explanations of this “missing heritability” have been proposed (81, 85, 86). These include a role for additional common variants of small effect, a role for less common variants (including variants with frequencies between 0.5% and 5%, which have not been well surveyed by current GWA studies), the presence of even rarer variants (those that are essentially private to each unrelated individual), nonadditive interactions between variants, and epigenetic effects. Regardless, these initial GWA studies, along with the failure of linkage studies to generate reproducible signals, have provided strong evidence that many common diseases and quantitative traits are quite polygenic, and this is likely an important contributor to asyet-unexplained variance. Indeed, despite the large sizes of GWA studies to date, it remains possible that much of the unexplained variance can be accounted for by additional common variants that have not yet been detected. Recent work suggests that common variants of small effect may account for up to half of the heritability of phenotypes such as height and even schizophrenia (80, 81, 87), so further increases in sample size will likely yield new associated variants. Current GWA 18 Hirschhorn · Gajdos studies have largely interrogated variants with frequencies of at least 5%–10% in the population. The next versions of GWA studies could build on data from the 1000 Genomes Project (http://www.1000genomes.org) to identify additional associated variants, as exemplified by a recent candidate gene sequencing study of type 1 diabetes that found associated variants in the 1% frequency range in IFIH1 (88). Advances in sequencing technologies will enable genome-wide sequencing studies to assess more comprehensively the role of rare variation. These will no doubt identify rare variation that influences polygenic traits and diseases, based on early successes of classic candidate gene sequencing studies of obesity, lipid levels, and blood pressure (74, 89–91). However, implementation and interpretation of sequencing studies in polygenic traits and diseases will not be straightforward. First, methods for rigorous analysis, high-quality data generation, careful interpretation, and avoidance of artifact (especially confounding by ancestry) have not been well-established for sequencing studies. Second, in sequencing studies, rare variants must be analyzed in aggregate, and it may be difficult to distinguish rare functional variants from the background of rare neutral variants, particularly for noncoding variation. Finally, the lack of strong linkage signals provides evidence that the contribution of rare variants at any one gene will be modest, so it is likely that large samples will be required, perhaps comparable to those that have been needed for GWA studies (2). IMPACT OF GWA STUDIES ON CLINICAL MEDICINE The identification of genetic loci can have two major impacts on clinical medicine—through prediction of future outcomes or through elucidation of underlying biology (Figure 1). Prediction has the potential for immediate impact, although, as discussed below and by others (53, 92), the clinical utility of predictive genetic tests depends both on the degree of additional prediction provided by the genetic markers and on ME62CH02-Hirschhorn ARI 4 December 2010 11:3 whether the clinical course of action would be altered by predictive information. By contrast, the insights into biology and pathophysiology are likely to develop over a longer time frame. New genetic loci discovered Annu. Rev. Med. 2011.62:11-24. Downloaded from www.annualreviews.org by University of Oxford - Bodleian Library on 05/27/11. For personal use only. Prediction Using Genetics: The Potential for “Personalized Medicine” Much of the immediate focus on the discoveries from GWA studies has been on the feasibility of using genetic testing to predict disease or to guide therapy. One illustration is the rapid appearance of direct-to-consumer genetic testing companies that utilize common variants to provide estimates of relative risk, but not absolute risk (93). However, it is not certain that current or even future collections of associated variants will be clinically useful for prediction. First, the level of prediction thus far is typically modest, although in some cases the discriminative power of common genotypes is comparable to clinical tests that are in widespread use [such as LDL cholesterol for the prediction of myocardial infarction (78)]. More critically, the clinical utility of predictive models depends on their ability to alter clinical management, and this in turn depends on the availability of clinical interventions that are not universally indicated for reasons of safety or cost, but that might on balance be beneficial or cost-effective for higherrisk subgroups of patients (Figure 1). There are many examples of genetics influencing clinical management for Mendelian or near-Mendelian traits and diseases, including diagnosis, prognosis, and reproductive counseling for many single-gene disorders, as well as blood typing prior to transfusion. In a few polygenic cases, particularly those involving drug response, the predictive information is strong and is used to make management decisions; for example, patients are HLA-typed to avoid hypersensitivity reactions to abacavir (94). Other GWA results in the area of pharmacogenetics may lead to similar clinical algorithms that incorporate genetic testing, perhaps with genetically guided interventions to avoid adverse reactions (95). In other cases, predictive power is strong but there are no preventive measures Short time frame Short-to-medium time frame Identification of the relevant variants Identification of the relevant genes Short time frame Prediction models Medium-to-long time frame Understanding of underlying biology Depends on predictive power and available clinical options Clinically useful prediction Long time frame Clinically useful therapies Figure 1 Identification of genetic loci that are associated with human disease can lead in two directions. Left: In the short term, if the predictive value of specific genetic variants (which can be nearby markers of the actual causal variants) is strong enough, and there are clinical interventions whose utility depends on predictive information, genetic information can guide clinical care. The clearest examples come from single-gene disorders and pharmacogenetics, where predictive power is high. However, many clinically useful tests have predictive power similar to that provided by genetic variation for many common diseases, raising the possibility of eventual application of genetic information for prediction. Right: Alternatively, identification of genetic loci and the relevant genes at those loci can lead to a deeper understanding of the underlying biology, which can in turn help guide the development of new interventions and therapies. Even when successful, this process usually takes decades before new therapies are developed, but it may provide the greater long-term impact of human genetic studies. that are not universally indicated, so the associations do not affect clinical management. Examples include type 1 diabetes and AMD. For yet other diseases, the level of prediction may be lower, but might still be sufficient to identify a subgroup of patients who would benefit from an intervention that is either too expensive or too risky to apply to the general population. One possible example is the use of intensive lifestyle management and/or pharmacotherapy in patients who are at high risk of developing type 2 diabetes; although these interventions are effective (96), they are too costly for www.annualreviews.org • Genome-Wide Association Studies 19 ME62CH02-Hirschhorn ARI 4 December 2010 11:3 Annu. Rev. Med. 2011.62:11-24. Downloaded from www.annualreviews.org by University of Oxford - Bodleian Library on 05/27/11. For personal use only. universal adoption, but genetic test results in combination with other known risk factors might eventually identify a high-risk group for whom the interventions would be costeffective. As predictive power continues to improve, clinical trials that test whether it is useful to take genetic factors into consideration could become more informative. Finally, we note that genetic risk scores would most appropriately supplement rather than replace traditional risk estimates, and should be evaluated in this context. Understanding Human Biology and Pathophysiology Looking into the future, the greatest impact of GWA studies (and genetic studies more generally) will likely flow from expanding our understanding of underlying biology in patients. GWA studies of polygenic diseases and traits recapitulate many known biological pathways relevant to those diseases and traits. Furthermore, the delineation of pathways becomes clearer as the number of loci increases, with the picture continuing to sharpen even when the number of loci reaches the hundreds (80), so the continued identification of loci may aid in the identification of new pathways. Even more important, the sites of action of many known therapies have already been highlighted by associated variants (55, 75, 80), suggesting that the other loci may provide clues to new therapies. It is clear that many GWA loci do not contain genes that had previously been suspected as biological candidates. In some cases (as described in this review), these new genes identify well-studied biological pathways that were not previously connected to a particular disease, such as complement factor H and AMD, or autophagy and Crohn’s disease. In these cases, efforts directed toward developing potential therapies could begin immediately. In others, more work is needed to understand the clues that have been provided by GWA studies. 20 Hirschhorn · Gajdos It is important to realize that, because of the genetic correlation (linkage disequilibrium) between nearby variants (see sidebar “Comparison of Association and Linkage Analysis”), association studies do not usually pinpoint the variant responsible for the association, or even the gene that is affected by the associated variant. Instead, association studies typically highlight a small region that may contain several genes (although sometimes the relevant gene may be obvious from previous genetic or biological studies). Although many GWA studies typically report the nearest gene(s) as a way of identifying the location of an associated variant, connecting a specific gene with a trait or disease generally requires additional genetic, biological, or functional data. Thus, additional functional or genetic studies (e.g., sequencing) will often be needed in order to identify the relevant gene as a prerequisite to deciphering the relevant biology. Even if the relevant genes and biological pathways are understood, the time frame between biological knowledge and a new therapy can be long, as illustrated by the two decades that elapsed between Goldstein & Brown’s work implicating HMGCR and cholesterol metabolism in atherosclerosis (97) and the successful use of HMGCR inhibitors (statins) to prevent coronary artery disease (98). Where the genes and/or biology are unknown, the time frame will be longer. Still, GWA studies (and the studies that will follow in their wake) hold the promise of new and better therapies that target previously unsuspected aspects of disease biology that are genetically validated as relevant in patients. The promise of revolutionizing clinical medicine is great enough to justify follow-up studies based on the findings from these genetic studies. However, the likely time frame of these follow-up studies is long enough that the true level of success of genetic studies of common diseases and polygenic traits will be best judged in the coming decades rather than in the next few months or years. ME62CH02-Hirschhorn ARI 4 December 2010 11:3 DISCLOSURE STATEMENT The authors are not aware of any affiliations, memberships, funding, or financial holdings that might be perceived as affecting the objectivity of this review. Annu. Rev. Med. 2011.62:11-24. Downloaded from www.annualreviews.org by University of Oxford - Bodleian Library on 05/27/11. For personal use only. LITERATURE CITED 1. Glazier AM, Nadeau JH, Aitman TJ. 2002. Finding genes that underlie complex traits. Science 298:2345– 49 2. Altshuler D, Daly MJ, Lander ES. 2008. Genetic mapping in human disease. Science 322:881–88 3. Kaprio J, Tuomilehto J, Koskenvuo M, et al. 1992. Concordance for type 1 (insulin-dependent) and type 2 (non-insulin-dependent) diabetes mellitus in a population-based cohort of twins in Finland. Diabetologia 35:1060–67 4. Zdravkovic S, Wienke A, Pedersen NL, et al. 2002. Heritability of death from coronary heart disease: a 36-year follow-up of 20 966 Swedish twins. J. Intern. Med. 252:247–54 5. Sullivan PF, Kendler KS, Neale MC. 2003. Schizophrenia as a complex trait: evidence from a meta-analysis of twin studies. Arch. Gen. Psychiatry 60:1187–92 6. Beekman M, Heijmans BT, Martin NG, et al. 2002. Heritabilities of apolipoprotein and lipid levels in three countries. Twin Res. 5:87–97 7. Maes HH, Neale MC, Eaves LJ. 1997. Genetic and environmental factors in relative body weight and human adiposity. Behav. Genet. 27:325–51 8. Silventoinen K, Sammalisto S, Perola M, et al. 2003. Heritability of adult body height: a comparative study of twin cohorts in eight countries. Twin Res. 6:399–408 9. Risch N, Merikangas K. 1996. The future of genetic studies of complex human diseases. Science 273:1516– 17 10. Collins FS, Guyer MS, Charkravarti A. 1997. Variations on a theme: cataloging human DNA sequence variation. Science 278:1580–81 11. Harris H. 1975. The Principles of Human Biochemical Genetics. Amsterdam: North-Holland 12. Lander ES. 1996. The new genomics: global views of biology. Science 274:536–39 13. Reich DE, Lander ES. 2001. On the allelic spectrum of human disease. Trends Genet. 17:502–10 14. Clayton DG. 2009. Prediction and interaction in complex disease genetics: experience in type 1 diabetes. PLoS Genet. 5:e1000540 15. Zhernakova A, van Diemen CC, Wijmenga C. 2009. Detecting shared pathogenesis from the shared genetics of immune-related diseases. Nat. Rev. Genet. 10:43–55 16. Van Limbergen J, Wilson DC, Satsangi J. 2009. The genetics of Crohn’s disease. Annu. Rev. Genomics Hum. Genet. 10:89–116 17. Poirier J, Davignon J, Bouthillier D, et al. 1993. Apolipoprotein E polymorphism and Alzheimer’s disease. Lancet 342:697–99 18. Klein RJ, Zeiss C, Chew EY, et al. 2005. Complement factor H polymorphism in age-related macular degeneration. Science 308:385–89 19. Thein SL, Menzel S, Peng X, et al. 2007. Intergenic variants of HBS1L-MYB are responsible for a major quantitative trait locus on chromosome 6q23 influencing fetal hemoglobin levels in adults. Proc. Natl. Acad. Sci. USA 104:11346–51 20. Menzel S, Garner C, Gut I, et al. 2007. A QTL influencing F cell production maps to a gene encoding a zinc-finger protein on chromosome 2p15. Nat. Genet. 39:1197–99 21. Thein SL, Menzel S, Lathrop M, et al. 2009. Control of fetal hemoglobin: new insights emerging from genomics and clinical implications. Hum. Mol. Genet. 18:R216–23 22. Uda M, Galanello R, Sanna S, et al. 2008. Genome-wide association study shows BCL11A associated with persistent fetal hemoglobin and amelioration of the phenotype of beta-thalassemia. Proc. Natl. Acad. Sci. USA 105:1620–25 23. Jonas DE, McLeod HL. 2009. Genetic and clinical factors relating to warfarin dosing. Trends Pharmacol. Sci. 30:375–86 www.annualreviews.org • Genome-Wide Association Studies 21 ARI 4 December 2010 11:3 24. Lohmueller KE, Pearce CL, Pike M, et al. 2003. Meta-analysis of genetic association studies supports a contribution of common variants to susceptibility to common disease. Nat. Genet. 33:177–82 25. McCarthy MI, Abecasis GR, Cardon LR, et al. 2008. Genome-wide association studies for complex traits: consensus, uncertainty and challenges. Nat. Rev. Genet. 9:356–69 26. Wellcome Trust Case Control Consortium. 2007. Genome-wide association study of 14,000 cases of seven common diseases and 3,000 shared controls. Nature 447:661–78 27. Chanock SJ, Manolio T, Boehnke M, et al. 2007. Replicating genotype-phenotype associations. Nature 447:655–60 28. Clayton DG, Walker NM, Smyth DJ, et al. 2005. Population structure, differential bias and genomic control in a large-scale, case-control association study. Nat. Genet. 37:1243–46 29. Campbell CD, Ogburn EL, Lunetta KL, et al. 2005. Demonstrating stratification in a European American population. Nat. Genet. 37:868–72 30. Price AL, Zaitlen NA, Reich D, et al. 2010. New approaches to population stratification in genome-wide association studies. Nat. Rev. Genet. 11:459–63 31. Gabriel SB, Schaffner SF, Nguyen H, et al. 2002. The structure of haplotype blocks in the human genome. Science 296:2225–29 32. International HapMap Consortium. 2005. A haplotype map of the human genome. Nature 437:1299–320 33. Frazer KA, Ballinger DG, Cox DR, et al. 2007. A second generation human haplotype map of over 3.1 million SNPs. Nature 449:851–61 34. Ragoussis J. 2009. Genotyping technologies for genetic research. Annu. Rev. Genomics Hum. Genet. 10:117– 33 35. Marchini J, Howie B. 2010. Genotype imputation for genome-wide association studies. Nat. Rev. Genet. 11:499–511 36. Li Y, Willer C, Sanna S, et al. 2009. Genotype imputation. Annu. Rev. Genomics Hum. Genet. 10:387–406 37. Duerr RH, Taylor KD, Brant SR, et al. 2006. A genome-wide association study identifies IL23R as an inflammatory bowel disease gene. Science 314:1461–63 38. Rioux JD, Xavier RJ, Taylor KD, et al. 2007. Genome-wide association study identifies new susceptibility loci for Crohn disease and implicates autophagy in disease pathogenesis. Nat. Genet. 39:596–604 39. Parkes M, Barrett JC, Prescott NJ, et al. 2007. Sequence variants in the autophagy gene IRGM and multiple other replicating loci contribute to Crohn’s disease susceptibility. Nat. Genet. 39:830–32 40. Amundsdottir LT, Sulem P, Gudmundsson J, et al. 2006. A common variant associated with prostate cancer in European and African populations. Nat. Genet. 38:652–58 41. Gudmundsson J, Sulem P, Manolescu A, et al. 2007. Genome-wide association study identifies a second prostate cancer susceptibility variant at 8q24. Nat. Genet. 39:631–37 42. Sladek R, Rocheleau G, Rung J, et al. 2007. A genome-wide association study identifies novel risk loci for type 2 diabetes. Nature 445:881–85 43. Steinthorsdottir V, Thorleifsson G, Reynisdottir I, et al. 2007. A variant in CDKAL1 influences insulin response and risk of type 2 diabetes. Nat. Genet. 39:770–75 44. Saxena R, Voight BF, Lyssenko V, et al. 2007. Genome-wide association analysis identifies loci for type 2 diabetes and triglyceride levels. Science 316:1331–36 45. Scott LJ, Mohlke KL, Bonnycastle LL, et al. 2007. A genome-wide association study of type 2 diabetes in Finns detects multiple susceptibility variants. Science 316:1341–45 46. Zeggini E, Weedon MN, Lindgren CM, et al. 2007. Replication of genome-wide association signals in UK samples reveals risk loci for type 2 diabetes. Science 316:1336–41 47. Frayling TM, Timpson NJ, Weedon MN, et al. 2007. A common variant in the FTO gene is associated with body mass index and predisposes to childhood and adult obesity. Science 316:889–94 48. McPherson R, Pertsemlidis A, Kavaslar N, et al. 2007. A common allele on chromosome 9 associated with coronary heart disease. Science 316:1488–91 49. Easton DF, Pooley KA, Dunning AM, et al. 2007. Genome-wide association study identifies novel breast cancer susceptibility loci. Nature 447:1087–93 50. Hunter DJ, Kraft P, Jacobs KB, et al. 2007. A genome-wide association study identifies alleles in FGFR2 associated with risk of sporadic postmenopausal breast cancer. Nat. Genet. 39:870–74 Annu. Rev. Med. 2011.62:11-24. Downloaded from www.annualreviews.org by University of Oxford - Bodleian Library on 05/27/11. For personal use only. ME62CH02-Hirschhorn 22 Hirschhorn · Gajdos Annu. Rev. Med. 2011.62:11-24. Downloaded from www.annualreviews.org by University of Oxford - Bodleian Library on 05/27/11. For personal use only. ME62CH02-Hirschhorn ARI 4 December 2010 11:3 51. Todd JA, Walker NM, Cooper JD, et al. 2007. Robust associations of four new chromosome regions from genome-wide analyses of type 1 diabetes. Nat. Genet. 39:857–64 52. Botstein D, Risch N. 2003. Discovering genotypes underlying human phenotypes: past successes for Mendelian disease, future approaches for complex disease. Nat. Genet. 33(Suppl.):228–37 53. Kraft P, Hunter DJ. 2009. Genetic risk prediction—Are we there yet? N. Engl. J. Med. 360:1701–3 54. McClellan J, King MC. 2010. Genetic heterogeneity in human disease. Cell 141:210–17 55. Hirschhorn JN. 2009. Genomewide association studies—illuminating biologic pathways. N. Engl. J. Med. 360:1699–701 56. Hindorff LA, Sethupathy P, Junkins HA, et al. 2009. Potential etiologic and functional implications of genome-wide association loci for human diseases and traits. Proc. Natl. Acad. Sci. USA 106:9362–67 57. Rosenstiel P, Sina C, Franke A, et al. 2009. Towards a molecular risk map—recent advances on the etiology of inflammatory bowel disease. Semin. Immunol. 21:334–45 58. Barrett JC, Lee JC, Lees CW, et al. 2009. Genome-wide association study of ulcerative colitis identifies three new susceptibility loci, including the HNF4A region. Nat. Genet. 41:1330–34 59. Asano K, Matsushita T, Umeno J, et al. 2009. A genome-wide association study identifies three new susceptibility loci for ulcerative colitis in the Japanese population. Nat. Genet. 41:1325–29 60. Imielinski M, Baldassano RN, Griffiths A, et al. 2009. Common variants at five new loci associated with early-onset inflammatory bowel disease. Nat. Genet. 41:1335–40 61. Franke A, Balschun T, Sina C, et al. 2010. Genome-wide association study for ulcerative colitis identifies risk loci at 7q22 and 22q13 (IL17REL). Nat. Genet. 42:292–94 62. McGovern DP, Gardet A, Torkvist L, et al. 2010. Genome-wide association identifies multiple ulcerative colitis susceptibility loci. Nat. Genet. 42:332–37 63. Florez JC, Hirschhorn J, Altshuler D. 2003. The inherited basis of diabetes mellitus: implications for the genetic analysis of complex traits. Annu. Rev. Genomics Hum. Genet. 4:257–91 64. Voight BF, Scott LJ, Steinthorsdottir V, et al. 2010. Twelve type 2 diabetes susceptibility loci identified through large-scale association analysis. Nat. Genet. 42:579–89 65. Lyssenko V, Jonsson A, Almgren P, et al. 2008. Clinical risk factors, DNA variants, and the development of type 2 diabetes. N. Engl. J. Med. 359:2220–32 66. Ghoussaini M, Song H, Koessler T, et al. 2008. Multiple loci with different cancer specificities within the 8q24 gene desert. J. Natl. Cancer Inst. 100:962–66 67. Ahmadiyeh N, Pomerantz MM, Grisanzio C, et al. 2010. 8q24 prostate, breast, and colon cancer risk loci show tissue-specific long-range interaction with MYC. Proc. Natl. Acad. Sci. USA 107:9742–46 68. Wang K, Zhang H, Ma D, et al. 2009. Common genetic variants on 5p14.1 associate with autism spectrum disorders. Nature 459:528–33 69. Weiss LA, Arking DE, Daly MJ, et al. 2009. A genome-wide linkage and association scan reveals novel loci for autism. Nature 461:802–8 70. Merikangas AK, Corvin AP, Gallagher L. 2009. Copy-number variants in neurodevelopmental disorders: promises and challenges. Trends Genet. 25:536–44 71. Stankiewicz P, Lupski JR. 2010. Structural variation in the human genome and its role in disease. Annu. Rev. Med. 61:437–55 72. Berkel S, Marshall CR, Weiss B, et al. 2010. Mutations in the SHANK2 synaptic scaffolding gene in autism spectrum disorder and mental retardation. Nat. Genet. 42:489–91 73. Hegele RA. 2009. Plasma lipoproteins: genetic influences and clinical implications. Nat. Rev. Genet. 10:109–21 74. Cohen JC, Kiss RS, Pertsemlidis A, et al. 2004. Multiple rare alleles contribute to low plasma levels of HDL cholesterol. Science 305:869–72 75. Teslovich TM, Musunuru K, Smith AV, et al. 2010. Biological, clinical and population relevance of 95 loci for blood lipids. Nature 466:707–13 76. Musunuru K, Strong A, Frank-Kamenetsky M, et al. 2010. From noncoding variant to phenotype via SORT1 at the 1p13 cholesterol locus. Nature 466:714–19 77. Johansen CT, Wang J, Lanktree MB, et al. 2010. Excess of rare variants in genes identified by genome-wide association study of hypertriglyceridemia. Nat. Genet. 42:684–87 www.annualreviews.org • Genome-Wide Association Studies 23 ARI 4 December 2010 11:3 78. Ripatti S, Tikkanen E, Orho-Melander M, et al. 2010. A multi-locus genetic risk score and risk for incident coronary heart disease. Lancet 376:1393–400 79. Fisher RA. 1918. The correlation between relatives on the supposition of Mendelian inheritance. Trans. R. Soc. Edinb. 52:399–433 80. Lango Allen H, Estrada K, Lettre G, et al. 2010. Hundreds of variants influence height and cluster in genomic loci and biological pathways. Nature 467:832–38 81. Yang J, Benyamin B, McEvoy BP, et al. 2010. Common SNPs explain a large proportion of the heritability for human height. Nat. Genet. 42:565–69 82. Lettre G, Sankaran VG, Bezerra MA, et al. 2008. DNA polymorphisms at the BCL11A, HBS1L-MYB, and beta-globin loci associate with fetal hemoglobin levels and pain crises in sickle cell disease. Proc. Natl. Acad. Sci. USA 105:11869–74 83. Sankaran VG, Xu J, Ragoczy T, et al. 2009. Developmental and species-divergent globin switching are driven by BCL11A. Nature 460:1093–97 84. Sankaran VG, Menne TF, Xu J, et al. 2008. Human fetal hemoglobin expression is regulated by the developmental stage-specific repressor BCL11A. Science 322:1839–42 85. Manolio TA, Collins FS, Cox NJ, et al. 2009. Finding the missing heritability of complex diseases. Nature 461:747–53 86. McCarthy MI, Hirschhorn JN. 2008. Genome-wide association studies: potential next steps on a genetic journey. Hum. Mol. Genet. 17:R156–65 87. Purcell SM, Wray NR, Stone JL, et al. 2009. Common polygenic variation contributes to risk of schizophrenia and bipolar disorder. Nature 460:748–52 88. Nejentsev S, Walker N, Riches D, et al. 2009. Rare variants of IFIH1, a gene implicated in antiviral responses, protect against type 1 diabetes. Science 324:387–89 89. Farooqi IS, Yeo GS, Keogh JM, et al. 2000. Dominant and recessive inheritance of morbid obesity associated with melanocortin 4 receptor deficiency. J. Clin. Invest. 106:271–79 90. Ji W, Foo JN, O’Roak BJ, et al. 2008. Rare independent mutations in renal salt handling genes contribute to blood pressure variation. Nat. Genet. 40:592–99 91. Vaisse C, Clement K, Durand E, et al. 2000. Melanocortin-4 receptor mutations are a frequent and heterogeneous cause of morbid obesity. J. Clin. Invest. 106:253–62 92. Rogowski WH, Grosse SD, Khoury MJ. 2009. Challenges of translating genetic tests into clinical and public health practice. Nat. Rev. Genet. 10:489–95 93. Kaye J. 2008. The regulation of direct-to-consumer genetic tests. Hum. Mol. Genet. 17:R180–83 94. Lai-Goldman M, Faruki H. 2008. Abacavir hypersensitivity: a model system for pharmacogenetic test adoption. Genet. Med. 10:874–78 95. Fellay J, Thompson AJ, Ge D, et al. 2010. ITPA gene variants protect against anaemia in patients treated for chronic hepatitis C. Nature 464:405–8 96. Knowler WC, Barrett-Connor E, Fowler SE, et al. 2002. Reduction in the incidence of type 2 diabetes with lifestyle intervention or metformin. N. Engl. J. Med. 346:393–403 97. Goldstein JL, Brown MS. 1973. Familial hypercholesterolemia: identification of a defect in the regulation of 3-hydroxy-3-methylglutaryl coenzyme A reductase activity associated with overproduction of cholesterol. Proc. Natl. Acad. Sci. USA 70:2804–8 98. Pedersen TR, Kjekshus J, Berg K, et al. 1994. Randomised trial of cholesterol lowering in 4444 patients with coronary heart disease: the Scandinavian Simvastatin Survival Study (4S). Lancet 344:1383–89 Annu. Rev. Med. 2011.62:11-24. Downloaded from www.annualreviews.org by University of Oxford - Bodleian Library on 05/27/11. For personal use only. ME62CH02-Hirschhorn 24 Hirschhorn · Gajdos ME62-Frontmatter ARI 15 December 2010 15:56 Annual Review of Medicine Annu. Rev. Med. 2011.62:11-24. Downloaded from www.annualreviews.org by University of Oxford - Bodleian Library on 05/27/11. For personal use only. Contents Volume 62, 2011 Role of Postmarketing Surveillance in Contemporary Medicine Janet Woodcock, Rachel E. Behrman, and Gerald J. Dal Pan p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p 1 Genome-Wide Association Studies: Results from the First Few Years and Potential Implications for Clinical Medicine Joel N. Hirschhorn and Zofia K.Z. Gajdos p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p11 Imaging of Atherosclerosis D.R.J. Owen, A.C. Lindsay, R.P. Choudhury, and Z.A. Fayad p p p p p p p p p p p p p p p p p p p p p p p p p p p25 Novel Oral Factor Xa and Thrombin Inhibitors in the Management of Thromboembolism Bengt I. Eriksson, Daniel J. Quinlan, and John W. Eikelboom p p p p p p p p p p p p p p p p p p p p p p p p p p p41 The Fabry Cardiomyopathy: Models for the Cardiologist Frank Weidemann, Markus Niemann, David G. Warnock, Georg Ertl, and Christoph Wanner p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p59 Kawasaki Disease: Novel Insights into Etiology and Genetic Susceptibility Anne H. Rowley p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p69 State of the Art in Therapeutic Hypothermia Joshua W. Lampe and Lance B. Becker p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p79 Therapeutic Potential of Lung Epithelial Progenitor Cells Derived from Embryonic and Induced Pluripotent Stem Cells Rick A. Wetsel, Dachun Wang, and Daniel G. Calame p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p95 Therapeutics Development for Cystic Fibrosis: A Successful Model for a Multisystem Genetic Disease Melissa A. Ashlock and Eric R. Olson p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p 107 Early Events in Sexual Transmission of HIV and SIV and Opportunities for Interventions Ashley T. Haase p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p 127 HIV Infection, Inflammation, Immunosenescence, and Aging Steven G. Deeks p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p 141 v ME62-Frontmatter ARI 15 December 2010 15:56 The Increasing Burden of HIV-Associated Malignancies in Resource-Limited Regions Corey Casper p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p 157 Biliary Atresia: Will Blocking Inflammation Tame the Disease? Kazuhiko Bessho and Jorge A. Bezerra p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p 171 Advances in Palliative Medicine and End-of-Life Care Janet L. Abrahm p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p 187 Annu. Rev. Med. 2011.62:11-24. Downloaded from www.annualreviews.org by University of Oxford - Bodleian Library on 05/27/11. For personal use only. Clostridium difficile and Methicillin-Resistant Staphylococcus aureus: Emerging Concepts in Vaccine Development David C. Kaslow and John W. Shiver p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p 201 Antiestrogens and Their Therapeutic Applications in Breast Cancer and Other Diseases Simak Ali, Laki Buluwela, and R. Charles Coombes p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p 217 Mechanisms of Endocrine Resistance in Breast Cancer C. Kent Osborne and Rachel Schiff p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p 233 Multiple Myeloma Jacob Laubach, Paul Richardson, and Kenneth Anderson p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p 249 Muscle Wasting in Cancer Cachexia: Clinical Implications, Diagnosis, and Emerging Treatment Strategies Shontelle Dodson, Vickie E. Baracos, Aminah Jatoi, William J. Evans, David Cella, James T. Dalton, and Mitchell S. Steiner p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p 265 Pharmacogenetics of Endocrine Therapy for Breast Cancer Michaela J. Higgins and Vered Stearns p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p 281 Therapeutic Approaches for Women Predisposed to Breast Cancer Katherine L. Nathanson and Susan M. Domchek p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p 295 New Approaches to the Treatment of Osteoporosis Barbara C. Silva and John P. Bilezikian p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p 307 Regulation of Bone Mass by Serotonin: Molecular Biology and Therapeutic Implications Gerard Karsenty and Vijay K. Yadav p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p 323 Alpha-1-Antitrypsin Deficiency: Importance of Proteasomal and Autophagic Degradative Pathways in Disposal of Liver Disease–Associated Protein Aggregates David H. Perlmutter p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p 333 Hepcidin and Disorders of Iron Metabolism Tomas Ganz and Elizabeta Nemeth p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p 347 vi Contents ME62-Frontmatter ARI 15 December 2010 15:56 Interactions Between Gut Microbiota and Host Metabolism Predisposing to Obesity and Diabetes Giovanni Musso, Roberto Gambino, and Maurizio Cassader p p p p p p p p p p p p p p p p p p p p p p p p p p p p 361 The Brain-Gut Axis in Abdominal Pain Syndromes Emeran A. Mayer and Kirsten Tillisch p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p 381 Cognitive Therapy: Current Status and Future Directions Aaron T. Beck and David J.A. Dozois p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p 397 Annu. Rev. Med. 2011.62:11-24. Downloaded from www.annualreviews.org by University of Oxford - Bodleian Library on 05/27/11. For personal use only. Toward Fulfilling the Promise of Molecular Medicine in Fragile X Syndrome Dilja D. Krueger and Mark F. Bear p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p 411 Stress- and Allostasis-Induced Brain Plasticity Bruce S. McEwen and Peter J. Gianaros p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p 431 Update on Sleep and Its Disorders Allan I. Pack and Grace W. Pien p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p 447 A Brain-Based Endophenotype for Major Depressive Disorder Bradley S. Peterson and Myrna M. Weissman p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p 461 Indexes Cumulative Index of Contributing Authors, Volumes 58–62 p p p p p p p p p p p p p p p p p p p p p p p p p p p 475 Cumulative Index of Chapter Titles, Volumes 58–62 p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p 479 Errata An online log of corrections to Annual Review of Medicine articles may be found at http://med.annualreviews.org/errata.shtml Contents vii