Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Zinc finger nuclease wikipedia , lookup
Gene regulatory network wikipedia , lookup
Nucleic acid analogue wikipedia , lookup
Endogenous retrovirus wikipedia , lookup
Biosynthesis wikipedia , lookup
Genomic library wikipedia , lookup
Non-coding DNA wikipedia , lookup
Alternative splicing wikipedia , lookup
Bisulfite sequencing wikipedia , lookup
Gene expression wikipedia , lookup
Gene therapy wikipedia , lookup
Gene therapy of the human retina wikipedia , lookup
Vectors in gene therapy wikipedia , lookup
Real-time polymerase chain reaction wikipedia , lookup
Personalized medicine wikipedia , lookup
Deoxyribozyme wikipedia , lookup
Genetic code wikipedia , lookup
Community fingerprinting wikipedia , lookup
Silencer (genetics) wikipedia , lookup
Artificial gene synthesis wikipedia , lookup
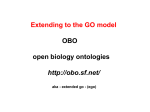
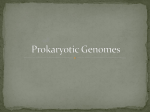
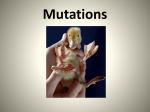
From www.bloodjournal.org by guest on June 14, 2017. For personal use only. The Wiskott-Aldrich Syndrome and X-Linked Congenital Thrombocytopenia Are Caused by Mutations of the Same Gene By Qili Zhu, Min Zhang, R. Michael Blaese, Jonathan M.J. Derry, Anne Junker, Uta Francke, Shi-Han Chen, and Hans D. Ochs The Wiskott-Aldrich syndrome (WAS) is an X-linked recessivedisordercharacterizedbythrombocytopenia,small platelets,eczema,recurrentinfections,andimmunodeficiency. Besidesthe classic WAS phenotype,there is a group of patients with congenitalX-linkedthrombocytopenia (XLT) who have small platelets but only transient eczema, if any, and minimal immune deficiency. Because the gene responsible for WAS has been sequenced, it was possible to correlatethe WAS phenotypeswith WAS gene mutations. Using a fingerprinting screening technique, we determined the approximate location of the mutation in 13 unrelated WAS patients with mild to severe clinical symptoms. Direct sequence analysis of cDNA and genomic DNA obtainedfrom patient-derived cell lines showed 12 unique mutations distributed throughout the WAS gene, including insertions, deletions, and point mutations resulting in amino acid substiOf 4 tutions, termination, exon skipping, or splicing defects. unrelated patients with the XLT phenotype,3 had missense mutations affecting exon2 and 1 had a splice-sitemutation affecting exon 9. Patients with classic WAS had more complex mutations, resultingin termination codons, frameshift, andearly termination. Thesefindingsprovidedirectevidence that XLT and WAS are caused by mutations of the same gene and suggestthat severe clinical phenotypes are associated with complex mutations. 0 1995 by The American Societyof Hematology. T severity of WAS-associated symptoms was scored from 1 to 5 , based on the following criteria. A score of 1 was given to patients with thrombocytopenia and small sized platelets, but without any other symptoms or clinical findings. Patients with platelet abnormalities and a history of mild, transient, eczema, with or without minor infections, received a score of 2. Patients with persistent but manageable eczema, with recurrent infections, or with both received a score of 3. Those patients with persistent and difficult to control eczema associated with frequent potentially life-threatening infections were scored as 4. A score of 5 was assigned if patients presenting with eczema and/or frequent infections developed autoimmune disease. Seven of the 13 families reported more than 1 affected male patient. Of the 13 unrelated WAS patients included in this study, 1 infant (BM), diagnosed prenatally by linkage analysis and receiving a transplant at 1 month of age with bone marrow from an HLA-matched sibling had not been observed long enough to be scored; up to the time of marrowtransplantation, BM‘s only findings were thrombocytopenia, small platelets, and petechiae. However, his older brother, who died of meningitis at 6 years of age, had severe clinical symptoms and was assigned a score of 4.Patient AR, who presented with congenital thrombocytopenia and persistent small platelet size, but HE WISKOTT-ALDFUCH syndrome (WAS) is an Xlinked recessive disorder characterized by thrombocytopenia, small platelet volume, eczema, recurrent bacterial and viral infections, autoimmune diseases, increased risk of maligancies, and abnormal B- and T-cell f~ncti0n.l.~ Patients with WAS respond poorly to immunization with polysaccharides and certain protein antigen^,^.^ and lymphocyte proliferation in response to mitogens and antigens is variably dep r e ~ s e d Distinguishable .~ from this classic WAS phenotype are boys with X-linked thrombocytopenia (XLT) whose platelets are small and who either are free of eczema6”’ or have a history of only mild and transient Most patients with XLT have normal susceptibility to infections and normal immune functions. The gene for XLT has been mapped to Xpll.22, the same band to which the classic WAS phenotype had been mapped?~”~12 The gene responsible for WAS has been isolated, cloned, and ~equenced.’~ Encoded by 12 exons and composed of 1,823 bp, the cDNA encodes a 502-amino acid, proline-rich protein (WAS protein) of unknown function that appears to be of central importance for the function of hematopoietic cell lineages.13.14 WASgene transcript was absent in 2 of 5 Epstein-Barr virus (EBV)-transformed B-lymphoblastoid cell lines (B-LCL) derived from affected male patients, and sequence analysis of genomic DNA showed three independent mutations, strongly suggesting that the newly identified gene was the WAS gene.” To determine the mutation pattern of the WAS gene and to correlate location and type of mutations with clinical phenotypes, we studied 13 additional unrelated WAS families whose affected members presented with mild to severe disease. Twelve unique mutations, which were distributed throughout the WAS gene, were identified and included insertions, deletions, and point mutations resulting in stop codons, amino acid substitutions, exon skipping, or splicing defects. MATERIALS AND METHODS Patients and Their Phenotypes Affected members of 13 unrelated WAS families with variable phenotypes were included in this analysis (Table 1). All patients had in common thrombocytopenia and small platelet volume. The Blood, Vol 86, No 10 (November 15). 1995: pp 3797-3804 From the Department of Pediatrics,University of Washington School of Medicine, Seattle, WA;the Clinical Gene Therapy Branch, National Centerfor Human Genome Research, National Institutes of Health, Bethesda. MD; Howard Hughes Medical Institute, Beckman Center for Molecular and Genetic Medicine, Stanford University Medical Center,Stanford, CA; the Department of Pediatrics, University of British Columbia, Vancouver, British Columbia, Canada. Submitted June 12, 1995; accepted July 18, 1995. Supported bygrantsfrom the National lnstitutes of Health (H017427 [H.D.O.]),the March of Dimes and Birth Defects Foundation (6-0116 [H.D.O.] and 6-0694 [S.-H.C.]), and the Howard Hughes Medical Institute (Investigator [U.F.] and Associate [J.M.J.D.]),and in part by B.C. Medical Services Foundation 5 S4511 (A.J.). A portion of this work was conducted through the Clinical Research Center of the University of Washington (RR-37). Address reprint requests to Hans D. Ochs, MD, Department of Pediatrics, RD-20, University of Washington School of Medicine, Seattle, WA 98195. The publication costsof this article were defrayedin part by page chargepayment. This article must therefore be hereby marked “advertisement” in accordance with 18 U.S.C. section 1734 solely to indicate this fact. 0 1995 by The American Society of Hematology. 0006-4971/95/8610-0013$3.00/0 3797 mic From www.bloodjournal.org by guest on June 14, 2017. For personal use only. 3798 ZHU ET AL Table 1. Clinical Phenotypes and Mutations of the WASP Gene Observed in 12 Unrelated Patients With WAS Other Affected Mutation Members Family Patient Score* Transcriptt(Score*) AR CS JS BG Exon 1 0 ND 2 2 2 1 (2) ++ 0 (+) (+) 2 4 2 (2, 2) 2 2 9 5 1 (5) 0 ++ ++ TH 5 4 3 (4. 4, 2) (+) 1 10 RM 5 0 (-) 3 MB 4 5 (all 4) (+) 9 MS DM BM* - 1 (4) + EA PP 3 4 0 2 (4. 4) (+) 1 ++ 10/11 CR 5 0 (+) 10 DNA C290T ArgE6Cys C290T C174A Ala47Asp A953G (ATG bp gtg) G407A C71T C995T C329T 11 cDNA + 13 t + c at +2nt of - intron 9 t c at +2nt of intron 11 61-65 i n s C 9 bp del, 11 bp ins intron 10 del1301-1305 G Mutation Expected Effect C290T C290T C174A del Arg86Cys Frameshiftrer G407A C71T C995T Skipping of exon 3 (87 bpK329T 965 ins 114 bp Gly125Arg Argl3Ter Arg32lTer Truncated protein Skipping exon 11 (115 bp) 61-65 ins C 1372 ins 13 bp del 38 aa, frameshift del1301-1305 G ins 38 aa Frameshimer Frameshimer Frameshimer * Scoring system is described in text. t Determined by Northernblot(Fig 2); ++ and + indicate normal amounts of transcript, (+) indicates severely reduced but detectable transcript, and (-) indicates transcript that is undetectable by Northern blot but detectable by RT-PCR. When marrow transplantation was performed at 1 month of age, BM had no symptoms other than thrombocytopenia, small platelets, and petechiae. * without eczema or increased susceptibility to infections, was evaluated carefully and found to be immunologically normal; he was given a score of 1. However, shortly after splenectomy, AR developed pneumococcal sepsis, suggesting that hemay have mild immune deficiency. All of the remaining 11 patients had additional symptoms, including various degrees of immune abnormalities. Three patients (CS, JS, and BG) with transient, mild eczema and infrequent infections responding well to antibiotics were given scores of 2. One patient (EA) whose persistent eczema and infections were wellcontrolled by standard therapy was given a score of 3. The remaining 7 patients had severe clinical symptoms and were given a score of 4 if without and a score of 5 if with symptoms of an autoimmune disorder. Cell Lines B-LCLs established by inoculating peripheral blood mononuclear cells (PBMCs) with supernatants from the marmoset cell line B95.8I5 were available from all but 1 WAS patient. From patient AR, mRNA and genomic DNA were isolated from frozen spleen cells that had been obtained during splenectomy. Selection of Primers Primers for amplification of cDNA and genomic DNA and for dideoxynucleotide fingerprinting were selected from theknown cDNA and genomic DNA sequences of the WAS gene'3 and designed to identify the mutations of our patient population (Table 2). RNA Isolation and Reverse Transcriptase-Polymerase Chain Reaction (RT-PCR) RNA isolation andRT-PCR were performed as previously described.16 Briefly, total RNA was isolated from B-LCLs or spleen cells using a single-step method and Trizol (GIBCO BRL, Gaithersburg, MD). The first-strand cDNA was synthesized by incubating 2.5 pg of total RNA with oligo (dT) as primer using the Superscrip Preamplification System kit (GIBCO BRL), as recommended by the manufacturer. The WAS protein cDNA was amplifed by PCR in two overlapping fragments. For reaction 1 (Table 2), PCR underwent 35 cycles in20 mmol/L Tris-HC1 (pH 8.4). 50 mmol/L KCI, 1.5 mmoULMgCI,, 0.2 mmol/L dNTP, 0.5 pmol/L primers W-2 and 5.24, 5 pL first-strand cDNA products, and 2.5 U Taq polymerase (GIBCO BRL) in a total volume of 100 pL at 94°C for 1 minute, 57°C for 1 minute, 72°C for 1.5 minutes, and a final extension step at 72°Cfor 10 minutes. For reaction 2 (Table 2), PCR wasperformed in20 mmom Tris-HC1 (pH 8.8). 10 mmol/L KC], 10 mmol/L (NH&S04, 2 mmol/L MgSO,, 0.1% Triton X-100, 0.1 mg/mL bovine serum albumin (BSA), 0.2 mmom dNTP, 0.5 pmol/L primers W-906 and W-l708c, 5 pL of the first-strand cDNA products, 2.5 U of the Taq Extender PCR additive (Stratagene, La Jolla, CA), and 2.5 U Taq polymerase in a total volume of 100 p L at 94°C for 1 minute, 57°C for 1 minute, 72°C for 1.5 minutes, and a final extension step at 7 2 T for 5 minutes for 35 cycles. The PCR products were purified by agarose gel electrophoresis. Dideoxynuckotide Fingerprinting (ddF) and Direct Sequencing of cDNA To screen the amplified WAS protein cDNA for mutations, we used the modified ddF method originally described by Sarkar et a1" and the fmol cycle sequencing kit (Promega, Madison, WI). Briefly, 50 to 75 ngof amplified cDNA, 2 pL ddC/dC mixture, 0.25 p L (0.25 pmol) "P end-labeled primer, 1.25 pL 5X sequence buffer, 0.25 pL Taq polymerase, and distilled H20 to a total volume of 6 pL was incubated in an automatic DNA thermal cycler (PerkinElmer, Norwalk, CT) at 95°C for 30 seconds, 60°C for 30 seconds, and 72°C for 1 minute for 30 cycles. The resulting products were electrophoresed in 5% polyacrylamide nondenaturing gels at 4°C. The mutations suggested by ddF were confirmed by direct sequenc- From www.bloodjournal.org by guest on June 14, 2017. For personal use only. WASP GENE MUTATIONS X-THROMBOCYTOPENIA IN WAS AND 3799 Table 2. Primw PainUsed for Fingerprinting and MutationAnalysis of cDNA and GenomkDNA in 12 WAS Families Primers Reaction W3'P Fragment Size Positiont W-2* 5.24 GCCTCGCCAGAGAAGACAAG GCAATCCCCAAAGGTACAGG 2-2 1 1064-1083 W-906$ W-1708cS ACGACTTCATTGAGGACCAG TGAGTGTGAGGACCAGGCAG 906-925 1688-1707 W-2 W-l5 6 ~ W-215 W-i2c W-325 W-496c GCCTCGCCAGAGAAGACAAG CGTCCAAGCATCTCAAAGAG GCTGAGCACTGGACCAAGGA ACTGGCTTGCAAGTCCAGTC GGAACAGGAGCTGTACTCAC TCCACmGCCTCTGATTCC 2-21 137-156 215-234 Intron 2 ( + l 8 to +37) 325-344 477-496 6 W-i2 W-i4c GTGCCTCAGTGCCACTGTGC CTCACCTCTGCCCAACTTCC Intron 2 ( --23 to -42) Intron 4 (.t25 to +44) 7 5.28 5.24 CAAGAGGmCACTATGAAGG GCAATCCCCAAAGGTACAGG Intron 7 ( --51 to -71) 1064-1083 W-1157* W-1472~ ACTGGACGTTCTGGACCACTG CTCTGCTTCTCTTCTGCATC 1157-1177 1453-1472 5.30 W-illc GGGAGAAATGCTCCmCC ACGAGGCTGACACAAGAlTC Intron 10 (-40 to -58) Intron 11 (+l19 to +138) 1 2 3 4 5 Exon 1: Exon 2-9: 118 Exon 10: 165 Exon 9: Exon 10-11: 220 Exon 12: 155 Exon 1: 799 60 522 93 Exon 2: Intron 2: Exon 3: Intron 3: Exon 4: Intron 2: Exon 3: Intron 3: Exon 4: Intron 4 Intron 7: Exon 8: Intron 8: Exon 9: Intron 9: Exon 1 0 Exon 10: Intron 10: Exon 11: Intron 10: 37 70 100 102 42 87 100 103 44 71 43 201 154 205 118 216 251 100 58 Exon 11: Intron 11: 115 128 Primers listed for reactions 1 and 2 were used to amplify WAS protein cDNA in two overlapping fragments. The other primers (reactions 3 through 9) were used to amplify genomic DNA of fragment size listed. t The numbers represent the cDNA sequence position of exons or, if indicated, the position within introns. + indicates the position counted from the 5' splice site of an intron; - indicates the position counted from the 3' splice site. Used also for dideoxynucleotide fingerprinting, together with primers W-249 (starting at cDNA nucleotide 249) (5"GTGCTTCGTGAAGGATAACC), W-516 (5'-ACCACCAACACCAGCCAATG),W-756 (5'-CCAGTGGATTCAAGCATGTC), and W-l406 (5'-CCACCACCTCAGAGCTCAGA). * ing using selected primers and the fmol cycle sequencing kit (Promega) according to the manufacturer's recommendation. DNA Pur$cation and Sequencing of Genomic DNA resed through agaroselformaldehyde gel and transferred to a nylon membrane (Magna NT, MSI, Westboro, MA). The radiolabeled WAS protein cDNA clone M5.5, a 750-bp cDNA fragment o f the WAS gene, was used as probe for hybridization, as previously de~cribed.'~ After enrichment for Poly A (+) mRNA, the larger of the two transcripts originally describedr3was no longer present, leaving only the 2.0-kb transcript. DNA was extracted from B-LCLs or spleen cells as previously described.I6 Purified genomic DNA samples were amplified with primer pairs (Table 2) designed to span the suspected mutation sites. The PCR conditions used were as follows. For reactions 3 through 7 (Table 2), the samples were incubated for 5 minutes at94°C followed by 30 cycles at 94°C for 1 minute, 55°C for 1 minute, and 72°C for 1 minute. The conditions for reactions 8 and 9 (Table 2) were identical to those for reaction 2, which have been already described. The amplifiedDNA fragments were separated by agarose gel electrophoresis and electroelution. Direct sequencing was perfomed by the dideoxynucleotide chain termination method," using either the sequenase DNA sequencing kit (US Biochemical Corp, Cleveland, OH)or the fmol cycle sequencing kit (Promega) as recommended by the manufacturers. To identify theapproximate location of mutations, we screened the entire coding region and part of the noncoding region of WASprotein cDNA withddF. This procedure showed abnormal sequences in all 13 patients reported here and allowed us to predict the approximate location of each defect. AdditionalWASpatientsneedto be studiedin a similar manner to determine the overall effectiveness of this method in detecting mutations. Northern Blot Analysis Direct Sequencing of cDNA and Genomic DNA Poly A (+) mRNA samples isolated from 30 p g total RNA with the PolyATtract mRNA isolation system (Promega) were electropho- OnlyafterintroducingtheTaqExtender PCR additive provided by Stratagene were we able to consistently obtain RESULTS Screening for Mutations by ddF From www.bloodjournal.org by guest on June 14, 2017. For personal use only. ZHU ET AL 3800 61-65ins c C329T(stop) Skipping of exon3 t + c,+2 n.t., ins of 114 bD 1372 ins 13 bp I / / / / + / exon 1 2 3 4 5 6 7 8 9 10 l1 12 C201T” 21l del T’ /\ G” G291A’512-516ins C741 C” G2911T’ Fig 1. Schematic representation of the WAS gene showing the location of the mutations and nucleotide changes. *Patients reported in Derry et al.” “Patients reported in Villa et al.” PCR products from exons 10 and 11. Single nucleotide substitutions (point mutations), observed in the genomic DNA of 10 patients withninenovelmutations,werethemost frequent mutations; in the remaining 3 patients, we found insertions or deletions of nucleotides within the genomic DNA (Table I and Fig 1). Pointmutations resulting in XLT. Two unrelatedpatients (AR and CS) with a mild phenotype (scores of l and 2) had the same missense mutation, a C * T transition at position 290 in exon 2, resulting in the substitution of arginine with cystein (Arg86Cys). This mutation had no effect on the amount of mRNA (Fig 2, lane 2). Patient JS had a C A transversion at position 174 in exon 2, resulting in the substitution of alanine with aspartic acid (Ala47Asp) and a markedreduction in theamount of transcript (datanot shown). cDNA analysis of patient BG showed a deletion of the last 13 bp of exon 9 (bp953-965) due to an A + G transition at position953 of genomic DNA. Instead ofchanging the normal codon 307 from ATG (Met) to GTG (Val), this mutation activates a cryptic splice site at 13 nucleotides 5‘ to the normal splice site (5’-GAGgtgagg-3’; Fig 3). The deletion of 13 nucleotides results in frameshift and premature termination 137 triplets downstream in exon IO. Northern blot analysis of BG’s B-LCLs indicates markedly reduced transcript (Fig 2, lane 8). Point mutations resulting in classic WAS. Patient MS with a severe form of WAS hada G + A transition at position 407 in exon 4, resulting in the substitution of glycine with arginine (Glyl25Arg). This missense mutation did not interfere with transcription (Fig 2, lane 3). Two patients (DM and TH), both with severe WAS, were found to have nonsense mutations due to single nucleotide substitutions resulting in termination codons. DM had a C * T transition at position 71 in exon 1 (Arg13Ter) and normal amount of transcript (Fig 2, lane 4). TH had a C T transition at position 995 in exon 10 (Arg321Ter) and reduced transcript (Fig 2, lane 5). The PCR-amplified cDNA obtained from a B-LCLof patient RM consisted of a strong band that migrated faster than the normal product and a second, much fainter band (<25%) of normalsize.Direct sequence analysis of the faster migrating, dominant band of RM’s amplified cDNA showed a deletion of 87 bp, representing exon 3. Sequence 1 2 3 4 5 6 7 8 9 l0111213 - + + Fig 2. Northern blot analysis of WAS gene expression. PolyA (+I mRNA was electrophoresed and transferred to a nylon membrane, and the blot was probed with the radiolabeled WAS protein cDNA clone M5.5. Lane 1 represents a B-LCL from a normal control. Lanes 2 through 13 are WAS patients CS (lane 21, M S (3). DM (4). TH (5). R M (6). M B (71, BG 181, B M (91, EA (101, PP (111, and CR (12). In lane 13, mRNA from patient JNl.l.l, known to have a markedly reduced tran~cript,’~ is shown as a negative control. A strong single band of 2.0 kbcould be identified in the normal control andin the lanes representingfive WAS patients. A control hybridizationwith pactin cDNA (2.0 kbl is provided in each lane. From www.bloodjournal.org by guest on June 14, 2017. For personal use only. GENE WASP MUTATIONS IN WAS AND X-THROMBOCYTOPENIA :\ 3801 A 1 c c G A G G Fig3.Sequenceanalysis of cDNA and genomic DNA derived from Datient BG shows a deletion of 13 bp involving nucleotides 953 to 965 at the 3' end of exon 9 caused by an A G transition at position 953. This mutation generated a new splice site (gtg) within exon 9. The deleted segment is boxed. - \ cDNA Normal BG G T \l A G G A c G G analysis of genomic DNA showed that the skipping of exon 3 was the direct consequence of a nonsense mutation, a C 4T transition, affecting nucleotide 329 in exon 3 (Fig 4); this would result in the formation of a termination codon (Gln99Ter). To explore the possibility of alternative splicing, we sequenced individual clones of RM's cDNA after PCR amplification. Ten clones were found to have exon 3 deleted and 3 clones were of normal size and contained the termination codon. Northern blot analysis failed to detect transcript (Fig 2, lane 6), suggesting that both mRNA populations are poorly transcribed or unstable, although definitively present as shown by RT-PCR. The t -P c transition at position +2 of the 5' splice site of intron 9 of patient MB resulted in the activation of a cryptic splice site and the insertion of the 5' segment of intron 9 consisting of 114 bp into this patient's cDNA. This insertion caused frameshift and a termination codon within the inserted segment. On Northern blot, the amount of mRNA detected was severely reduced and appeared to migrate slower (Fig 2, lane 7). In patient BM, the t 4 c transition at position + 2 of the 5' splice site of intron cDNA \ \ / Normal RM GATC GATC 1g G 1 1 resulted in the deletion of exon 11 (1 15 bp) due to loss of the donor splice site. The resulting mRNA is abundant and, as expected, of smaller size (Fig 2, lane 9). A protein made from this transcript would lack38 amino acids encoded by exon 11 and, because of frameshift, would be unstable. Insertions and deletions affecting genomic DNA resulting in classic WAS. In 3 unrelated WAS patients, the mutations were due to the insertion or the deletion of nucleotides from genomic DNA. EA was found to have a single nucleotide (C) insertion between nucleotides 61 and 65 (GCCCG GCCCCG) of exon I, affecting codon 11 and resulting in frameshift and premature termination at codon 37; the amount of mRNA on Northern blot was markedly reduced (Fig 2, lane 10). A deletion and insertion of small DNA fragments, observed in genomic DNA of patient PP, resulted in a new splice site and the addition of 13 bp derived from intron 10 (Fig 5), causing premature termination close to the 3'end of exon 12. A B-LCL derived from this patient contained abundant mRNA (Fig 2, lane 11). A proteinmade from this transcript would be 4 amino acids shorter but most / / \ v C \: C Fig 4. Sequenceanalysis of cDNA and genomic DNA of the WAS gene from a normal control and patient RM. Analysis of cDNA obtained from an EBV-induced B-LCL established from patient RM shows a deletion of exon 3. Thisdeletion is due to a C -Ttransition affecting nucleotide 329 within exon 3, resulting in a termination codon and the skipping of an exon. From www.bloodjournal.org by guest on June 14, 2017. For personal use only. ZHU ET AL 3802 A B G G C G A E\ g G T G G C A \ T Genomic DNA Normal PP C C C C T G G G i C B A C A C C del r - - - - - - - - - -INormal-ccctctgtgdtgetccctd.. III1IIIIII I I I I I I I I I I PP t G C A A a C D c' Intron 10 Exon 11 c c t g c t g c ~ A C C C C T G G G G C C C C A G A GIIIIIIIIIIIIIIIIIIIIIIIIIIII I I I I I I I I , I I I I , I I I I J I I I , I , , I , -c c ctc 1gtgc at c t g I L"""""""1 ACCCCTGGGGCCCCAGAG Ins Intron 104-l+ Exon 11 (ins 13 bp) likely unstable due to frameshift and amino acid substitution at the carboxy terminal. The deletion of a single nucleotide (G) between nucleotides 1301 and 1305 (CGGGGGC + CGGGGC) in exon 10 of patient CR. which was also found in genomic DNA, resulted in frameshift, premature termination at codon 444, and either reduced transcription or unstable mRNA (Fig 2, lane 12). DISCUSSION To explore whether all WAS patients, irrespective of the clinical phenotype, have mutations of the WAS gene, we selected for mutation analysis 13 unrelated patients with clinical and laboratory findings that ranged from isolated platelet anomalies, characteristic for XLT, to the classic WAS phenotype. Using the dideoxy fingerprinting method for rapid screening, followed by sequence analysis of both cDNA and genomic DNA, we were able to identify mutations of the WAS gene in 9 boys with classic WAS and in4 with thrombocytopenia and small platelets. The most common mutations observed were point mutations of genomic DNA that resulted in either amino acid substitutions, the generation of termination codons, or the insertion or deletion of segments of cDNA. Only 3 of the 12 mutations identified were due to mutations other than single point mutations of genomic DNA. These mutations include insertions and deletions of single or multiple base pairs resulting in frameshift and amino acid substitutions followed by early termination. - Fig 5. Sequence analysis of cDNA end genomic DNA of patient PP shows an insertion of 13 bp in patient pp,s cDNA ,Al. This derived from intron 10, was due to a complex rearrangement including a deletion and insertion affecting intron 10 (B and Cl. Of the 18 unique mutations of the WAS gene reported to dateI3.l9(Fig l), 3 affected arginine 86, suggesting that codon 86 may be a mutation hot spot. Substitution of arginine with cysteine (2 patients reported here) resulted in a mild phenotype; substitution with leucine or with histidine" resulted in a classic phenotype. A simple scoring system to assess disease severity was designed to clearly identify patients with a mild phenotype resembling XLT. Three of the four unrelated XLT patients included in the analysis were found to have point mutations resulting in amino acid substitutions within exon 2 (Arg86Cys in 2 patients and Ala47Asp in 1 patient). The fourth patient with XLT had a point mutation within exon 9, resulting in the creation of a new splice site. This new splice site caused the deletion of 13 nucleotides and resulted in frameshift and the formation of a truncated and most likely unstable protein. It is possible that the circulating lymphocytes of the affected members of this family express two populations of mRNA: one having the deletion and the other a less detritmental missense mutation, Met307Val. Villa et all9 recently reported three unique mutations of the WAS gene in 3 unrelated boys with thrombocytopenia and small size platelets. Two of their patients had missense mutations within exon 2 and exon 7, respectively. The third mutation reported was more complex, consisting of a single nucleotide insertion, which resulted in frameshift and termination in exon 5 . At this time, without knowing the function of the WAS protein, it is difficult to understand why mutations From www.bloodjournal.org by guest on June 14, 2017. For personal use only. 3803 WASPGENE MUTATIONS IN WAS ANDX-THROMBOCYTOPENIA resulting in truncated proteins can lead to a mild phenotype affecting only platelets. Of the 9 patients with classic WAS phenotypes (score 3 to 5), only 1 had a simple missense mutation. Of the remaining 8 patients, 2 had nonsense mutations affecting exons 1 and 10, respectively, and 6 had complex mutations resulting in deletions or insertions, frameshift, and early termination. Sequence analysis of R " s genomic DNA showed a C + T transition at nucleotide 329, introducing a nonsense codon. However, the RT-PCR product consisted of two cDNA populations: one was of normal size and contained the termination codon and the other was shorter in size due to a deletion of 87 nucleotides. This deletion was found to represent the 5' section of the exon described as exon 3 in our original r e p ~ r t . 'Reexamination ~ of this region showed that this exon was divided by a 100-nucleotide-long intron into two exons: the 87-nucleotide-long exon 3 and the 102nucleotide-long exon 4 (see erratum to Deny et al,13 and Ochs et all4). Sequence analysis of the exodintron junctions surrounding the deleted exon failed to identify alternative splice sites that could account for the skipping of exon 3. Thus, the nonsense mutation at position 329 must be responsible for the deletion of exon 3 in the majority of the gene transcripts. Skipping of exons containing nonsense mutations has been observed in the fibrillin gene FBNl, which is responsible for Marfan's syndrome"; in the cystic fibrosis gene"; and in the gene involved in the complementation group C of Fanconi anemia:* suggesting that nonsense mutations may alter the selection or the effectiveness of regional splice site^.'^,^^ The reduced amount of mRNA found in this patient's B-LCL, suggesting insufficient transcription or unstable mRNA, shows that the resulting protein is not only truncated but also diminished, which is compatible with a severe clinical phenotype. Exodintron splice junction mutations were observed in two unrelated families. Although both of these mutations were t + c transitions at position+2 of the 5' splice site of intron 9 and 11, respectively, the consequences on transcription were different, depending which intron was affected. The t + c transition 5' of intron 9 resulted in the activation of an alternative splice site, the inframe addition of 114 nucleotides derived from intron 9, the generation of a termination codon within the inserted segment and a severely diminished transcript. The t + c transition 5' of intron 11 resulted in the skipping of exon 11, the loss of 115 nucleotides, an out of frame transcript, a truncated protein, and a normal amount of transcript. For 5' splice sites, the generation of an alternative splice site is dependent on the presence of such a site in the vicinity of the mutation site and on a certain degree of homology between the sequences of the old and the new splice sitesm In both patients, the consensus sequence at the exodintron junction, Ggtgag, was mutated to Ggcgag. In patient MB, a cryptic splice site, located 114 bp 3', with the sequence TGgtcag, was available, whereas in patient BM, no such cryptic splice site existed, and, as a consequence, exon 11 is skipped. The tools are now available to identify mutations within the WAS gene, to confirm the diagnosis in patients with atypical phenotypes, to recognize carrier females, and to perform prenatal diagnosis. However, despite cloning the WAS gene and progress in identifying unique mutations, little is known about the function of the WAS protein and its role in the normal development of T and B lymphocytes and the production of platelets. Analysis of the effect of naturally occurring mutations of the WAS gene on cell function should provide new insights into the regulation of the immune response and platelet homeostasis. REFERENCES 1. Wiskott A: Familitirer, angeborener Morbus Werlhofii? Monatsschr Kinderheilkd 68:212, 1937 2. Aldrich, RA, Steinberg AG, Campbell DC: Pedigree demonstrating a sex-linked recessive condition characterized by draining ears, eczematoid dermatitis and bloody diarrhea. Pediatrics 13:133, 1954 3. Cooper MD, Chase HP, Lowman JT, Krivit W, Good RA: Wiskott-Aldrich syndrome: An immunologic deficiency disease involving the afferent limb of immunity. Am J Med 44:499, 1968 4. Sullivan KE, Mullen CA, Blaese RM, Winkelstein JA: A multiinstitutional survey of the Wiskott-Aldrich syndrome. J Pediatr 125:876, 1994 5. Ochs HD, Slichter SJ, Harker LA, Von Behrens WE, Clark RA, Wedgwood W:The Wiskott-Aldrich syndrome: studies of lymphocytes, granulocytes, and platelets. Blood 55:243, 1980 6. Canales L, Mauer AM: Sex-linked hereditary thrombocytopenia as a variant of Wiskott-Aldrich syndrome. N Engl JMed 277:899, 1967 7. Chiaro JJ, Dharmkrong-at A, Bloom GE: X-linked thrombocytopenic purpura. I. Clinical and genetic studies of a kindred. Am J Dis Child 123:565, 1972 8. Stormorken H, Hellum B, Egeland T, Abrahamsen TG,Hovig T X-linked thrombocytopenia and thrombocytopathia: Attenuated Wiskott-Aldrich syndrome. Thromb Haemost 65:300, 1991 9. Donnir M, Schwartz M, Carlsson KU, Holmberg L: Hereditary X-linked thrombocytopenia maps to the same chromosomal region as the Wiskott-Aldrich syndrome. Blood 72:1849, 1988 10. Notarangelo LD, Parolini 0, Faustini R, Porteri V, Albertini A, Ugazio AG: Presentation of Wiskott-Aldrich syndrome as isolated thrombocytopenia. Blood 77: 1125, 1991 (letter) 11. Puck JM, Siminovitch KA, Poncz M, Greenberg CR, Rottem M, Conley M E : Atypical presentation of Wiskott-Aldrich syndrome: Diagnosis in two unrelated males based on studies of maternal T cell X chromosome inactivation. Blood 75:2369, 1990 12.De Saint-Bade G, Schlegel N, Caniglia M, Le Deist F, Kaplan C, Lecompte T, Piller F, Fischer A, Griscelli C: X-linked thrombocytopenia and Wiskott-Aldrich syndrome: Similar regional assignment but distinct X-inactivation pattern in carriers. Ann Hemato1 63:107, 1991 13. Deny JMJ, Ochs HD, Francke U: Isolation of a novel gene mutated in Wiskott-Aldrich syndrome. Cell 78:635, 1994 (erratum Cell 79: 1994) 14. Ochs HD, Deny JMJ, Zhu Q, Blaese RM, Francke U: The Wiskott-Aldrich gene, in Caragol I, EspaiiolT, Fontan G, Matamoros N (eds): Progress in Immune Deficiency V. Barcelona, Spain, Springer-Verlag Ibirica, 1995, p 32 15. Levitt D, Ochs HD, Wedgwood RJ: Epstein-Barr virus-induced lymphoblastoid cell lines derived from the peripheral blood of patients with X-linked agammaglobulinemia can secrete IgM. J Clin Immunol 4:143, 1984 16. Zhu Q, Zhang M, Rawlings DJ, Vihinen M, Hagemann T, Saffran DC, Kwan S-P, Nilsson L, Smith CIE, Witte ON, Chen S-H, Ochs HD: Deletion within the Src homology domain 3of From www.bloodjournal.org by guest on June 14, 2017. For personal use only. 3804 Bruton’s tyrosine kinase resulting in X-linked agammaglobulinemia (XLA). J Exp Med 180:461, 1994 17. Sarkar G, Yoon H-S, Sommer SS: Dideoxy fingerprinting (ddF): A rapid and efficient screen for the presence of mutations. Genomics 13:441, 1992 18. Sanger F, Nicklen S, Coulson AR:DNA sequencing with chain-terminating inhibitors. Proc Natl Acad Sci USA 74:5463, 1977 19. Villa A, Notarangelo L, Macchi P, Mantuano E, Cavagni G, Brugnoni D, Strina D, Patrosso MC, Ramenghi U, Sacco MG, Ugazio A, Vezzoni P: X-linked thrombocytopenia and Wiskott-Aldrich syndrome are allelic diseases with mutations in the WASP gene. Nat Genet 9:414, 1995 20. Dietz HC, Valle D, Francomano CA, Kendzior RJ Jr, Pyeritz ZHU ET AL RE, Cutting GR: The skipping of constitutive exons in vivo induced by nonsense mutations. Science 259:680, 1993 21. Hull J, Shackleton S, Harris A: The stop mutation R553X in the C R R gene results in exon slupping. Genomics 19:362, 1994 22. Gibson RA, Hajianpour A, Murer-Orlando M, Buchwald M, Mathew CG: A nonsense mutation and exon skipping in the Fanconi anaemia group C gene. Hum Mol Genet 2:797, 1993 23. Belgrader P, Maquat LE: Nonsense but not missense mutations can decrease the abundance of nuclear mRNA for the mouse major urinary protein, while both types of mutations can facilitate exon skipping. Mol Cell Biol 14:6326, 1994 24. Cooper DN, Krawczak M: Single basepair substitution, in Cooper DN, Krawczak M (eds): Human Gene Mutation. Oxford, UK, Bios Scientific Publishers, 1993, p 109 and 257 From www.bloodjournal.org by guest on June 14, 2017. For personal use only. 1995 86: 3797-3804 The Wiskott-Aldrich syndrome and X-linked congenital thrombocytopenia are caused by mutations of the same gene Q Zhu, M Zhang, RM Blaese, JM Derry, A Junker, U Francke, SH Chen and HD Ochs Updated information and services can be found at: http://www.bloodjournal.org/content/86/10/3797.full.html Articles on similar topics can be found in the following Blood collections Information about reproducing this article in parts or in its entirety may be found online at: http://www.bloodjournal.org/site/misc/rights.xhtml#repub_requests Information about ordering reprints may be found online at: http://www.bloodjournal.org/site/misc/rights.xhtml#reprints Information about subscriptions and ASH membership may be found online at: http://www.bloodjournal.org/site/subscriptions/index.xhtml Blood (print ISSN 0006-4971, online ISSN 1528-0020), is published weekly by the American Society of Hematology, 2021 L St, NW, Suite 900, Washington DC 20036. Copyright 2011 by The American Society of Hematology; all rights reserved.