Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Bioidentical hormone replacement therapy wikipedia , lookup
Hormonal breast enhancement wikipedia , lookup
Hypothyroidism wikipedia , lookup
Hormone replacement therapy (menopause) wikipedia , lookup
Graves' disease wikipedia , lookup
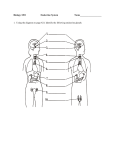
Hyperandrogenism wikipedia , lookup
Hormone replacement therapy (male-to-female) wikipedia , lookup
Hyperthyroidism wikipedia , lookup
Hypothalamus wikipedia , lookup
Neuroendocrine tumor wikipedia , lookup
Growth hormone therapy wikipedia , lookup
NAME_______________________ DATE COMPLETED__________ Endocrine Physiology Case Study -- Bathsheba Background A few years ago when I was teaching endocrine physiology to biology majors here at USD one of the students came up to me with her case as example of how the endocrine system works. Subsequently she came and talked with me about her life and the consequences of the situation that she developed as a young child. Situation At age 12, I appeared to be a normal healthy child. In May of 1997, at my yearly physical, my family doctor noticed that the chart representing my growth was quite unusual. In fact, it showed no growth, in regards to height and weight, in the last sixteen months. The doctor also noted that unlike my classmates, I did not exhibit any signs of pre-puberty or puberty. These symptoms cued him to perform several blood tests. An IGF-1 (evaluates pituitary gland function), free T4 & TI3 (thyroid hormone levels), and a blood estrogen level were all taken. The IGF-1 level came back as 0.21 m-IU/L (normal range 0.5 – 5.0 m-IU/L). This dramatically low test result alone could indicate endocrine trouble, but coupled with the free T4 level of 0.3 (normal range 0.8-1.9) is indicative of major loss of pituitary function. Upon seeing these results, my doctor referred me to a pediatric endocrinologist who ordered repeat series on all the blood tests and found them to be even lower than previously recorded. This prompted him to order a cranial MRI with contrast to look at the pituitary gland. In doing the scan, he hoped to rule out several possibilities. At that point, the possibilities ranged from simple lack of endocrine function not based on anatomy to pituitary deformity to a tumor, be it benign or malignant. A stage four tumor essentially encapsulating the pituitary gland was found. 1. How could this condition affect growth and development in Bathsheba? YOU HAVE JUST COMPLETED THIS CASE STUDY! NAME_______________________ DATE COMPLETED__________ The medical staff needed to determine whether the hypopituitaryism was malignant or benign. The doctor entered the skull through a small hole in the right parietal lobe to take a biopsy of the tumor through a two and a half inch incision. The frozen sections were examined in pathology and the tumor was identified as CNS Germinoma (very uncommon accounting for about 0.052% of cancers), and normally such tumors arise in the gonads or ovaries. Germ cell tumors, by definition, arise while in-utero, so this tumor in theory had had twelve years to grow. In surgery, it was discovered that the tumor was inoperable, taking that treatment option away. Other therapies would have to be used quickly so high dose chemotherapy was chosen. After six cycles of chemotherapy over the five months, the chemotherapy drugs not only did a fantastic job at destroying the cancer, but they were devastating to my immune system. I was given eighteen blood transfusions throughout. While radiating the remainder of the tumor, they “accidentally” radiated my pituitary and thyroid glands as well, turning them into (as the doctor put it) raisins. However, all of the therapy resulted in complete remission of the cancer. 2. What would Bathsheba’s hypothyroidism do to her? How could she be treated for low thyroid hormone? 3. What would Bathsheba’s hypocortisolism do to her? Would it be dangerous for Bathsheba to be stressed? YOU HAVE JUST COMPLETED THIS CASE STUDY! NAME_______________________ DATE COMPLETED__________ 4. Is it possible to help Bathsheba grow more normally and go into puberty? How would one do that? 5. If Bathsheba were your patient, what would you advise her about getting pregnant and nursing an infant? 6. If artificial hormones were not available to Bathsheba, what would be her levels of hypothalamic hormones? If too many artificial hormones were given to Bathsheba, what would be her levels of hypothalamic hormones? YOU HAVE JUST COMPLETED THIS CASE STUDY! NAME_______________________ DATE COMPLETED__________ 7. Which hormones would Bathsheba be able to stop taking as she matures? Don’t forget to add the posterior pituitary hormones vasopressin and oxytocin. Hypothalamic Pituitary Axis Image A version may be found in Silverthorn, Figure 7.9 from Human Physiology: An Integrated Approach, sixth edition, from Pearson, copyright 2013. You have completed the exercise! Please submit answers only, typed on a new sheet. Thank you! Special thanks to Bathsheba for sharing her story with future physiology students. YOU HAVE JUST COMPLETED THIS CASE STUDY! APPENDIX: MEDICAL BACKGROUND FOR BATHSHEBA At age 12, I appeared to be a normal healthy child. In May of 1997, at my yearly physical, my family doctor noticed that the chart representing my growth was quite unusual. In fact, it showed no growth, in regards to height and weight, in the last sixteen months. The doctor was, of course, bothered by this. He also noted that unlike my classmates, I did not exhibit any signs of pre-puberty nor puberty. These symptoms cued him to perform several blood tests. An IGF-1 (evaluates pituitary gland function), Free T4 & T3 (thyroid hormone levels), and a blood estrogen level were all taken. The IGF-1 level came back as 0.21 m-IU/L (normal range 0.5 – 5.0 m-IU/L). This dramatically low test result alone could indicate endocrine trouble, but coupled with the Free T4 level of 0.3 (normal range 0.81.9) is indicative of major loss of pituitary function. Upon seeing these results, the doctor realized that he, as a general family physician, was way over his head. He referred me to a Pediatric Endocrinologist who happened to be running a clinic in my hometown within the next month. The endocrinologist was duly concerned with the blood tests. He ordered a repeat series on all and found them to be even lower than previously recorded. This prompted him to order a cranial MRI with contrast to get a look at the pituitary gland. In doing the scan, he hoped to rule out several possibilities. At that point, the possibilities ranged from simple lack of endocrine function not based on anatomy to pituitary deformity to a tumor, be it benign or malignant. The scan was done immediately and revealed what we had feared. A stage four tumor extending from the sella turcica to the third ventricle (which is bound by the thalamus, the hypothalamus, and the lamina terminalis) was discovered. The tumor had essentially encapsulated my pituitary gland, explaining the lack of growth. Now that the hypopituitaryism was no longer idiopathic, we had to determine if the tumor was malignant or benign. An acclaimed neurosurgeon was called immediately and flew to Sioux Falls from Minneapolis as I was transported to the hospital in Sioux Falls. After being checked in and completing a creatine clearance, I was sedated. For the next five hours, a steriotactic biopsy was performed. The doctor entered the skull through the right parietal lobe, as it allowed the least invasive sampling of the tumor, through a two and a half inch incision. Three frozen sections from the biopsy were examined in pathology and the tumor was identified as CNS Germinoma. Germinoma is a type of cancer that is uncommon unto itself (accounting for only about 0.052% of cancers), but normally such tumors arise in the gonads or ovaries. Germ cell tumors, by definition, arise while in-utero, so this tumor in theory had twelve years to grow. In surgery, it was discovered that the tumor was inoperable, taking that treatment option away. Other therapies would have to be used, and quickly. Luckily, a specialist on brain germinomas who happened to be working at the Sioux Falls hospital was called in. After discussing our options on how to quickly destroy the tumor, high dose chemotherapy was decided upon. I underwent six cycles of chemotherapy over the next five months. Cisplatinin and VP-16 were the chemo drugs administered intravenously in the first three chemotherapy sessions. While doing a fantastic job at destroying the cancer, they were devastating to my immune system. I was given eighteen blood transfusions throughout. The time pattern for therapy was: one week of chemo, three weeks off, one week of chemo, three weeks off, etc. Because of how harsh the therapies were and because we had already reduced the tumor to 30% of its original size by the third round of chemo, Carboplatnin (an experimental drug at the time) replaced Cisplatinin in my cocktail for the last three sessions. A month was taken off to allow my body to reboot and restore blood counts. After this, thirty cycles of radiation therapy and brain boost radiation were administered at the University of Minnesota Hospital in St. Paul. While radiating the remainder of the tumor, they “accidentally” radiated my pituitary and thyroid glands as well, turning them into (as the doctor put it) raisins. However, all of the therapy resulted in complete remission of the cancer. The aftermath of cancer and therapy is: hypopituitaryism, hypothyroidism, diabetes insipidus, and a menopause like state of estrogen levels. Hormone replacement had to wait for about two years because of the chance of recurrence. (It’s not a good idea to provide a tumor with hormones.) When the time came to begin hormone replacement, I was a sixteen-year-old in the body of a twelve-year-old. Anti-diuretic hormone replacement had begun just after finishing radiation therapy, as it didn’t pose a tumor boosting danger. Thyroid hormone replacement and growth hormone injections were next to come. Synthroid was the thyroid hormone replacement and Nutropin AQ was the growth hormone of choice because it provided the highest amount of raw growth hormone without added testosterones or estrogens, both of which would age my growth plates minimizing the growth we could achieve. This bone aging is also the reason that estrogen therapy wasn’t begun for another year following the HGH and thyroid replacement. When the time came, we began with estrogens similar to what a woman would produce during her non-menstruating weeks. These were given for fourteen months prior to putting me on cycling hormones. The results of all this exciting therapy were: fourteen inches of height increase, and puberty! Thank you artificial endocrine hormones!