Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Vectors in gene therapy wikipedia , lookup
Neuronal ceroid lipofuscinosis wikipedia , lookup
Epigenetics of neurodegenerative diseases wikipedia , lookup
Site-specific recombinase technology wikipedia , lookup
Designer baby wikipedia , lookup
Polycomb Group Proteins and Cancer wikipedia , lookup
Nutriepigenomics wikipedia , lookup
Artificial gene synthesis wikipedia , lookup
Gene expression profiling wikipedia , lookup
Oncogenomics wikipedia , lookup
Gene therapy wikipedia , lookup
Therapeutic gene modulation wikipedia , lookup
Epigenetics of diabetes Type 2 wikipedia , lookup
Gene therapy of the human retina wikipedia , lookup
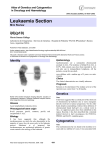
From www.bloodjournal.org by guest on June 14, 2017. For personal use only. Brief report p16INK4a immunocytochemical analysis is an independent prognostic factor in childhood acute lymphoblastic leukemia Jean Hughes Dalle, Martine Fournier, Brigitte Nelken, Françoise Mazingue, Jean-Luc Laı̈, Francis Bauters, Pierre Fenaux, and Bruno Quesnel We investigated the prognostic value of p16INK4a immunocytochemistry (ICC) analysis in 126 cases of newly diagnosed childhood acute lymphoblastic leukemia (ALL). The incidence of negative p16INK4a ICC was 38.1% and was more frequent in T-lineage ALL. Overall survival (OS) and event-free survival (EFS) were significantly higher in patients with positive p16INK4a ICC than in patients with negative ICC (6 years OS, 90% versus 63%, P ⴝ .0014; 6 years EFS, 77.8% versus 55%, P ⴝ .0033). The p16INK4a ICC remained a significant prognostic factor within the subgroup of B-precursor ALL. Multivariate analysis showed that negative p16INK4a ICC was an independent prognostic factor for OS (relative risk [RR], 3.38; P ⴝ .02) and EFS (RR, 2.49; P ⴝ .018). Sequential study showed that p16INK4a expression remained stable during first relapse in most patients. These findings indicate that p16INK4a ICC is an independent factor of outcome in childhood ALL. (Blood. 2002;99:2620-2623) © 2002 by The American Society of Hematology Introduction The p15INK4b and p16INK4a proteins are cell-cycle regulators involved in the inhibition of G1 phase progression. The p16INK4a and p15INK4b genes are homozygously deleted in many tumor types, including childhood acute lymphoblastic leukemia (ALL), but p16INK4a expression in leukemic cells may vary in the absence of gene deletion or point mutation.1-12 We recently reported the results of p16INK4a protein analysis by immunocytochemistry (ICC) in a limited cohort of adult ALL patients.13 The technique of p16INK4a ICC requires only bone marrow or blood smears; many samples can be processed in the same day, and this technique allows direct identification of leukemic cells, leading to an easier interpretation. We observed that negative p16INK4a ICC conferred an adverse outcome in adult ALL with standard-risk karyotype, but the small number of samples did not allow us to perform multivariate analysis. The low rate of high-risk karyotypic abnormalities in childhood ALL allowed us to expect a specific prognostic value of p16INK4a ICC in childhood ALL. In a large, homogenously treated cohort of childhood ALL patients, we investigated the influence of negative p16INK4a ICC on overall survival (OS) and event-free survival (EFS) in univariate and multivariate analysis. Additionally, we sequentially investigated p16INK4a ICC in a cohort of those patients at relapse. (range, 0.5-15). There were 73 males and 53 females. Of these patients, 80 were treated according to the European Organization for Research and Treatment of Cancer (EORTC) protocol 58881 between 1991 and December 1998, and 46 were treated by EORTC protocol 58951 between January 1998 and December 2000.14 The median observation time for all patients was 4.8 years (range, 1.4-9.2 years). There were 31 other patients studied by p16INK4a ICC in first relapse. Among them, 20 were also studied sequentially (14 at diagnosis and first relapse, 6 in first and second or third relapse). Immunocytochemical detection of p16INK4a protein was performed with the immunoglobulin G1- mouse monoclonal antibody antihuman p16INK4a (clone DCS-50.1/H4) (Oncogene Research Products, Cambridge, United Kingdom), as previously described.13 The ICC reaction was performed with avidin-biotinperoxidase technique by means of Vector reagents (Vector Laboratories, Burlingame, CA). Positive cells appeared with brownish granules. Samples were considered ICC-positive when more than 5% of cells showed p16INK4a protein, according to our previous study in adult ALL.13 The chi-square and Fisher exact test were used for comparison between initial parameters. OS and EFS were estimated according to the KaplanMeier method. Events were defined as induction death, relapse, and death in complete remission (CR). Multivariate analysis was based on the Cox proportional hazards regression model. Statistical analyses were performed on SPSS 9.1 analysis software (SPSS, Chicago, IL). Results and discussion Study design We analyzed p16INK4a gene expression by p16INK4a ICC in 126 childhood ALLs (89 B-precursor ALLs, 28 T-ALLs, and 9 acute undifferentiated leukemias). Patient bone marrow (n ⫽ 87) or blood (n ⫽ 39) smears were collected from May 1992 to December 2000. Median age was 4.9 years From Service des Maladies du Sang, Centre Hospitalier et Universitaire Lille; 2-Service d’Hématologie Pédiatrique, Centre Hospitalier et Universitaire Lille; Laboratoire d’Hématologie, Centre Hospitalier et Universitaire Lille; Laboratoire de Cytogénétique, Centre Hospitalier et Universitaire Lille; Unité INSERM 524, Institut de Recherche sur le Cancer de Lille, Lille, France. Submitted August 31, 2001; accepted November 30, 2001. Supported by the Ligue Contre le Cancer (Comité du Nord and Comité du Pas de Calais). 2620 As previously observed in adult ALL, a great variation in the percentage of p16INK4a ICC-positive cells was seen (median, 20%; range, 0-100).13 We found 51 samples (38.1%) to be p16INK4a ICC–negative. All patients achieved CR. No difference for sex, white blood cell count, presence of a bulky mass, central nervous system disease, hemoglobin level, chromosome 9p abnormalities, J.H.D. and M.F. contributed equally to this work as first authors. Reprints: Bruno Quesnel, Service des Maladies du Sang, CHU Lille, 1 Place de Verdun, 59037, Lille, France; e-mail: [email protected]. The publication costs of this article were defrayed in part by page charge payment. Therefore, and solely to indicate this fact, this article is hereby marked ‘‘advertisement’’ in accordance with 18 U.S.C. section 1734. © 2002 by The American Society of Hematology BLOOD, 1 APRIL 2002 䡠 VOLUME 99, NUMBER 7 From www.bloodjournal.org by guest on June 14, 2017. For personal use only. BLOOD, 1 APRIL 2002 䡠 VOLUME 99, NUMBER 7 p16INK4a IS AN INDEPENDENT FACTOR IN CHILDHOOD ALL 2621 were negative p16INK4a ICC ALL patients, but significance (P ⫽ .046) disappeared after stratification by phenotype (P ⫽ .205). Increased sensitivity threshold for glucocorticoid-induced apoptosis induced by forced p16INKa expression in lymphoblastic leukemia cell line has been reported.15 However, we did not find significant association in our cohort of childhood ALL patients between p16INK4a ICC status and prednisone response at day 8 (P ⫽ .434). Hence, it remains unclear whether p16INK4a expression influences in vivo glucocorticoid-induced apoptosis of ALL cells. Univariate analysis showed significantly better OS and EFS in patients with positive p16INK4a ICC at diagnosis (Figure 1). OS estimates at 6 years for patients with or without positive p16INK4a ICC at diagnosis were 90% (SE ⫽ 3.8%) and 63% (SE ⫽ 8.7%), respectively (P ⫽ .0014, log-rank test). EFS estimates at 6 years were 78% (SE ⫽ 5.8%) and 54% (SE ⫽ 8.4%) for p16INK4a ICC–positive and p16INK4a ICC–negative subgroups, respectively (P ⫽ .0033, log-rank test). When cutoff values of 0% and 10%, rather than 5%, for negative versus positive p16INK4a ICC were used, results were less significant. These findings indicate that, as in our previous analysis in adult ALL, 5% is a valid cutoff value for prognostic studies in ALL.13 Despite the association between negative ICC and T phenotype at diagnosis, p16INK4a ICC remained a significant prognostic factor in the subgroup of B-precursor ALLs for both OS (P ⫽ .0044) and EFS (P ⫽ .011) (Figure 1). This was not the case for T-ALL (OS, P ⫽ .23; EFS, P ⫽ .19). Final models of multivariate analysis showed that p16INK4a ICC remained an independent prognostic factor for both OS (P ⫽ .02) and EFS (P ⫽ .0188) in the whole cohort (Table 1). However, karyotype remained the main prognostic factor for OS (relative risk ⫽ 3.92 versus 3.38). Incorporation of immunophenotype into the model did not Table 1. Multivariate Cox model analysis for overall and event-free survival of the 126 childhood acute lymphoblastic leukemia patients Univariate analysis P Variable Multivariate analysis P RR 95% CI OS p16INK4aICC* .0014 .0204 3.38 1.20-9.48 Karyotype† .0032 .0227 3.92 1.21-12.72 Age‡ .0165 .12 2.30 0.81-6.61 WBC§ .0425 .0719 2.55 0.92-7.09 Prednisone response day 8㛳 .069 — — — Hemoglobin¶ .964 — — — Bulky tumor mass .27 — — — Immunophenotype# .25 — — — Sex .8425 — — — p16INK4aICC* .0033 .0188 2.49 1.16-5.32 Karyotype† .0609 — — — Age‡ .0374 .0735 2.06 0.93-4.55 WBC§ .297 — — — Prednisone response day 8㛳 .4 — — — Hemoglobin¶ .73 — — — Bulky tumor mass .77 — — — Immunophenotype# .28 — — — Sex .52 — — — EFS Figure 1. Survival of childhood ALL patients according to their p16INK4a ICC status. OS (panel A) and EFS (panel B) of the 126 childhood ALL patients. OS (panel C) and EFS (panel D) of childhood B-precursor ALL patients according to their p16INK4a ICC status. or karyotype could be observed between p16INK4a ICC–positive and p16INK4a ICC–negative cases. However, positive p16INK4a ICC was found significantly more frequently in B-precursor ALL (70.7%) than in T-ALL (43%) (P ⫽ .006). Positive p16INK4a ICC ALL patients were also more likely to be older than age 9 years than RR indicates relative risk; CI, confidence interval; OS, event-free survival; ICC, immunocytochemistry; WBC, white blood count; EFS, event-free survival. *Greater than 5% acute lymphoblastic leukemia cells; 5% or fewer acute lymphoblastic leukemia cells. †High risk, including t(9; 22), t(4; 11), t(1; 19) and hypodiploid; intermediate and low risk. ‡Younger than 1 and older than 9 years; 1 year or older and 9 years or younger. §Lower than 50 000/L; 50 000/L or higher. 㛳Circulating blasts at 1000/L or more; fewer than 1000/L circulating blasts. ¶More than 11 g/dL; lower than 11 g/dL. #T-acute lymphoblastic leukemia; B-precursor acute lymphoblastic leukemia. From www.bloodjournal.org by guest on June 14, 2017. For personal use only. 2622 BLOOD, 1 APRIL 2002 䡠 VOLUME 99, NUMBER 7 DALLE et al modify the results. It has been suggested in previous studies that the significance of p16INK4a gene deletions would disappear within the subgroups of T-ALL and B-precursor ALL.16,17 Our data show that T phenotype does not account for the poorer outcome of p16INK4a ICC–negative patients. However, the results of gene deletion studies and protein expression analyses by ICC may differ. Indeed, several studies have shown that p16INK4a protein expression in leukemic cells is a complex phenomenon and can be altered not only by gene deletion but also by promoter methylation and other, unknown mechanisms.18-21 We also observed, both in adult ALL and in the present pediatric study, that a few samples of leukemic cells with no detectable p16INK4a protein at diagnosis showed p16INK4a expression at relapse (Table 2, patient I120).13 These findings might explain why p16INK4a ICC provides prognostic information distinct from that derived through p16INK4a gene deletion analysis. The lower proportion of high-risk karyotypes such as t(9;22)(q34;q11) in children may explain why p16INK4a ICC has a specific prognostic value in childhood ALL as compared with adult ALL. Of the children with ALL analyzed at first relapse, 11 (35.5%) showed negative p16INK4a ICC (Table 2). Previous studies had shown that p16INK4a gene deletion could be acquired during evolution of the disease, but these findings have not been observed by other groups.3,5,16,22-24 In our study, ICC status became negative between diagnosis and first relapse in one patient (I119), and between first and second relapse in two others (I102, I103). Substantial variations of the percentage of p16INK4a-positive cells were also observed in 5 patients, suggesting that p16INK4a expression varies widely among both patients and varieties of disease progression. Thus, p16INK4a ICC should be tested when drugs targeting p16INK4a protein are tested.20 These findings indicate that absence of p16INK4a expression is an early phenomenon in the evolution of ALL. Some patients may lose p16INK4a expression during further relapse, but the impact of p16INK4a inactivation in those leukemic cells, which probably have accumulated numerous other gene alterations, remains to be determined. Thus, the simple and reproducible p16INK4a ICC method should provide important prognostic information in large-scale prospective therapeutic studies. Table 2. Sequential analysis of p16INK4a immunocytochemistry in patients with acute lymphoblastic leukemia Positive leukemic cells by p16INK4a ICC, % Patient no. Immunophenotype Diagnosis First relapse Second relapse Third relapse I101 B ND 80 95 100 I102 B ND 90 0 — I103 B ND 100 0 — I104 B 70 100 — — I105 B 100 25 — — I106 AUL 3 2 — — I107 T 0 1 0 0 I108 B ND 100 ND 100 I109 T 75 40 I110 B 2 2 — — I111 B 16 100 — — I112 B 95 20 — — I113 AUL 100 30 — — I114 T ND 2 0 — I115 B 1 1 ND — I116 B ND 1 0 — I117 B 100 70 — — I118 T 0 1 — — I119 B 80 1 0 — I120 B 16 — — I121 T ND 40 — — I122 B ND 35 — — I123 B ND 25 — — I124 B ND 50 — — I125 B ND 100 — — I125 AUL ND 100 — — I127 B ND 1 — — I128 B ND 2 — — I129 T ND 1 — — I130 B ND 35 — — I131 B ND 7 — — 2.5 — ICC indicates immunocytochemistry; AUL, acute undifferentiated leukemia; ND, not done. References 1. Quesnel B, Preudhomme C, Philippe N, et al. p16 gene homozygous deletions in acute lymphoblastic leukemia. Blood. 1995;85:657-663. 2. Iolascon A, Faienza MF, Coppola B, della Ragione F, Santoro N, Schettini F. High frequency of homozygous deletions of CDK4I gene in childhood acute lymphoblastic leukaemia. Br J Haematol. 1995;91:647-651. 3. Ohnishi H, Kawamura M, Ida K, et al. Homozygous deletions of p16/MTS1 gene are frequent but mutations are infrequent in childhood T-cell acute lymphoblastic leukemia. Blood. 1995;86: 1269-1275. 4. Takeuchi S, Bartram CR, Seriu T, et al. Analysis of a family of cyclin-dependent kinase inhibitors: p15/MTS2/INK4B, p16/MTS1/INK4A, and p18 genes in acute lymphoblastic leukemia of childhood. Blood. 1995;86:755-760. 5. Takeuchi S, Bartram CR, Wada M, et al. Allelotype analysis of childhood acute lymphoblastic leukemia. Cancer Res. 1995;55:53775382. 6. Zhou M, Gu L, James CD, et al. Homozygous deletions of the CDKN2 (MTS1/p16ink4) gene in cell lines established from children with acute lymphoblastic leukemia. Leukemia. 1995;9:11591161. 7. Iolascon A, Faienza MF, Coppola B, della Ragione F, Schettini F, Biondi A. Homozygous deletions of cyclin-dependent kinase inhibitor genes, p16(INK4A) and p18, in childhood T cell lineage acute lymphoblastic leukemias. Leukemia. 1996; 10:255-260. 8. Nakao M, Yokota S, Kaneko H, et al. Alterations of CDKN2 gene structure in childhood acute lymphoblastic leukemia: mutations of CDKN2 are observed preferentially in T lineage. Leukemia. 1996;10:249-254. 9. Ohnishi H, Hanada R, Horibe K, et al. Homozygous deletions of p16/MTS1 and p15/MTS2 genes are frequent in t(1;19)–negative but not in t(1;19)–positive B precursor acute lymphoblastic leukemia in childhood. Leukemia. 1996;10:11041110. 10. Pui CH. Acute leukemia in children. Curr Opin Hematol. 1996;3:249-258. 11. Kees UR, Burton PR, Lu C, Baker DL. Homozygous deletion of the p16/MTS1 gene in pediatric acute lymphoblastic leukemia is associated with unfavorable clinical outcome. Blood. 1997;89: 4161-4166. 12. Rubnitz JE, Behm FG, Pui CH, et al. Genetic studies of childhood acute lymphoblastic leukemia with emphasis on p16, MLL, and ETV6 gene abnormalities: results of St Jude Total Therapy Study XII. Leukemia. 1997;11:12011206. 13. Soenen V, Lepelley P, Gyan E, et al. Prognostic significance of p16INK4a immunocytochemistry in adult ALL with standard risk karyotype. Leukemia. 2001;15:1054-1059. 14. Vilmer E, Suciu S, Ferster A, et al. Long-term results of three randomized trials (58831, 58832, 58881) in childhood acute lymphoblastic leukemia: a CLCG-EORTC report. Children Leukemia Cooperative Group. Leukemia. 2000;14:22572266. 15. Ausserlechner MJ, Obexer P, Wiegers GJ, Hartmann BL, Geley S, Kofler R. The cell cycle inhibitor p16(INK4A) sensitizes lymphoblastic leukemia cells to apoptosis by physiologic glucocorticoid levels. J Biol Chem. 2001;276: 10984-10989. 16. Carter TL, Watt PM, Kumar R, et al. Hemizygous p16(INK4A) deletion in pediatric acute lymphoblastic leukemia predicts independent risk of relapse. Blood. 2001;97:572-574. 17. Graf Einsiedel H, Taube T, Hartmann R, et al. Prognostic value of p16(INK4a) gene deletions in pediatric acute lymphoblastic leukemia. Blood. 2001;97:4002-4004. From www.bloodjournal.org by guest on June 14, 2017. For personal use only. BLOOD, 1 APRIL 2002 䡠 VOLUME 99, NUMBER 7 18. Nakamura M, Sugita K, Inukai T, et al. p16/MTS1/ INK4A gene is frequently inactivated by hypermethylation in childhood acute lymphoblastic leukemia with 11q23 translocation. Leukemia. 1999; 13:884-890. 19. Wong IH, Ng MH, Huang DP, Lee JC. Aberrant p15 promoter methylation in adult and childhood acute leukemias of nearly all morphologic subtypes: potential prognostic implications. Blood. 2000;95:1942-1949. 20. Omura-Minamisawa M, Diccianni MB, Batova A, et al. In vitro sensitivity of T-cell lymphoblastic leukemia to UCN-01 (7-hydroxystaurosporine) is p16INK4a IS AN INDEPENDENT FACTOR IN CHILDHOOD ALL dependent on p16 protein status: a Pediatric Oncology Group study. Cancer Res. 2000;60:65736576. 21. Omura-Minamisawa M, Diccianni MB, Batova A, et al. Universal inactivation of both p16 and p15 but not downstream components is an essential event in the pathogenesis of T-cell acute lymphoblastic leukemia. Clin Cancer Res. 2000;6:12191228. 22. Ogawa S, Hangaishi A, Miyawaki S, et al. Loss of the cyclin-dependent kinase 4-inhibitor (p16; MTS1) gene is frequent in and highly specific to lymphoid tumors in primary human he- 2623 matopoietic malignancies. Blood. 1995;86: 1548-1556. 23. Maloney KW, McGavran L, Odom LF, Hunger SP. Acquisition of p16(INK4A) and p15(INK4B) gene abnormalities between initial diagnosis and relapse in children with acute lymphoblastic leukemia. Blood. 1999;93:2380-2385. 24. Carter TL, Reaman GH, Kees UR. INK4A/ARF deletions are acquired at relapse in childhood acute lymphoblastic leukaemia: a paired study on 25 patients using real-time polymerase chain reaction. Br J Haematol. 2001;113:323328. From www.bloodjournal.org by guest on June 14, 2017. For personal use only. 2002 99: 2620-2623 doi:10.1182/blood.V99.7.2620 p16INK4a immunocytochemical analysis is an independent prognostic factor in childhood acute lymphoblastic leukemia Jean Hughes Dalle, Martine Fournier, Brigitte Nelken, Françoise Mazingue, Jean-Luc Lai?, Francis Bauters, Pierre Fenaux and Bruno Quesnel Updated information and services can be found at: http://www.bloodjournal.org/content/99/7/2620.full.html Articles on similar topics can be found in the following Blood collections Brief Reports (1936 articles) Neoplasia (4182 articles) Oncogenes and Tumor Suppressors (795 articles) Information about reproducing this article in parts or in its entirety may be found online at: http://www.bloodjournal.org/site/misc/rights.xhtml#repub_requests Information about ordering reprints may be found online at: http://www.bloodjournal.org/site/misc/rights.xhtml#reprints Information about subscriptions and ASH membership may be found online at: http://www.bloodjournal.org/site/subscriptions/index.xhtml Blood (print ISSN 0006-4971, online ISSN 1528-0020), is published weekly by the American Society of Hematology, 2021 L St, NW, Suite 900, Washington DC 20036. Copyright 2011 by The American Society of Hematology; all rights reserved.