Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Prescription costs wikipedia , lookup
NMDA receptor wikipedia , lookup
Discovery and development of beta-blockers wikipedia , lookup
5-HT3 antagonist wikipedia , lookup
Pharmacogenomics wikipedia , lookup
Effect size wikipedia , lookup
Discovery and development of angiotensin receptor blockers wikipedia , lookup
Cannabinoid receptor antagonist wikipedia , lookup
Pharmacognosy wikipedia , lookup
Drug interaction wikipedia , lookup
NK1 receptor antagonist wikipedia , lookup
Neuropharmacology wikipedia , lookup
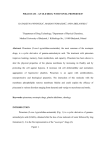
Pharmacological Reports 2006, 58, 680691 ISSN 1734-1140 Copyright © 2006 by Institute of Pharmacology Polish Academy of Sciences Vinpocetine and piracetam exert antinociceptive effect in visceral pain model in mice Omar M.E. Abdel Salam Department of Pharmacology, National Research Centre, Tahrir St., Dokki, Cairo, Egypt Correspondence: Omar M.E. Abdel Salam, e-mail: [email protected] Abstract: The effect of vinpocetine or piracetam on thermal and visceral pain was studied in mice. In the hot plate test, vinpocetine (0.9 and 1.8 mg/kg), but not piracetam, produced a reduction in nociceptive response. Vinpocetine (0.45–1.8 mg/kg, ip) or piracetam (75–300 mg/kg, ip) caused dose-dependent inhibition of the abdominal constrictions evoked by ip injection of acetic acid. The effect of vinpocetine or piracetam was markedly potentiated by co-administration of propranolol, guanethidine, atropine, naloxone, yohimbine or prazosin. The marked potentiation of antinociception occurred upon a co-administration of vinpocetine and baclofen (5 or 10 mg/kg). In contrast, piracetam antagonized antinociception caused by the low (5 mg/kg), but not the high (10 mg/kg) dose of baclofen. The antinociception caused by vinpocetine was reduced by sulpiride; while that of piracetam was enhanced by haloperidol or sulpiride. Either vinpocetine or piracetam enhanced antinociception caused by imipramine. The antinociceptive effects of vinpocetine or piracetam were blocked by prior administration of theophylline. Low doses of either vinpocetine or piracetam reduced immobility time in the Porsolt’s forced-swimming test. This study indicates that vinpocetine and piracetam possess visceral antinociceptive properties. This effect depends on activation of adenosine receptors. Piracetam in addition inhibits GABA-mediated antinociception. Key words: vinpocetine, piracetam, thermal pain, visceral pain, mice Introduction Piracetam, the first of the pyrrolidone derivatives (2-oxopyrrolidine), is a widely used drug in the treatment of cerebral stroke [20], dementia or cognitive impairment in the elderly [41], and myoclonus epilepsy [10]. The drug reverses hippocampal membrane alterations in Alzheimer’s disease [8]. Vinpocetine, a synthetic derivative of the alkaloid vincamine having antianoxic, antiischemic and neuroprotective properties, is frequently used in the therapy of cerebral disorders of vascular origin [11]. Although both drugs belong to distinct chemical classes, they share the name nootropic, the term introduced by Giurgea 680 Pharmacological Reports, 2006, 58, 680691 [16], to indicate this category of drugs that enhance memory, facilitate learning and protect memory processes against conditions which tend to disrupt them. Despite the fact that piracetam and vinpocetine have been used in clinical practice for around three decades, their precise mechanism of action within the brain remains largely unknown. Enhancement of oxidative glycolysis, anticholinergic effects, positive effects on the cerebral circulation, effects on membrane physics, and also reduction of platelet aggregation and improvement in erythrocyte function are likely to account for a cognition-enhancing effect and a neuroprotective effect of piracetam in stroke [36]. On the other hand, vinpocetine is a potent vasodilator at the cerebral vascular bed, increasing cerebral blood flow, Antinociception by vinpocetine and piracetam Omar M.R. Abdel Salam that increases the regional cerebral glucose uptake and, to a certain extent, glucose metabolism in the so-called peri-stroke region as well as in the relatively intact brain tissue [40]. Vinpocetine has been found to interfere with various stages of the ischemic cascade: adenosine triphosphate (ATP) depletion, activation of voltage-sensitive Na+- and Ca++-channels, glutamate and free radicals release [17]. Apart from their cognitive enhancing properties, both drugs are likely to possess other important pharmacological properties. Gastric protective effects have been described for vinpocetine [28], whereas piracetam has been suggested to exert anti-inflammatory properties [27]. Prolonged consumption of piracetam resulted in a 3-fold decrease in beta-endorphin concentration in plasma of rats [39], but its ip administration (100 mg/kg) inhibited gamma aminobutyric acid (GABAergic) antinociception caused by baclofen [13]. Nefiracetam, a new member of the piracetam group of cognition enhancers, reversed the thermal hyperalgesia observed in nerve-injured mice and the thermal hyperalgesia observed in streptozotocin-induced diabetic mice [33]. Vinpocetine is capable of blocking NaV1.8 sodium channel activity, which suggests a potential additional utility of the drug in various sensory abnormalities arising from abnormal peripheral nerve activity [44]. The above data suggest that these nootropic drugs are likely to modulate nociception and might prove useful in certain types of pain. In the light of the above and since the nootropic agents vinpocetine and piracetam are widely prescribed for the pharmacotherapy of memory and neurodegenerative disorders, it, therefore, looked pertinent to investigate and compare the pharmacological effects of piracetam and vinpocetine in two experimental pain models in mice: the acetic acid-induced writhing response, a model of visceral inflammatory pain (chemonociception), and the tailflick test, a model of supraspinal analgesia. Moreover, the effect of the two drugs on locomotor activity and their potential antidepressant effect were evaluated. Materials and Methods Animals Male albino Swiss mice 20–22 g of body weight were used. Standard laboratory food and water were pro- vided ad libitum. All experimental procedures were conducted in accordance with the guide for the care and use of laboratory animals and were reviewed by the Local Animal Care and Use Committee. The doses of vinpocetine or piracetam used in the study were based upon the human dose after conversion to that of rat [31]. Hot-plate assay The hot-plate test was performed by using an electronically controlled hot plate (Ugo Basile, Italy) heated to 52 ± 0.1°C). The cut-off time was 30 s. Groups of mice (n = 6/group) were given vinpocetine (0.45, 0.9 or 1.8 mg/kg, sc, 0.2 ml, n = 6/group) or piracetam (75, 150 or 300 mg/kg, sc, 0.2 ml) or saline (control), 30 min prior to testing. The experimenter was blind to the dose. Latency to lick a hind paw or jump out of the apparatus was recorded for the control and drug-treated groups. Abdominal constriction assay Separate groups of 6 mice each were given vinpocetine (0.45, 0.9 or 1.8 mg/kg, ip, 0.2 ml), piracetam (75, 150 or 300 mg/kg, ip, 0.2 ml), indomethacin (20 mg/kg, ip, 0.2 ml) or saline (0.2 ml, ip, control). Unless otherwise indicated in the text, drugs or saline were administered 30 min prior to an ip injection of 0.2 ml of 0.6% acetic acid [22]. Each mouse was then placed in an individual clear plastic observational chamber, and the total number of writhes experienced by each mouse was counted for 30 min after acetic acid administration by an observer who was not aware of the animals’ treatment. Afterwards, animals were sacrificed by CO2 exposure. Further experiments were designed in an attempt to elucidate the mechanisms by which vinpocetine or piracetam exerts its anti-nociceptive effect. The dose of 1.8 mg/kg of vinpocetine or 300 mg/kg of piracetam was then selected to be used in the subsequent experiments. Thus, we examined the effects of co-administration of the a-1 adrenoceptor antagonists prazosin (2 mg/kg, ip) and doxazosin (4 or 16 mg/kg, ip), a-2 adrenoceptor antagonist yohimbine (4 mg/kg, ip), b-adrenoceptor antagonist, propranolol (2 mg/kg, ip), muscarinic acetylcholine receptor antagonist atropine (2 mg/kg ip), non-selective opioid receptor antagonist naloxone (5 mg/kg ip), GABA agonist baclofen (5 or 10 mg/kg) Pharmacological Reports, 2006, 58, 680691 681 and ATP-gated potassium channel blocker glibenclamide (5 mg/kg, ip) on antinociception caused by vinpocetine or piracetam. Drugs were administered 30 min prior to the abdominal constriction assay. The effect of adrenergic neuron blockade with guanethidine (16 mg/kg, ip) co-administered with either vinpocetine or piracetam was also investigated. The abdominal constriction assay was carried out 30 min after the administration of vinpocetine or piracetam. In addition, the effect of the non-selective adenosine receptor antagonist theophylline (20 mg/kg ip) or the nonsteroidal anti-inflammatory drug indomethacin (20 mg/kg, ip) was examined. Theophylline or indomethacin was administered 30 min prior to vinpocetine or piracetam (60 min prior to the abdominal constriction assay). In further experiments, the effect of coadministration of the centrally acting dopamine D2 receptor antagonists, sulpiride (10 or 20 mg/kg, ip) and haloperidol (0.5, 1.5 or 3 mg/kg, ip) or D2 receptor agonist bromocryptine (1.5 or 3 mg/kg, ip) on vinpocetine (1.8 mg/kg, ip) or piracetam (300 mg/kg, ip) antinociception was examined. Lastly, the effect of vinpocetine or piracetam on antinociception caused by the tricyclic agent imipramine was studied. Rota-rod test Motor performance in mice was measured as the latency to fall from an accelerating rota-rod located over plates connected to an automatic counter (Ugo Basile, Varese, Italy). Mice were trained to remain on a rotating rod for 2 min as the rod rotated toward the animal. After the 2-min training period, the mice were administered vehicle (saline) or drugs (sc) and 30 min later were placed on the rotating rod as it accelerated from 4 to 40 rpm over 5 min and the time they could remain on the accelerating rod was recorded [25]. The cut-off time was 600 s. The time was measured from the start of the acceleration period. The test was repeated 2 h after vehicle or drug injection. Six animals were used per dose and for the controls. Porsolt’s forced-swimming test In this test, a commonly used tool for screening of potential antidepressants, the floating time, which is considered as the measure of despair, is decreased by the administration of antidepressant drugs [32]. 682 Pharmacological Reports, 2006, 58, 680691 Briefly, each mouse was placed individually in a glass cylinder (diameter 12 cm, height 24 cm) filled with water to a height of 12 cm. Water temperature was maintained at 24–25°C. The animal was forced to swim for 6 min and the duration of immobility was measured. The mouse was considered as immobile when it stopped struggling and moved only to remain floating in the water, keeping its head above water [32]. In two separate sets of experiments, the floating time was recorded after treatment with different doses of vinpocetine (0.45–1.8 mg/kg, sc) or piracetam (37.5–300 mg/kg, sc) and compared to that of imipramine (15 mg/kg, sc). The control group received saline. In the third set of experiments, the possible modulation of the antidepressant effect of imipramine (15 mg/kg, sc) by either vinpocetine (1.8 mg/kg, sc) or piracetam (300 mg/kg, sc) or the possible effect of combined vinpocetine (1.8 mg/kg, sc) and piracetam (300 mg/kg, sc) administration was investigated. Drugs Vinpocetine (Vinporal, Amrya. Pharm. Ind., Cairo, ARE), piracetam (Nootropil, Chemical Industries Development; CID, Cairo, ARE), guanethidine, propranolol hydrochloride, yohimbine hydrochloride, naloxone hydrochloride (Sigma, St. Louis, USA), imipramine hydrochloride, bromocryptine (Novartis Pharma, Cairo, ARE), amitriptyline hydrochloride, haloperidol, indomethacin (Kahira Pharm & Chem. IND Co., Cairo, ARE), glibenclamide (Hoechst Orient, Cairo, ARE), atropine sulfate, baclofen (Misr Pharm Co., Cairo, ARE), domperidone (JanssenCilag, Switzerland), clozapine (APEX Pharma, Cairo, ARE) were used. Analytical-grade glacial acetic acid (Sigma, St. Louis, USA) was diluted with pyrogenfree saline to provide a 0.6% solution for ip injection. All drugs were dissolved in isotonic (0.9% NaCl) saline solution immediately before use. Statistical analyses Data are expressed as the mean ± SE. Differences between vehicle control and treatment groups were tested using one- and two-way ANOVA followed by Duncan’s multiple comparison test. When there were only two groups, a two-tailed Student’s t-test was used. A probability value less than 0.05 was considered statistically significant. Antinociception by vinpocetine and piracetam Omar M.R. Abdel Salam Results Effect of vinpocetine or piracetam on thermal nociception Hot-plate latency (s) The mean reaction time in the hot plate test was significantly delayed at 30 min after the administration of vinpocetine at doses of 0.9 mg/kg or 1.8 mg/kg, compared with basal (pre-drug) values, denoting decreased nociception (p < 0.05, one way ANOVA). Piracetam given at doses of 75–300 mg/kg failed to affect the nociceptive response (Fig. 1). Fig. 2. Effect of different doses of vinpocetine (0.45, 0.9 or 1.8 mg/kg), piracetam (75, 150 or 300 mg/kg), indomethacin (20 mg/kg) or saline (control) on abdominal constrictions caused by injection of dilute acetic acid in mice. Drugs or saline (control) were administered 30 min prior to testing. Data are expressed as the mean ± SE and percent inhibition (%) compared to the control animals. * p < 0.05 . control, n = 6 EF EF LI mice in a dose-dependent manner. The degree of inhibition was 42.3, 53, 63.9% for vinpocetine at 0.45, 0.9 or 1.8 mg/kg (Fig. 2A) and 48.1, 51.3, 76.8% for piracetam at 75, 150 or 300 mg/kg, respectively (Fig. 2B). In comparison, the non-steroidal anti-inflammatory drug indomethacin (20 mg/kg) decreased the number of abdominal constrictions by 54.9%. Fig. 1. Effect of different doses of vinpocetine (0.45, 0.9 or 1.8 mg/kg) or piracetam (75, 150 or 300 mg/kg) in the hot-plate test of thermal pain. Basal and 30-min latencies were determined for each treatment group (saline, vinpocetine or piracetam). The first column represents the basal (pre-drug) latencies and the second column represents the 30 min- (post-drug) values in each treatment group. Saline or drugs were administered 30 min prior to testing. Data are expressed as the mean ± SE. Hot-plate latencies comparisons were made between baseline paw withdrawal latencies (pre-drug values) as compared with the respective post-drug values. * p < 0.05 . basal (pre-drug value), n = 6 EF LI Effect of vinpocetine or piracetam on visceral nociception Either vinpocetine (0.45, 0.9 or 1.8 mg/kg) or piracetam (75, 150 or 300 mg/kg) inhibited the number of writhes induced by ip acetic acid administration in Investigation of the mechanism of visceral antinociception by vinpocetine or piracetam Figures 3–5 show the effect of the a-2 adrenoceptor antagonist yohimbine (4 mg/kg) and a-1 adrenoceptor antagonists prazosin (2 mg/kg) and doxazosin (16 mg/kg) on the nociceptive responses. The administration of prazosin or doxazosin caused a marked reduction in the number of abdominal constrictions. The administration of yohimbine or prazosin at the above-mentioned doses significantly enhanced the antinociceptive action of vinpocetine or piracetam in the abdominal constriction assay. When administered at 16 mg/kg, doxazosin given alone or combined with either vinpocetine or piracetam markedly inhibited the abdominal constrictions by 94.8–90.2% (Fig. 4). To delineate whether there is any synergism between Pharmacological Reports, 2006, 58, 680691 683 Fig. 5. Effect of doxazosin (4 mg/kg) on antinociception caused by vinpocetine (1.8 mg/kg) or piracetam (300 mg/kg) in the abdominal constriction assay. Drugs or saline (control) were administered 30 min prior to testing. Data are expressed as the mean ± SE, * p < 0.05 compared to control group. The plus sign (+) indicates significant change from the other treatment groups, n = 6 EF Fig. 3. Effect of yohimbine (4 mg/kg, ) or prazosin (2 mg/kg, ) on antinociception caused by vinpocetine (1.8 mg/kg, ) or piracetam (300 mg/kg, ) in the abdominal constriction assay. Drugs or saline (control) were administered 30 min prior to testing. Data are expressed as the mean ± SE and percent inhibition (%) compared to the control animals. * p < 0.05 . control and between different groups as shown in the figure. The plus sign (+) indicates significant difference from the yohimbine-treated group, n = 6 EF EF EF EF LI Fig. 6. Effect of atropine (2 mg/kg) or propranolol (2 mg/kg) on antinociception caused by vinpocetine (1.8 mg/kg) or piracetam (300 mg/kg) in the abdominal constriction assay. Drugs or saline (control) were administered 30 min prior to testing. Data are expressed as the mean ± SE and percent inhibition (%) compared to the control animals. * p < 0.05 compared to control and between different groups as shown in the figure. The plus sign (+) indicates significant change from the atropine-treated group. The (#) sign indicates significant difference from the vinpocetine + atropine or vinpocetine + propranolol-treated groups, n = 6 EF Fig. 4. Effect of doxazosin (16 mg/kg) on antinociception caused by vinpocetine (1.8 mg/kg) or piracetam (300 mg/kg) in the abdominal constriction assay. Drugs or saline (control) were administered 30 min prior to testing. Data are expressed as the mean ± SE, * p < 0.05 compared to control group, n = 6 EF 684 Pharmacological Reports, 2006, 58, 680691 Antinociception by vinpocetine and piracetam Fig. 7. Effect of guanethidine (16 mg/kg) on visceral antinociception caused by vinpocetine (1.8 mg/kg) or piracetam (300 mg/kg). Drugs or saline (control) were administered 30 min prior to testing. Data are expressed as the mean ± SE and percent inhibition (%) compared to the control animals. * p < 0.05 compared to control and between different groups as shown in the figure. The plus sign (+) indicates significant change from the guanethidine-treated group, n = 6 EF doxazosin and either nootropic, doxazosin was administered at a lower dose of 4 mg/kg. Figure 5 shows that doxazosin at the dose of 4 mg/kg was able to enhance the piracetam-induced antinociception. The effect of vinpocetine was markedly potentiated by co-administration of the beta-adrenergic antagonist propranolol or muscarinic receptor antagonist atropine, with 99.5% inhibition of the abdominal constriction response. Propranolol or atropine also enhanced the piracetam effect (Fig. 6). Antinociception caused by vinpocetine or piracetam was, in addition, enhanced by co-administration of the adrenergic neuron blocking agent guanethidine. Guanethidine by itself elicited a significant reduction in the number of abdominal constrictions as compared to the control group (Fig. 7). Potentiation of antinociception caused by vinpocetine or piracetam was also observed when the nonspecific opioid receptor antagonist naloxone was administered along with the nootropics. Naloxone administered alone increased the writhing response (Fig. 8A). The potassium channel blocker gibenclamide administered ip 30 min prior to testing inhibited abodominal constrictions but did not affect antino- Glibenclamide + Piracetam Glibenclamide 5 mg/kg Glibenclamide + Vinpocetine N N Omar M.R. Abdel Salam Fig. 8. (A) Effect of naloxone (5 mg/kg) on antinociception caused by vinpocetine (1.8 mg/kg) or piracetam (300 mg/kg) in the abdominal constriction assay. * p < 0.05 . control. The plus sign (+) indicates significant change from the naloxone-treated group. The (#) sign indicates significant difference from the vinpocetine + naloxone or piracetam + naloxone-treated groups. (B) Effect of gibenclamide (5 mg/kg) on visceral antinociception caused by vinpocetine (1.8 mg/kg) or piracetam (300 mg/kg). * p < 0.05 compared to control. The plus sign (+) indicates significant change from the vinpocetine-treated group. Drugs or saline (control) were administered 30 min prior to testing. Data are expressed as the mean ± SE and percent inhibition (%) compared to the control animals, n = 6 LI EF ciception by vinpocetine or piracetam (Fig. 8B). The non-steroidal anti-inflammatory drug indomethacin given 30 min prior to vinpocetine or piracetam increased the antinociceptive response (Fig. 9). The vinpocetine- or piracetam-induced antinociception was, however, inhibited by pretreatment with the nonselective adenosine receptor antagonists theophylline administered at the dose of 20 mg/kg (Fig. 9). The antinociception induced by the nootropic drugs vinpocetine and piracetam was also examined in the presence of the dopamine D2 receptor antagonists, sulpiride and haloperidol or the dopamine D2 receptor agonist bromocryptine. As shown in Figure 10, the antinociception caused by vinpocetine was reduced by sulpiride; while that of piracetam was enhanced by sulpiride. The administration of either vinpocetine or piracetam with haloperidol at 1.5 or 3 mg/kg, almost abolished the writhing response. However, haloperidol administered at 1.5 or 3 mg/kg by itself inhibited the writhing response by 93.1 and 98.4%, respecPharmacological Reports, 2006, 58, 680691 685 Fig. 9. Effect of theophylline (20 mg/kg) or indomethacin (20 mg/kg) on antinociception caused by vinpocetine (1.8 mg/kg) or piracetam (300 mg/kg). Theophylline or indomethacin was administered ip 30 min prior to vinpocetine or piracetam (60 min prior to the abdominal constriction assay). Data are expressed as the mean ± SE and percent inhibition (%) compared to the control animals. * p < 0.05 compared to control and between different groups as shown in the figure, n = 6 Fig. 10. Effect of sulpiride (10 or 20 mg/kg) and haloperidol (1.5 or 3 mg/kg) on antinociception caused by vinpocetine (1.8 mg/kg) or piracetam (300 mg/kg). Drugs or saline (control) were administered 30 min prior to testing. Data are expressed as the mean ± SE and percent inhibition (%) compared to the control animals. * p < 0.05 compared to control. The plus sign (+) indicates significant change from the sulpiride (20 mg/kg)-treated group. The (#) sign indicates significant difference from the sulpiride (10 mg/kg)-treated group, n = 6 EF 686 Pharmacological Reports, 2006, 58, 680691 Fig. 11. Effect of haloperidol (0.5 mg/kg) on antinociception caused by vinpocetine (1.8 mg/kg) or piracetam (300 mg/kg). Drugs or saline (control) were administered 30 min prior to testing. Data are expressed as the mean ± SE and percent inhibition (%) compared to the control animals. * p < 0.05 compared to control. The plus sign (+) or the sign (#) indicates significant change from the other treatment groups, n = 6 EF Fig. 12. Effect of bromocryptine (1.5 or 3 mg/kg) on visceral antinociception caused by vinpocetine (1.8 mg/kg) or piracetam (300 mg/kg). Drugs or saline (control) were administered 30 min prior to testing. Data are expressed as the mean ± SE and percent inhibition (%) compared to the control animals. * p 0.05 compared to control. The plus sign (+) indicates significant change from the piracetam or bromocryptine (1.5 mg/kg)-treated groups, n = 6 EF Antinociception by vinpocetine and piracetam Omar M.R. Abdel Salam Effect of vinpocetine or piracetam in rota-rod test Vinpocetine (0.45, 0.9 or 1.8 mg/kg) or piracetam (75, 150 or 300 mg/kg) did not produce any significant changes on the rota-rod performances of the mice. Both controls and either vinpocetine- or piracetamtreated mice remained on accelerating rotating rod during the acceleration period (5 min) and for 5 min thereafter (data not shown). Effect of vinpocetine or piracetam in Porsolt’s forced-swimming test Effect of baclofen (5 mg/kg) on antinociception caused by vinpocetine (1.8 mg/kg) or piracetam (300 mg/kg). * p < 0.05 compared to control. The plus sign (+) indicates significant change from the piracetam + baclofen (5 mg/kg)-treated group. The (#) sign indicates significant difference from the vinpocetine-treated group, n = 6. (B) Effect of imipramine (15 mg/kg) alone or co-administered with either vinpocetine (1.8 mg/kg) or piracetam (300 mg/kg) or vinpocetine (1.8 mg/kg) + piracetam (300 mg/kg) on visceral nociception. * p < 0.05 compared to control. The plus (+) sign indicates significant difference from the vinpocetine + piracetam-treated group, n = 6. Drugs or saline (control) were administered 30 min prior to testing. Data are expressed as the mean ± SE and percent inhibition (%) compared to the control animals, n = 6 EF tively, vs. the saline-treated control group (Fig. 10). Thus, the effect of a lower dose of haloperidol (0.5 mg/kg, ip) was examined. Figure 11 shows that the piracetam effect was enhanced by a lower dose (0.5 mg/kg) of the dopamine D2 receptor antagonist haloperidol. On the other hand, the administration of the D2 receptor agonist bromocryptine (1.5 or 3 mg/kg) reduced the number of abdominal constrictions in a dose-dependent manner by 30.1 and 61.3%, respectively (Fig. 12). A marked and significant antinociception was still observed when either nootropic was co-administered with bromocryptine (Fig. 12). Figure 13A shows that marked potentiation of antinociception occurred upon a co-administration of vinpocetine and GABA agonist baclofen (5 or 10 mg/kg). In contrast, piracetam antagonized antinociception caused by the low (5 mg/kg), but not the high (10 mg/kg) dose of baclofen (Fig. 13A). When we examined the effect of vinpocetine or piracetam on the imipramine-induced inhibition of the writhing response, we observed that either nootropic enhanced antinociception caused by imipramine (Fig. 13B). Duration of immobility (s) Fig. 13. (A) The floating time, was reduced by 19.9 and 20.8% after treatment with low doses of vinpocetine (0.45 mg/kg) or piracetam (37.5 mg/kg), respectively, but was markedly reduced by 63.4% after treatment with imipramine (15 mg/kg) (Fig. 14A, B). The coadministration of either vinpocetine (1.8 mg/kg) or pi- Fig. 14. Porsolts forced-swimming test. The graph shows three sets of experiments. In parts A & B the effect of different doses of vinpocetine (0.453.6 mg/kg) or piracetam (37.5300 mg/kg) were investigated and compared to that of imipramine (15 mg/kg) or saline. * p < 0.05 compared to saline control. The plus (+) sign indicates significant difference from the imipramine-treated group. The (#) sign indicates significant difference from the vinpocetine (0.45 mg/kg)-treated group. In part C the effect of combined administration of either vinpocetine (1.8 mg/kg) or piracetam (300 mg/kg) with imipramine (15 mg/kg) or the effect of vinpocetine (1.8 mg/kg) combined with piracetam (300 mg/kg) was studied. * p < 0.05 compared to saline control. The plus (+) sign indicates significant difference from the vinpocetine + piracetam-treated group. Data are expressed as the mean ± SE and percent inhibition (%) compared to the control animals, n = 6 Pharmacological Reports, 2006, 58, 680691 687 racetam (300 mg/kg) with imipramine (15 mg/kg) had no significant effect on the antidepressant effect of imipramine (Fig. 14C). Meanwhile, a decrease in immobility time by 31.8% was noted in mice treated with a combination of vinpocetine (1.8 mg/kg) and piracetam (300 mg/kg), suggesting an additive antidepressant effect of either nootropic (Fig. 14C). Discussion The present study provides evidence that the nootropic drugs vinpocetine and piracetam exert pain-modulating effects. In the hot-plate test of thermal pain, vinpocetine showed antinociceptive effect. Vinpocetine is capable of blocking NaV1.8 sodium channel activity, which is likely to be responsible for the analgesic properties of the drug [44]. In this model of supraspinal analgesia, piracetam failed to alter nociception. In another study, nefiracetam, a new member of the piracetam group of cognition enhancers, reversed the thermal hyperalgesia in mouse models of neuropathic pain [33]. It should be noted, however, that members of the 2-oxopyrrolidine group though structurally close to piracetam differ markedly in their pharmacological properties and clinical effects. On the other hand, either vinpocetine or piracetam clearly inhibited the abdominal constrictions induced in mice by injection of dilute acetic acid into the peritoneal cavity, a model of visceral inflammatory pain, brought about by the release of prostaglandins [2]. Vinpocetine and piracetam did not impair motor performance in the rota-rod test, thus ruling out the confounding influence of a possible sedative effect. The inhibition of adrenergic, cholinergic and opioidergic systems appears to facilitate vinpocetine- or piracetam-induced antinociception. The induction of pain behaviors in animals relies upon a stimulus applied to a nociceptive neuron and the activation of a pain pathway and reflexes. Several drugs induce analgesia or antinociception by interfering with the neuronal pathways involved in the receipt and transmission of nociceptive information from the periphery to higher centers in the central nervous system. In this context, the spinal cholinergic system and muscarinic receptors are important for modulation of nociception. Spinal muscarinic agonists, such as carbachol and the cholinesterase inhibitor neostigmine, 688 Pharmacological Reports, 2006, 58, 680691 induce a potent analgesia in the rat; spinal M1 and/or M3 receptor subtypes [26] likely mediate these effects. Activation of spinal muscarinic receptors inhibits dorsal horn neurons through inhibition of the glutamatergic synaptic input [23] and potentiation of synaptic GABA release in the spinal cord [43]. Also, M1-muscarinic agonists increased the pain threshold in the mouse acetic acid writhing test and in rat paw pressure test [1]. In contrast, atropine, a cholinergic muscarinic antagonist, has been reported to produce analgesia when administered at low doses of 1–100 µg/kg, while hyperalgesia was observed with 5 mg/kg of the agent. The analgesia caused by very low doses of atropine was attributed to amplification of cholinergic transmission by a selective blockade of presynaptic muscarinic autoreceptors [15]. In the present study, atropine administered ip at 2 mg/kg increased the number of writhes in the abdominal constriction assay, yet amplified the antinociceptive action of vinpocetine or piracetam. The sympathetic nervous system has also been implicated in the modulation of nociceptive transmission. Certain pain conditions involve the sympathetic nervous system, e.g., visceral pain due to abdominal and pelvic cancers; ischemic pain from peripheral vascular disease, arterial spasm or frostbite and others. Sympathetcomy or intravenous regional sympathetic block with guanethidine can be carried out to reduce pain [35]. Afferent nociceptive fibers from the viscera accompany sympathetic nerves to enter the spinal cord at the dorsal horn. Transmission of pain impulses through the spinal cord can be inhibited by descending reflexes that originate in the noradrenergic neurons of the mesencephalic periductal gray matter, and the pontine locus ceruleus, thereby altering ascending transmission mediating visceral sensation [4]. Behavioral, neurophysiological and clinical evidence shows that most forms of gastrointestinal pain are mediated by activity in visceral afferent fibers running in sympathetic nerves [5]. Sympathetic block interrupts these pathways and also the efferent viscero-visceral reflexes so that ischemia and spasm are relieved [9]. Voltage-gated sodium channels (Nav1.7) have been found predominantly in sensory and sympathetic neurons [42]. Sympathectomy produced in rats by administering 6-hydroxydopamine reduced spontaneous activity of sacral spinal cord neurons and attenuated visceral nociceptive responses due to colorectal distension [19]. Duarte et al. [7] observed a significant inhibition of writhing in the acetic Antinociception by vinpocetine and piracetam Omar M.R. Abdel Salam acid abdominal constriction assay with the adrenergic neuron blocker guanethidine (27% at 30 mg/kg, sc). In the present study, a 30% reduction in the nociceptive response was observed with 16 mg/kg of ip guanethidine. The latter is taken up into adrenergic neurons, where it binds to the storage vesicles and prevents release of the neurotransmitter in response to a neuronal impulse, which results in generalized decrease in sympathetic tone. In the present study, guanethidine potentiated antinociception when coadministered with either nootropic. A decrease in writhing response was also observed after a nonselective beta-adrenoceptor antagonist propranolol. The latter enhanced antinociception elicited by piracetam, whereas its administration with vinpocetine almost abolished the writhing response. Based upon these results, it might be suggested that a decrease in sympathetic tone facilitates antinociception caused by vinpocetine or piracetam. Descending brainstem systems influence nociceptive stimuli spinally while other systems modulate nociceptive input supraspinally. The administration of a-2 adrenoceptor agonists produces anti-nociception in rodents by inhibiting synaptic transmission in the spinal cord dorsal horn and there is an evidence of descending noradrenergic system, the stimulation of which results in the activation of spinal a-2-adrenergic receptors and antinociception [37]. Visceral nociception induced by ip administered 2% solution of acetic acid was reduced dose-dependently by prazosin, an a-1-adrenoceptor antagonist and clonidine, an a-2adrenoceptor agonist [21]. Results of the present study indicated that visceral nociception was markedly inhibited by the administration of a-1 antagonists. The administration of a-1 or a-2 antagonists amplified the vinpocetine or piracetam antinociception. Piracetam exerts GABAB antagonistic effect [13]. There is evidence to suggest that spinally projecting noradrenergic A7 neurons in the dorsolateral pontine tegmentum may be under tonic inhibitory control by GABA neurons [29]. Removal of inhibitory GABAB mechanisms by piracetam might thus facilitate a descending noradrenergic pathway so as to alter nociception. This hypothesis, however, cannot explain the potentiating effect of a-1 or a-2 antagonists on vinpocetine antinociception. Unexpected also was the finding that the visceral antinociceptive effects of vinpocetine or piracetam were enhanced by co-administration the opioid receptor antagonist naloxone. The latter increased the no- ciceptive behavior in the abdominal constriction assay when administered alone and was thus expected to reduce antinociception by the two nootropic drugs. Voltage-gated potassium channels can also contribute to the sensitization of primary afferents observed in gastrointestinal pain states [6]. The possible involvement of ATP-gated potassium channels in the mediation of antinociception induced by vinpocetine or piracetam is ruled out, in view of the inability of glibenclamide, an ATP-sensitive potassium channels blocker to reduce their antinociceptive effect. Adenosine is an inhibitory neuromodulator that can increase nociceptive thresholds in response to noxious stimulation [34] and blockade of adenosine receptors by theophylline, a non-selective adenosine receptor antagonist at A1 and A2 was shown to induce hyperalgesia [30]. The antinociceptive effects of vinpocetine or piracetam were reversed by prior administration of the adenosine receptor blocker theophylline. Therefore, it is suggested that an adenosine sensitive mechanism is likely to be responsible for the visceral antinociceptive properties of both nootropic drugs. Baclofen, a prototypical agonist of GABAB receptors, alters nociception at the level of the spinal cord by acting on GABAB receptors located on primary afferent terminals and is known to produce analgesia in man and animals [18]. In the present work, baclofen markedly inhibited the nociceptive response in the abdominal constriction assay. The drug potentiated antinociception elicited by vinpocetine. In contrast, piracetam antagonized antinociception caused by the low dose (5 mg/kg), though not the high dose (10 mg/kg) of baclofen. The prevention of baclofen antinociception is in accordance with other studies. Piracetam (and also aniracetam) antagonized GABAergic antinociception caused by baclofen [13]. Dopamine D2 receptors are involved in nociceptive and analgesic mechanisms [12, 38] and there is evidence to suggest that dopamine may acts tonically in the cortex to inhibit nociception [3]. In the present study, haloperidol itself dose-dependently inhibited the nociceptive behavior. In contrast, sulpiride, a highly selective D2-dopamine receptor antagonist, increased the nociceptive response. It is likely that different pharmacological receptor binding profiles of the two antagonists might be associated with different effects on visceral nociception. Haloperidol is a partially selective dopamine D2 receptor antagonist [24]. The involvement of other dopamine receptors as well is likely to account for the antinociceptive effect of ha- Pharmacological Reports, 2006, 58, 680691 689 loperidol seen in the present study. Haloperidol at 0.5 mg/kg potentiated antinociception caused by piracetam. On the other hand, sulpiride reduced antinociception caused by vinpocetine, but enhanced that of piracetam. Blockade of D2 receptors thus potentiates piracetam antinociception, but might reduce vinpocetine antinociception. These results suggest alteration of dopaminergic neurotransmission by modifying the D2-receptors which can alter antinociception induced by the two nootropic drugs. Antidepressant drugs such as clomipramine or imipramine can also modulate visceral nociception [14]. Data from the present study indicate that vinpocetine or piracetam are likely to enhance visceral antinociception caused by imipramine. Interestingly, when examined in the forced-swimming test in mice, a commonly used tool for screening of potential antidepressants [32], low doses of vinpocetine and also piracetam displayed antidepressant-like activity. In summary, vinpocetine, but not piracetam reduced thermal nociception. The two nootropics, however, displayed marked antinociceptive effect on visceral pain caused by ip injection of acetic acid in mice. This effect depended on the activation of adenosine receptors. Cholinergic muscarinic blockade with atropine, adrenorecptor blockade or opioid antagonism with naloxone potentiated vinpocetine or piracetam-induced antinociception. An interaction at the level of dopamine D2 receptors by the two nootropic agents is also suggested. Acknowledgment: The author acknowledges Wael Zedan and Mohamed Abd-Elaziz for their technical assistance in the experiments. 5. 6. 7. 8. 9. 10. 11. 12. 13. 14. 15. 16. 17. References: 1. Bartolini A, Ghelardini C, Fantetti L, Malcangio M, Malmberg-Aiello P, Giotti A: Role of muscarinic receptor subtypes in central antinociception. Br J Pharmacol, 1992, 105, 77–82. 2. Berkenkopf JW, Weichman BM: Production of prostacyclin in mice following intraperitoneal injection of acetic acid, phenylbenzoquinone and zymosan: its role in the writhing response. Prostaglandins, 1988, 36, 693–709. 3. Burkey AR, Carstens E, Jasmin L: Dopamine reuptake inhibition in the rostral agranular insular cortex produces antinociception. J Neurosci, 1999, 19, 4169–4179. 4. Camilleri M, Saslow SB, Bharucha AE: Gastrointestinal sensation: mechanisms and relation to functional gastro- 690 Pharmacological Reports, 2006, 58, 680691 18. 19. 20. 21. 22. intestinal disorders. In: Gastroenterology Clinics of NA: Gastrointestinal Motility in Clinical Practice, vol. 25. Ed. Camilleri M, Saunders, Philadelphia, 1996, 247–258. Cervero F: Neurophysiology of gastrointestinal pain. Baillieres Clin Gastroenterol, 1988, 2, 83–99. Cervero F, Laird JM: Role of ion channels in mechanisms controlling gastrointestinal pain pathways. Curr Opin Pharmacol, 2003, 3, 608–612. Duarte ID, Nakamura M, Ferreira SH: Participation of the sympathetic system in acetic acid-induced writhing in mice. Braz J Med Biol Res, 1988, 21, 341–343. Eckert GP, Cairns NJ, Muller WE. Piracetam reverses hippocampal membrane alterations in Alzheimer’s disease. J Neural Transm, 1999, 106, 757–761. Eisenberg E, Carr DB, Chalmers TC. Neurolytic celiac plexus block for treatment of cancer pain: a meta-analysis. Anesth Analg, 1995, 80, 290–295. Fedi M, Reutens D, Dubeau F, Andermann E, D’Agostino D, Andermann F: Long-term efficacy and safety of piracetam in the treatment of progressive myoclonus epilepsy. Arch Neurol, 2001, 58, 781–786. Fischhof PK, Moslinger-Gehmayr R, Herrmann WM, Friedmann A, Russmann DL: Therapeutic efficacy of vincamine in dementia. Neuropsychobiology, 1996, 34, 29–35. Frussa-Filho R, Rocha JB, Conceicao IM: Effects of dopaminergic agents on visceral pain measured by the mouse writhing test. Arch Int Pharmacodyn Ther, 1996, 331, 74–93. Galeotti N, Ghelardini C, Bartolini A: Piracetam and aniracetam antagonism of centrally active drug-induced antinociception. Pharmacol Biochem Behav, 1996, 53, 943–950. Ghelardini C, Galeotti N, Bartolini A: Antinociception induced by amitriptyline and imipramine is mediated by alpha2A-adrenoceptors. Jpn J Pharmacol, 2000, 82, 130–137. Ghelardini C, Malmberg-Aiello P, Giotti A, Malcangio M, Bartolini A: Investigation into atropine-induced antinociception. Br J Pharmacol, 1990, 101, 49–54. Giurgea C: The “nootropic” approach to the pharmacology of the integrative activity of the brain. Cond Reflex, 1973, 8, 108–115. Hadjiev D: Asymptomatic ischemic cerebrovascular disorders and neuroprotection with vinpocetine. Ideggyogy Sz, 2003, 56, 166–172. Hara K, Saito Y, Kirihara Y, Sakura S: The interaction between gamma-aminobutyric acid agonists and diltiazem in visceral antinociception in rats. Anesth Analg, 2004, 98, 1380–1384. Kalmari J, Niissalo S, Konttinen YT, Pertovaara A: Modulation of visceral nociceptive responses of rat spinal dorsal horn neurons by sympathectomy. Neuroreport, 2001, 12, 797–801. Kessler J, Thiel A, Karbe H, Heiss WD: Piracetam improves activated blood flow and facilitates rehabilitation of poststroke aphasic patients. Stroke, 2000, 31, 2112–2116. Korzeniewska-Rybicka I, Plaznik A: Role of serotonergic and noradrenergic systems in a model of visceral pain. Pol J Pharmacol, 2001, 53, 475–480. Koster R, Anderson M, De Beer EJ: Acetic acid for analgesic screening. Fed Proc, 1959, 18, 412. Antinociception by vinpocetine and piracetam Omar M.R. Abdel Salam 23. Li DP, Chen SR, Pan YZ: Role of presynaptic muscarinic and GABA(B) receptors in spinal glutamate release and cholinergic analgesia in rats. J Physiol, 2002, 543, 807–818. 24. Melis MR, Succu S, Mascia MS, Argiolas A, Bernard B: PD-168077, a selective dopamine D4 receptor agonist, induces penile erection when injected into the paraventricular nucleus of male rats. Neurosci Lett, 2005, 379, 59–62. 25. Millan MJ, Bervoets K, Rivet J-M, Widdowson P, Renouard A, Le Marouille-Girardon S, Gobert A: Multiple alpha -adrenergic receptor subtypes. II. Evidence for a role of rat R )-ARs in the control of nociception, motor behaviour and hippocampal synthesis of noradrenaline. J Pharmacol Exp Ther, 1994, 270, 958–972. 26. Naguib M, Yaksh TL: Antinociceptive effects of spinal cholinesterase inhibition and isobolographic analysis of the interaction with mu and alpha 2 receptor systems. Anesthesiology, 1994, 80, 1338–1348. 27. Nikolova M, Petrova L, Dushkova R: Effect of piracetam in models of experimental inflammation. Int J Tissue React, 1984, 6, 17–21. 28. Nosalova V, Machova J, Babulova A: Protective action of vinpocetine against experimentally induced gastric damage in rats. Arzneimittelforschung, 1993, 43, 981–985. 29. Nuseir K, Proudfit HK: Bidirectional modulation of nociception by GABA neurons in the dorsolateral pontine tegmentum that tonically inhibit spinally projecting noradrenergic A7 neurons. Neuroscience, 2000, 96, 773–783. 30. Paalzow GH: Noradrenaline but not dopamine involved in NMDA receptor-mediated hyperalgesia induced by theophylline in awake rats. Eur J Pharmacol, 1994, 252, 87–97. 31. Paget GE, Barnes JM. Toxicity tests. In: Evaluation of Drug Activities Pharmacometics. Eds. Laurence DR, Bacharach AL, Academic Press, London, New York, 1964, 1–135. 32. Porsolt RD, Le Pichon M, Jalfre M: Depression: a new animal model sensitive to antidepressant treatments. Nature, 1977, 266, 730–732. 33. Rashid MH, Ueda H: Nonopioid and neuropathy-specific analgesic action of the nootropic drug nefiracetam in mice. J Pharmacol Exp Ther, 2002, 303, 226–231. 34. Sawynok J: Adenosine receptor activation and nociception. Eur J Pharmacol. 1998, 347, 1–11. 35. Serpell M: Role of the sympathetic nervous system in pain. Anaesth Intensive Care Med, 2005, 6, 52–55. 36. Shorvon S: Pyrrolidone derivatives. Lancet, 2001, 358, 1885–1892. 37. Tanabe M, Takasu, K, Kasuya N: Role of descending noradrenergic system and spinal alpha2-adrenergic receptors in the effects of gabapentin on thermal and mechanical nociception after partial nerve injury in the mouse. Br J Pharmacol, 2005, 144, 703–714. 38. Taylor BK, Joshi C, Uppal H: Stimulation of dopamine D2 receptors in the nucleus accumbens inhibits inflammatory pain. Brain Res, 2003, 987, 135–143. 39. Vakulina OP, Iasnetsov VV, Isachenkov VA, Krylova IN, Tishkova IP, Bragin EO, Popkova EV: Effects of piracetam on pain sensitivity and levels of beta-endorphin in blood and cAMP in the cerebral cortex of rats (Russian). Biull Eksp Biol Med, 1990, 109, 163–165. 40. Vas A, Gulyas B, Szabo Z, Bonoczk P, Csiba L, Kiss B, Karpati E, Panczel G, Nagy Z: Clinical and non-clinical investigations using positron emission tomography, near infrared spectroscopy and transcranial Doppler methods on the neuroprotective drug vinpocetine: a summary of evidences. J Neurol Sci, 2002, 203–204, 259–262. 41. Waegemans T, Wilsher CR, Danniau A, Ferris SH, Kurz A, Winblad B: Clinical efficacy of piracetam in cognitive impairment: a meta-analysis. Dement Geriatr Cogn Disord, 2002, 13, 217–224. 42. Wood JN, Boorman JP, Okuse K, Baker MD: Voltagegated sodium channels and pain pathways. J Neurobiol, 2004, 61, 55–71. 43. Zhang HM, Li DP, Chen SR: M2, M3, and M4 receptor subtypes contribute to muscarinic potentiation of GABAergic inputs to spinal dorsal horn neurons. J Pharmacol Exp Ther, 2005, 313, 697–704. 44. Zhou X, Dong XW, Crona J, Maguire M, Priestley T: Vinpocetine is a potent blocker of rat NaV1.8 tetrodotoxin-resistant sodium channels. J Pharmacol Exp Ther, 2003, 306, 498–504. Received: April 6, 2006; in revised form August 22, 2006. Pharmacological Reports, 2006, 58, 680691 691