Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
DNA vaccination wikipedia , lookup
Lymphopoiesis wikipedia , lookup
Immune system wikipedia , lookup
Monoclonal antibody wikipedia , lookup
Innate immune system wikipedia , lookup
Cancer immunotherapy wikipedia , lookup
Adaptive immune system wikipedia , lookup
Adoptive cell transfer wikipedia , lookup
Molecular mimicry wikipedia , lookup
Human leukocyte antigen wikipedia , lookup
Immunosuppressive drug wikipedia , lookup
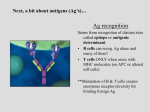
PRACTICAL TRANSPLANT IMMUNOLOGY Dr Nisar Anwar FRCP(Edin),Accredited Renal Physician (UK) Professor & Head : Department Of Nephrology KTH, Peshawar TERMINOLOGY OF TRANSPLANTATION • Auto graft (e.g. skin grafts for burns, etc.) • Syngraft (genetically identical twins; some stem cell therapies: nuclear transfer, iPS approaches) – – No immunologic rejection for these two types • Allograft (genetically distinct member of same species; almost all medical transplants) • Xenograft (different species; attractive due to shortage of organs for transplants) – – Very severe rejection problems. IMMUNOLOGY OF TRANSPLANTATION • Major barrier to organ/tissue transplantation is immunological • Immune system recognizes transplant as foreign and destroys it – Memory and specificity have properties of adaptive immune response – Memory is transferred by T cells (antibodies also can contribute). HISTOCOMPATIBILITY ANTIGENS • ABO blood group antigens Pre-existing antibodies to A or B antigens lead to – “hyperacute rejection” if not matched properly • Major histocompatibility antigens – Encoded by the MHC, originally discovered for their role in skin graft rejection in mice • Minor histocompatibility antigens Allelic variants of normal cellular proteins. Transplantation antigens Major Histocompatibility Complex (MHC): – Class I antigens: constitutively expressed on surface of most cells – Class II antigens: expressed on cells of lymphoid system – Expression of MHC molecules can be up regulated by ischemia, etc. – nomenclature • HLA (human) class I: A, B, C; class II: DR, DQ • H-2 (mouse) class I: K, D, L; class II: IA, IE MHC NOMENCLATURE • Identified & characterized over 40 years ago • Antigens were identified using antisera obtained from multiparous women, new antisera can split HLA antigens in to narrower specificities • DNA based techniques are more accurate in describing alleles • Frequency of antigens, alleles and combinations vary considerably • Most common HLA antigen A2 is found in 50% of the population. MHC STRUCTURE MHC CHARACTERISTICS • Polymorphism – Each MHC locus can express any one of hundreds of different molecules – Set of different MHC molecules or alleles expressed on one chromosome is called a Haplotype – A Genotype is the sum of two haplotypes • Genes are co-dominantly expressed – An individual expresses alleles from both chromosomes at each locus INHERITANCE • Each parental chromosome 6 provides a haplotype or linked set of MHC genes to the offspring. • Haplotypes are usually inherited intact from each parent • The child carries one representative antigen from each of class I & class II loci of each parent • A child is a one haplotype match to each parent • HLA haplotypes are inherited in a mendelian fashion • 25% siblings will share two haplotype match, 50% will share one haplotype and 25% will have zero match HLA-sensitization • Exposure to non-self HLA antigens can cause production of HLA-directed antibodies • Common causes of HLA-sensitization include blood transfusions, pregnancies, previous transplants • In infants, tissue patches implanted during cardiac surgery cause sensitization Does MHC (HLA) ‘Matching’ Prevent Rejection? • Reduces rejection but there are still ‘minor histocompatibility antigens’ (MiHA) • MiHA are probably polymorphisms affecting peptides in the grooves • But we cannot MHC-match most grafts: too much polymorphism, too little time, too few donors • Therefore need immunosuppression Matching and Cross-Matching • Matching: finding a donor who shares the HLA antigens of the recipient, to minimize antigen disparities – requires donor and recipient antigens to be identified • Cross-matching: testing the SERUM of the recipient for antibodies against the donor antigens Identifying MHC Polymorphisms (‘tissue typing’) • Formerly determined by antibodies against MHC molecules HLA typing MLR • Now by DNA testing: allele-specific PCR, sequencing Tissue Typing(or HLA-typing) Used to identify HLA molecules on cells Ab against HLA1 + complement Donor Recipient Cells die, appear blue MIXED LYMPHOCYTE REACTION: Recipient Donor + (Irradiate) Cell Proliferation Strong Proliferation--->High incompatibility Weak proliferation--->Low incompatibility No proliferation---> 100% compatibility Helps to identify any antigenic differences between donor and recipient CD4 & CD8 Subsets Of T Cells • CD 4 or Helper subset of T cells directly bind MHC class II molecules • CD 8 or Cytolytic subset of T cells directly bind MHC class I molecules • CD 4 cells mediate initial recognition of an allograft • CD 4 deficient mice are unable to reject grafts while CD 8 deficient mice do reject grafts. TCR SPECIFICITY AND SELF-MHC • MHC molecules are highly polymorphic • During development in the thymus, T cells are selected for moderate/weak binding to self-MHC + a self-peptide (“positive selection”) • During development in the thymus, T cells are killed (or become regulatory T cells) if they have strong binding to selfMHC + a self-peptide (“negative selection”) • Do the T cells of one person “see” MHC molecules from another person? Actually about 1% of T cells bind such MHC with self peptide strongly--like a microbial antigen/MHC complex-- and become activated (“alloreactive T cells”) DIRECT PRESENTATION • Direct presentation in transplantation (MHC + peptide: MHC is from graft; peptides are from cellular proteins, graft and/or host) • Graft dendritic cell is induced to mature, express costimulatory molecules (B7) and migrate to lymph node by stress of surgery, etc. • DC in lymph node activates allo-MHC recognizing CD4+ T cells and CD8+ T cells • Activated T cells expand and then home to sites of inflammation where they find allo-MHC on graft cells and secrete cytokines/kill graft cells • This is the critical pathway for CD8 T cell response. DIRECT PRESENTATION IN GRAFT REJECTION • Blue: host cell; pink: graft cell see also Abbas et al. Fig. 10-8. Semi-direct Antigen Presentation the Membrane Patch Pathway Host CD8+ cytotoxic cell Host CD8+ T cell Class I Allogeneic Donor Cell Shed membrane with donor MHC Intact donor MHC Host APC INDIRECT PRESENTATION • Indirect presentation in transplantation (MHC + peptide: MHC is from host, peptide may be • from graft MHC) • Dendritic cell pick up antigens (e.g. allo-MHCs), and load peptides from these allo-MHC onto their own MHC II, migrate to lymph nodes and activate T cells • CD4+ T cells are activated and then migrate to sites of inflammation where they are activated by host macrophages or DCs presenting graft antigens, leads to inflammatory reaction and tissue damage. • The indirect pathway is probably responsible for chronic rejection (rejection after 1 year) INDIRECT PRESENTATION IN GRAFT REJECTION Allorecognition: Indirect Pathways CD8+ cytotoxic cell CD4+ T cell IL-2 Class I Allogeneic Donor Cell Shed Allogeneic MHC (donor class I-derived peptide presented by host class II molecules) Donor MHC molecules are taken up and processed by host antigen presenting cell Host antigen presenting cell 3 Signals for T Cell Responses APC Ag signal 1 costimulation signal 2 cytokines B7 CD28 IL-2 signal 3 T cell activation key genes e.g.IL-2, CD40L IL- 15 etc G1 S replication M G2 Expression of effector activity Three-Signal Model Halloran, N Eng J Med, 2004;351:3715 ROLE OF CO-STIMULATORY PATHWAY • Do Alloreactive T cells need co stimulation? • Ordinarily T cell immune responses require co-stimulation (B7/CD28) • Blocking co stimulation with CTLA4-Ig, “belatacept” protects against acute graft rejection in kidney patients (phase III clinical trials published in 2010; FDA approval in 2011) • Most likely explanation: -ischemia, stress to organ, release of DAMPs can induce expression of co-stimulators -may explain why live donor organs have superior outcomes for kidney transplants compared to cadaver donor organs. CNIs Halloran, N Eng J Med, 2004;351:3715 CALCINEURIN PATHWAY MECHANISM OF IMMUNOSUPPRESSION BY CYCLOSPORINE • NF-AT: nuclear factor of activated T cells NF-AT is required for transcription of the IL-2 gene and some other cytokine genes • NF-AT cannot be activated in presence of cyclosporine. Corticosteroids Corticosteroids Halloran, N Eng J Med, 2004;351:3715 Mycophenolates Halloran, N Eng J Med, 2004;351:3715 m-TOR inhibitors Halloran, N Eng J Med, 2004;351:3715 ROLE OF B LYMPHOCYTES • Key role in hyper acute rejection. • B cells are less important than T cells in initiating an allo response but antibody formation can play a role in the effecter phase of graft destruction and chronic rejection. LEUKOCYTE RECRUITMENT Transplantation Antigens ABO system – ABH antigens are complex carbohydrate (polysaccharide) structures on surface of many cell types including graft cells & RBC; genes encode production of specific glycosyltransferases catalyze addition of terminal trisaccharide – nomenclature • • • • H antigen: base chain; defines blood type O A trisaccharide on H chain: blood type A or A1 B trisaccharide on H chain: blood type B A and B trisaccharides on H chains: blood type AB The ABO Blood Group Barrier in Organ Transplantation • ‘ABO’ antigens: carbohydrate structures expressed on many tissues and organs, including endothelium of organ transplants • Recipient pre-formed ‘natural’ anti-A or anti-B antibodies to non-self A/B antigens • Transplantation of ABO-incompatible organs: ‘Hyperacute’ rejection ‘isohemagglutinins’ ABO compatibility between donor and recipient is crucial to avoid rapid graft rejection © 2007 New Science Press Ltd new-science-press.com ABO Incompatible Renal Transplantation • • • • • Plasmapharesis IVIG CMV-IVIG Splenectomy Pre Transplant Immunosuppression TYPES OF TRANSPLANT GRAFT REJECTION • Antibody-mediated rejection (AMR) – Hyperacute rejection – Acute or delayed AMR • Cellular rejection • ‘Chronic’ rejection