Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Lymphopoiesis wikipedia , lookup
Immune system wikipedia , lookup
Adaptive immune system wikipedia , lookup
Hygiene hypothesis wikipedia , lookup
Molecular mimicry wikipedia , lookup
Polyclonal B cell response wikipedia , lookup
Management of multiple sclerosis wikipedia , lookup
Innate immune system wikipedia , lookup
Cancer immunotherapy wikipedia , lookup
Adoptive cell transfer wikipedia , lookup
Autoimmunity wikipedia , lookup
Psychoneuroimmunology wikipedia , lookup
Multiple sclerosis research wikipedia , lookup
X-linked severe combined immunodeficiency wikipedia , lookup
Sjögren syndrome wikipedia , lookup
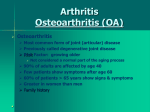
What is rheumatoid arthritis and are novel immunomodulatory therapies the preferable treatment? By Tristan Holt Introduction: This project was inspired by some work experience I undertook at University Hospital Southampton’s Immunology Labs where my supervisors were working on a potential immunomodulatory therapy to help cure rheumatoid arthritis. Rheumatoid arthritis is an autoimmune disease caused by the immune system’s reactivity to synovial cells. This leads to inflammation of the synovium, an increase in synovial fluid and eventually destruction of the joint. A close family friend suffers from this debilitating disease and her experiences of the symptoms, living with the disease and the treatment she has had to undertake helped me greatly to understand those respective areas as well as providing original information to be included within the dissertation. Fig.1. This image was taken from WebMD and shows how rheumatoid arthritis can affect the joints in a sufferer’s hand. 1|Page Contents Abstract ................................................................................................................................................... 2 Glossary ................................................................................................................................................... 3 Literature Review .................................................................................................................................... 3 A brief overview of the immune system: .......................................................................................... 3 How the immune system causes autoimmune disorders:................................................................ 5 Rheumatoid arthritis: ......................................................................................................................... 6 Current Treatments and therapies: ................................................................................................... 8 Extended Project Discussion: Can symptoms and signs of rheumatoid arthritis be alleviated completely by novel immunomodulatory therapies? ............................................................................ 9 Why is a new treatment needed? ..................................................................................................... 9 The success in treating psoriatic arthritis:....................................................................................... 11 What is Apremilast and how is it relevant? .................................................................................. 11 Why is Apremilast not used already? ........................................................................................... 11 Are novel immunomodulatory therapies the only alternative? .................................................... 12 Stem Cell Based Therapies ............................................................................................................ 12 Gene Therapy: ............................................................................................................................... 13 Are novel immunomodulatory therapies the most promising treatment? ................................... 14 Further Reading .................................................................................................................................... 16 Bibliography and Source Review ......................................................................................................... 16 Review of PubMed ............................................................................................................................ 21 Abstract Rheumatoid arthritis is an autoimmune disease in which the target antigen is presented by the cells in the synovium. The resultant swelling can cause lasting damage to the surrounding bone, leading to permanent deformation. Current treatments for rheumatoid arthritis involve a range of immunosuppressant drugs and other drugs to counteract the symptoms of these, specifically the significantly dampened immune response making the immune system far less efficient at combating pathogens that lead to infections. The discussion focuses on the apparent superiority of novel drugs like apremilast, for specific inhibition of TNF- α production in synovial joints, over the current treatment adalimumab, which prevents TNF- α interaction throughout the whole body. Although apremilast is not currently used to treat rheumatoid arthritis, it is used to treat psoriatic arthritis, a similar autoimmune form of arthritis. Other non-drug based novel therapies, such as stem cell therapy and gene based therapy, are also evaluated and compared to both current treatments and the potential development of a more specific TNF- α inhibitor. It is concluded that specific inhibitors of TNF- α in the synovial joints are the most promising of novel therapies. 2|Page Glossary Antigen – An abbreviation of antibody generator, an antigen is effectively any structural substance present on a cell surface membrane that can be recognised by the specific immune response. Cytokines – The name given to a very broad group of small proteins used to alter the activity of other cells. Exons – A section of DNA containing bases that encodes for a protein. HLA-DR – The cell surface membrane used to present antigens to T cells. Immunopathogenesis – The process of the development of a disease where an element of the immune function is involved. Interleukin – A group of cytokines (mostly synthesized by CD4 T helper cells) that have complex immunomodulatory functions. The deficiency of these cytokines affects the growth and differentiation of T and B cells, commonly leading to an autoimmune disease.1 Introns – A section of DNA that contains bases that do not encode for a protein. Lymphocytes – The group of specific white blood cells that include natural killer cells, T cells and B cells. The names of these refer to where the cells mature; B cells in the bone marrow and T cells in the thymus. Lysozymes – A group of enzymes commonly used to break down bacterial cell walls but are also used to break down body cells at the end of their lives. Macrophages – A group of innate white blood cells that ingest cellular debris. Mast Cells – A white blood cell found in tissues that release histamine. Monocytes – The largest of the white blood cells, they can be signalled to move to the site of infection where they differentiate into macrophages. Neutrophils – These make up the majority of white blood cells and are the first to the infection. Like all phagocytes, they are capable of engulfing and digesting pathogens. Pannus Tissue – An abnormal layer of fibrous tissue. Pathogen – An extremely broad term typically referring to an infective agent that can cause the development of a disease. This may be a virus, bacterium or something else. Pathophysiology – The merging of pathology (the study of a disease) and physiology (the study of biological processes) and how these two interact. Phagocytes – The broad class of innate white blood cells which engulf and digest pathogens. This group includes: neutrophils, monocytes, macrophages, mast cells, and dendritic cells. Synovial joints – The most common joint in a mammal. They can be characterised from fibrous and cartilaginous joints by the presence of a surrounding capsule filled with synovial fluid.2 Literature Review A brief overview of the immune system: The immune system is part of a group of bodily systems by which we, as living organisms, protect ourselves against harmful pathogens. Other elements of this prevention method include the skin, 1 Brocker C, Thompson D, Matsumoto A, Nebert DW, Vasiliou V: Evolutionary divergence and functions of the human interleukin (IL) gene family. Human Genomics 5 (Oct 2010) 2 The glossary was mostly comprised of words and definitions that could be found in the A-level textbook: Salters –Nuffield Advanced Biology for Edexcel A2 Biology. Published by Pearson Education Limited in 2009. 3|Page enzymes in saliva, tears and intestinal tract and mucus in the lungs. The immune system consists of two stages: the innate response and the specific response. The innate response is by far the quicker reacting of the two but, because of this speed, it is less advanced or effective [2]. This consists predominantly of phagocytic white blood cells, such as macrophages and neutrophils. Macrophages are initially monocytes that squeeze through gaps in capillary walls to reach an infection site where they then expand and become able to engulf and break down pathogens using lysozyme. The more important of the two phagocytes are the neutrophils that not only engulf and break down pathogens, but also use antigens from the pathogens and present these in their cell surface membrane, becoming antigen presenting cells (APCs). This process is so vital as it activates the specific immune response. Other elements of the innate response include various cells and soluble mediators involved in the process of acute inflammation and endothelial cell activation. Through the process of inflammation, histamine released from mast cells dilates the blood vessels around the infection site and increases the permeability of the capillaries. This allows white blood cells, including phagocytes and lymphocytes, to reach any infecting pathogens more quickly. The specific immune response, triggered by the APCs, often only becomes active after the failure or continued stimulation of the innate response. This happens by the CD4 glycoprotein on T helper cells binding to the antigen on the APCs surface, then in turn releasing cytokines to activate T killer cells, or by binding to B cell APCs to stimulate the production of antibodies3. A visual representation of those cells involved in the immune response is shown in fig.2. 3 John W. Baynes & Marek H. Dominiczak, Medical Biochemistry Second Edition. Published by Elsevier Mosby: 4|Page Fig. 2: This diagram shows a simple ‘Family Tree’ of white blood cells and their functions. B cells are a type of lymphocyte that mature in the bone marrow. They can be distinguished from other types of lymphocytes by the presence of the B cell receptor (BCR) in their outer membrane; this allows them to attach to or recognise a specific antigen on a cell or biological molecule [3]. Their main function is to produce antibodies, which attach to a specific antigen on the perceived pathogen. These antibodies have the structural shape of a Y with the two upper tips forming active sites. Once attached, the antibodies effectively make the antigen accessible for phagocytosis. This can be done in many ways such as precipitating soluble antigens, tagging to make identification easier, sticking particulate antigens together so they are less mobile and easier to engulf, or preventing reproduction. The production of these antibodies and cytokines is called the humoral response. They also differentiate into B memory cells which creates a quicker and more effective response if the antigen is encountered again as the memory cells remain in the blood stream for many years4. T cells are also lymphocytes, but their structure and function differs from B cells. T cells can be recognised by the presence of the T cell receptor (TCR) on their surface and derive their name from the thymus, where they mature, although they are originally created in the bone marrow [3]. Unlike B cells, T cells do not produce antibodies when activated by a T memory cell. Instead they activate phagocytes, antigen-specific cytotoxic T lymphocytes (natural killer T cells), and release a multitude of cytokines; this is called the cellular response. Both B and T cells can recruit and use cells from the innate response and use them in a more direct and efficient manner5. How the immune system causes autoimmune disorders: ‘Autoimmunity (self-reactivity) is normally avoided by thymic education; a breakdown in the process involved leads to autoimmune disease’ – John W. Baynes, PhD, in ‘Medical Biochemistry’ second edition. Published by Elsevier Mosby [3]. Like all cells and biological molecules, our body cells have unique antigens on their surface. Thymic education is the process by which cells involved in the immune response are taught to recognise body cells as ‘self’. This is done by the elimination or inactivation of self-reactive clones of immune cells. This is a complex and multi-layered strategy that is almost always completely effective. However, if this process is circumvented or breaks down, the results are self-reactive immune response cells. This state of immune reactivity and the inflammatory damage causes an autoimmune disease [3]. Different diseases develop depending upon which antigen is targeted and the immune response to it. If a ubiquitous antigen is targeted, this leads to ‘non-organ specific autoimmune diseases’. With these conditions, effects of the self-reactivity can be seen all over the body as the targeted antigen is common to many cells. An example of this is systemic lupus erythematosus (SLE) where apparent target antigens are located in the nucleus of body cells and effects are commonly seen in the skin, joints, kidney and nervous system. At the other end of the spectrum to this is selfreactivity, where the target antigens are unique to a specific type of cell. These are called ‘specific 4 Mauri Claudia & Bosma Anneleen, Immune regulatory function of B cells (2012) Annual review of immunology, January 2012 5 Alberts B, Johnson A, Lewis J, Raff M, Roberts K, Walter P, Molecular Biology of the Cell (2002) published by Garland science: New York. 5|Page autoimmune diseases’, an example of which is autoimmune thyroiditis where the apparent antigen is thyroid peroxidase [3]. Rheumatoid arthritis: Rheumatoid arthritis is the condition caused when immune cells become self-reactive against the cells in the synovium surrounding the sufferer’s joints, although the exact antigen the synovial cells possess that causes this reaction is currently unknown (possibly Type II collagen) [3]. The part of the body most commonly damaged is the hands due to the large number of delicate synovial joints. This systemic inflammatory disease affects almost 400,000 people in the UK alone, with it affecting about 1% of the population worldwide and being almost three times more likely to occur in women than men6. Although people of all ages can develop the disease, the peak incidence is in those patients around the age of 70 years old. Like the majority of autoimmune diseases, the cellular and molecular mechanisms of rheumatoid arthritis have been described in detail. However very little is known about its causes. It has been suggested that the onset of rheumatoid arthritis is triggered by a viral infection, but as of yet there is no conclusive evidence to support this. However trends can be found to identify those who are at most risk. Rheumatoid arthritis is more common in people who smoke, eat a lot of red meat and drink a lot of coffee, whilst the incidence is reduced in those who have a high vitamin C level and drink alcohol in moderation. If a person has an identical twin that suffers from rheumatoid arthritis, there is a 1 in 5 chance that they will develop it as well. This shows that genes increase the likelihood of development but do not determine whether the disease develops definitively. Cold, damp conditions are seen to worsen the symptoms but do not cause the disease itself [6]. Rheumatoid arthritis is characterised by the formation of pannus tissue around the synovial joints caused by the proliferation of blood vessels and swelling of the synovium. This in turn damages the articular cartilage and the adjacent bone. Synovial joints are the most abundant and movable joints in mammals; they involve capsules around the joints which contain lubricating synovial fluid not found in fibrous or cartilaginous joints. Although it is possible for rheumatoid arthritis to subside, the damage caused to the surrounding synovial joint is irreversible. A comparison between a normal joint and one affected by rheumatoid arthritis is shown in fig.3. Fig.3. This diagram shows the comparison between an unaffected joint and one badly affected by rheumatoid arthritis. These were taken from the Arthritis Research UK page on Rheumatoid 6 Arthritis Research UK website: http://www.arthritisresearchuk.org/arthritisinformation/conditions/rheumatoid-arthritis/what-is-rheumatoid-arthritis.aspx 6|Page Arthritis. It can be seen clearly how the synovium becomes inflamed and invades the synovial space, causing friction that leads to irreversible damage to the cartilage and eventually bone. The inflammation of the synovium is a very similar mechanism to that seen when a wound becomes inflamed. The blood vessels dilate and become leaky, leading to an increased size and blood flow, also explaining why inflamed areas become warm to the touch. The extreme and prolonged inflammation in the joints of rheumatoid arthritis sufferers is caused by the build-up of fluid and cells in the synovium. The pain is caused by the irritation of nerve endings by chemicals, known as inflammatory cytokines, and the stretching of the capsule [6]. The most important cytokine that causes the inflammation, and therefore the clinical problems of rheumatoid arthritis, has been identified as tumour necrosis factor alpha (TNF- α). This is secreted by adipose tissue (fat). TNF- α can be described as an acute phase protein as its blood concentrations increase or decrease in response to an inflammation7. Rheumatoid arthritis is caused by the abnormal interaction between B and T cells. This involves the presentation of a perceived antigen in the synovium from B cells to T cells through HLA-DR, which is a cell surface receptor. This interaction stimulates the release of TNF- α from either B or T cells, driving the inflammation [4]. Hypersensitivity is an abnormal response to the prolonged exposure to an antigen. If TNF- α is released by B cells, rheumatoid arthritis is seen as a form of type III hypersensitivity. It is also called the immune complex mediated response. This is where the antigenantibody complexes are not completely removed by the innate immune response and so cause inflammation. If released by T cells, rheumatoid arthritis is seen as closer to Type IV hypersensitivity. This is also called delayed type hypersensitivity as it often takes a few days to develop. Unlike Type III it is cell mediated not antibody mediated, meaning that the T-cells become excessively overactive8. 7 Keffer J, Probert L, Cazlaris H, Georgopoulos S, Kaslaris E, Kioussis D, Kollias G (December 1991) Transgenic mice expressing human Tumor Necrosis Factor: a predictive model of arthritis. The EMBO journal, December 1991 8 Holmes N, Immunology Division, Department of Pathology, University of Cambridge: Lecture 14: Hypersensitivity (1999). Best Practice and Research clinical Rheumatology, 25 December 2011 7|Page Current treatments and therapies: Currently there are three main types of treatment for rheumatoid arthritis although none of them cures the condition. They are: drugs, physical therapies and surgery. The three main drug types used are: non-steroidal anti-inflammatory drugs (NSAIDs), disease-modifying anti-rheumatic drugs (DMARDs) and steroids. In most treatments, patients use a combination of drugs due to the varying effects of each type. The most common combination is a painkiller, NSAID and one or more DMARDs. NSAIDs usually give pain relieving and fever reducing effects; however, if prescribed in high doses, they also develop an anti-inflammatory characteristic. A common example of an NSAID is aspirin, often used to remove minor aches and pains [6]. DMARDs are used specifically to treat rheumatoid arthritis and are prescribed to slow the progression of the disease [6]. A current DMARD used is Leflunomide, a specific inhibitor of dihydroorotate dehydrogenase (oxidises dihydroorotic acid to orotic acid by removing two hydrogens) [3]. It is used to treat rheumatoid arthritis because blockage of this step inhibits lymphocyte activation and therefore limits inflammation. Steroids are synthetic hormones used to treat medical conditions, although the body does produce its own steroids naturally for regular functions. Unlike anabolic steroids, those most commonly talked about in the context of athletics, the type used to treat rheumatoid arthritis and other autoimmune conditions are called corticosteroids, specifically synthetic glucocorticoids [6]. Instead of promoting muscle growth, these corticosteroids help to reduce inflammation and can also be used to treat conditions such as asthma. Unfortunately, corticosteroids commonly lead to the development of Cushing’s syndrome. This is not the same as Cushing’s disease, where a tumour develops in the pituitary gland stimulating increased cortisol production from the adrenal glands. However due to high glucocorticoid levels, those prescribed with corticosteroids often develop the symptoms of Cushing’s syndrome, which include: weight gain, thinning fragile skin and stretch marks [6]. Physical therapies simply involve exercises to strengthen muscles and move joints safely; a common activity is hydrotherapy [6]. Operations vary from minor releases of nerves or tendons to whole joint replacements. Hip, knee, shoulder and elbow replacements are highly successful although they are time consuming and costly. Many operations also often carry risks of not being successful or making the sufferer’s quality of life worse than it originally was if the operation is not a success, through damaging nearby tissue. However, these risks are common to almost all operations, regardless of the target area. Major advancements in the treatment of rheumatoid arthritis have occurred over the past two decades but the search for safer and/or more efficacious treatments still remains a challenge for difficult to treat patients and those unable to tolerate currently available therapies9. 20 years ago, regulatory T cells (formerly known as suppressor T cells) were discovered [5]. This initiated a new research area for immune disorders. The growing evidence for a critical role of these cells in controlling autoimmune responses has raised expectations for therapeutic application of regulatory T cells in patients with autoimmune arthritis. ‘Treating arthritis by immunomodulation: is there a role for regulatory T cells?' reviewed recent studies investigating the presence, phenotype and 9 Dimitrios A. Pappas, MD, Assistant Professor of Medicine, Aura Geraldino- Pardilla, MD, Assistant Professor of medicine, Joan M. Bathon, MD, Professor of Medicine: Immune Modulation of Rheumatoid Arthritis. Best Practice and Research clinical Rheumatology, December 2011. 8|Page function of these cells in patients with rheumatoid arthritis and juvenile idiopathic arthritis (JIA) and the consideration of their therapeutic potential. Both direct and indirect methods to target these cells were discussed and it was concluded that a therapeutic approach that combines multiple regulatory T cell enhancing strategies could be a successful clinical approach10. Advancements in biotechnology, and increasing understanding of the immunopathogenesis of rheumatoid arthritis, have driven the development of more modern therapies for rheumatoid arthritis. Recently, important successes have been achieved, especially in the area of biologic agents targeting the main pro inflammatory cytokine TNF- α (tumor necrosis factor alpha). This has therefore launched interest in further research into other immunomodulatory therapies for this and other autoimmune systemic inflammatory disorders. With this greater understanding of the pathophysiology of these diseases, novel therapies may offer patients noticeably improved outcomes and perhaps even cure the disease entirely11. The group of immunomodulatory drugs encompasses a broad spectrum of different drugs. In short, a drug counts as an immunomodulatory drug if it in some way affects the immune system’s normal function. There are currently three different types of immunomodulatory therapies: immunostimulants, tolerogens and immunosuppressants [3]. Immunostimulants enhance the strength of the immune system’s response. This can be done specifically: for example, most vaccines are specific immunostimulants against pathogens [2]. Non-specific immunostimulants enhance the function of the entire immune system: an example of this is female sex hormones like oestrogen. Tolerogens, sometimes known as immunogens, are used to force the immune system to accept donor organs. They work by stopping the specific response from attacking perceived antigens. The current types of immunomodulation used to treat rheumatoid arthritis are predominantly nonspecific immunosuppressant drugs. The perfect form of suppressant is one targeted specifically at cytokine TNF- α, one of the main contributors in the immune system’s response to the synovial fluid. The drug Adalimumab can carry out this function, however at this time there are no immunomodulatory therapies that specifically target the interaction between the immune system and the synovium. The most common treatment now is the use of at least one immunosuppressant drug along with a whole host of other drugs aimed at stopping the side effects of a weakened immune system [6]. Extended Project Discussion: Can symptoms and signs of rheumatoid arthritis be alleviated completely by novel immunomodulatory therapies? Why is a new treatment needed? There is currently no specific drug or regimen to cure the condition of rheumatoid arthritis. A variety of drugs and physical therapies are used alongside each other to lessen the symptoms and damage caused by the disease. These can be altered depending on how severe the arthritis is, or whether 10 Ellen J. Wehrens, Femke van Wijk, Sarah T.Roord, Salvatore Albani and Berent J. Prakken: Treating arthritis by immunomodulation: is there a role for regulatory T cells? Rheumatology (Oxford, England) September 2012 11 Arthur Kavanaugh, MD, University of California, San Diego, Professor of Medicine, Director of the Centre for innovative Therapy, Division of Rheumatology Allergy and Immunology: Novel Immunomodulatory therapies for Rheumatoid Arthritis. Reumatologia March 2005 9|Page you are about to undergo surgery. An example of a regimen to treat rheumatoid arthritis is this: the drugs Humira, Methotrexate, Naproxen and folic acid12. Humira, scientifically called adalimumab, is currently the world’s largest selling drug. It is used to reduce the effect of inflammatory stimulants, predominantly TNF- α, in the blood. Adalimumab achieves this by bonding with TNF- α and preventing the interaction between TNF- α and TNF- α receptors on cell surface membranes, therefore preventing an inflammatory response. It is injected subcutaneously every other week. Although it is effective, it has many serious side effects including lymphoma, a rare cancer that has been known to affect the liver, spleen and bone marrow13. It also increases the risk of subsequent infections due to the low levels of TNF- α. Methotrexate, a DMARD, works by preventing the absorption of folic acid, a key substance needed for cell replication, therefore greatly reducing the concentration of white blood cells in the blood. This acts as an immunosuppressant as with fewer lymphocytes being produced, the immune system becomes less active and the damage of the synovium is slowed. Methotrexate is taken once or twice a week through a pill. Although this is very effective, it has many unwanted side- effects, such as vomiting, blurred vision increased risk of infection and headaches14. When prescribed with Humira, the effectiveness of Methotrexate has been seen to double. Naproxen is a NSAID, working by inhibiting the production of prostaglandins, hormone-like lipid compounds associated with causing inflammation and pain. It is taken by swallowing a pill whole for an extended release. Like both of the other drugs, Naproxen has some serious side effects including an increase in the risk of heart attack, gastrointestinal bleeding and stroke15. Folic acid (vitamin B) is taken to reduce the side effects of methotrexate. As Methotrexate is not specific it effectively inhibits the function of all ‘active’ cells, especially the immune system. Folic acid is needed by the body to replicate, repair and methylate DNA (adding a methyl, CH3, group to the bases adenine and cytosine). Taking large doses of folic acid helps to reduce the strong side effects of Methotrexate and allows cells to function without extensively preventing the effectiveness of Methotrexate’s immunosuppressant capabilities [14]. Although regimens such as this work well and are effective against the disease, they are very inconvenient and can have some very serious side effects. Despite this effectiveness, up to 50% of patients still fail to see significant clinical responses [6]. The number of pills needed to combat the lack of specificity of drugs such as Methotrexate makes it a lot of effort for sufferers to remember to take the drugs at their uneven intervals. It is also painful to have regular injections, with sufferers either having to do this themselves or travel to a doctor if they are uncomfortable or unable to do so. This means that sufferers’ lives are dictated and limited by the urgent need to take these multiple treatments when they are needed. To help these people, a more specific immunomodulatory therapy would be excellent, as it would reduce the number of tablets and injections the sufferers would have to consume to counteract the weakened immune system, thus reducing the restrictions of the regimen [12]. The reduced cost to health services and drug companies due to the need to produce fewer tablets would also be a great benefit of fewer drugs being needed to combat rheumatoid arthritis. 12 This regimen is that used by a family friend who provided information on rheumatoid arthritis and how to live with it. 13 Drugs.com Page on Humira: http://www.drugs.com/humira.html: 14 Drugs.com Page on Methotrexate: http://www.drugs.com/methotrexate.html 15 Drugs.Com Page on Naproxen: http://www.drugs.com/naproxen.html 10 | P a g e The success in treating psoriatic arthritis: Psoriatic arthritis (PA) is also an autoimmune form of arthritis, this time usually affecting sufferers of the aggressive skin condition psoriasis. It causes many of the same symptoms as rheumatoid arthritis but is very easily kept under control by the relatively new drug Apremilast, the brand name of which is Otezla. It is worth noting that while Apremilast treats psoriatic arthritis, it does not treat the existing skin condition of psoriasis. For this, patients will still need to be prescribed steroidal cream. This condition and its treatment are a very useful comparison due to psoriatic arthritis and rheumatoid arthritis both involving an autoimmune response damaging synovial joints through inflammation. The treatment for both involves the targeting of the pro-inflammatory cytokine TNFα. What is Apremilast and how is it relevant? Apremilast was first approved by the FDA for use in the USA on March 21, 201416. It is currently produced by Celgene and has the advantage of being an orally administered pill over other, injection based treatments. It works to treat the inflammatory effects of psoriatic arthritis by inhibiting the spontaneous production of TNF- α from the synovial cells, the main cytokine involved in inflammation. This is different from Adalimumab as, instead of preventing the interaction between TNF- α and the TNF- α receptor, Apremilast inhibits the enzyme phosphodiesterase 4. This then specifically prevents the production of TNF- α from synovial cells and not other types of cells in the body. There are relatively few serious side effects due to the drug not prohibiting all interactions of TNF- α. However, some patients have reported headaches and nausea. It has also been reported to have several serious interactions with other drugs like Rifampicin, used to treat tuberculosis [16]. Apremilast holds great potential for treating rheumatoid arthritis as it inhibits TNF- α in the synovial joints, therefore reducing the damaging inflammatory reaction to the synovium. It is also very attractive as it specifically targets TNF- α, instead of just dampening down the whole immune system. This allows the sufferer to only have to take a single pill (monotherapy) instead of many current regimens that involve multiple drugs. This is far easier and reduces the number of possible side effects from taking so many drugs. Why is Apremilast not used already? Although Apremilast may seem like a perfect drug to treat rheumatoid arthritis already, Celgene reported that it failed the mid-stage trial [16]. This was found using the ACR (American College of Rheumatology) scale. During phase II clinical trials, Aremilast failed to reach ACR20. This means that the drug failed to significantly improve the arthritis in 20% of the patients before the end of Phase II trials. The structure of clinical drug testing is shown in fig.4. Fig.4. This table briefly outlines the four stages of clinical trials in the testing of a new drug. This table excludes animal testing and drug development. Phase I Phase II A group of healthy human participants are given the drug to check for any unwanted side effects. A small group of human participants who suffer from the target condition are given the drug to test that it helps combat the disease. 16 John Hopkins Arthritis centre page on Apremilast: http://www.hopkinsarthritis.org/arthritis-news/psoriaticnews/apremilast-otezla-approved-by-fda/ 11 | P a g e Phase III Phase IV A large group of human participants with the target condition are given the new drug and either a placebo (inactive agent like sugar) or a current treatment. This is to show that the drug has a noticeably greater effect on the disease than current treatments. Post marketing surveillance trials to ensure the safety of the new drug. Celgene also reported that the current treatment, Methotrexate, had a weakening effect on the efficacy of Apremilast17. This was a great disappointment, especially due to its success with treating psoriatic arthritis. However, Celgene is still carrying out trials of similar drugs and hopefully these will prove to be more effective when treating rheumatoid arthritis. Due to Apremilast being developed so recently, it is not currently known why it does not work in the treatment of rheumatoid arthritis but has such success in treating psoriatic arthritis. Are novel immunomodulatory therapies the only alternative? There are other potential treatments for autoimmune diseases; some of the more promising including stem cell based treatments and gene therapy. Stem cell based therapies The use of stem cells to prevent or cure a disease is widely seen by the medical community as a highly promising area of research in the context of curing chronic diseases [3]. However, despite this, only stem cell therapies for the treatment of cancers are widely used. The most common method of collecting stem cells is through bone marrow, umbilical cords or, very rarely, foetus’ samples. This does, of course, raise some serious ethical debates. Once a culture of healthy stem cells has been collected, they are injected into the body in or around the damaged areas. The stem cells recognise the types of cells around them and allow the production of healthy, properly functioning body cells that help regrow the areas damaged by rheumatoid arthritis. The property of stem cells that make them so attractive is that they are not differentiated and so can be used to form any body cell by placing them in the area of need. Cells with this ability are called totipotent stem cells. Once in place, the stem cell will recognise the type of cell it is near and start producing new, healthy versions of that cell18. Those taken from the bone marrow are pluripotent, meaning they can differentiate into most body cells but not all. Allogeneic mesenchymal stem cells, gathered from donated umbilical cords, are multipotent stromal cells that can differentiate into bone, cartilage and fat cells19 . Stem cell therapies would result in damaged cells around joints being regenerated and the damaging permanent effects of rheumatoid arthritis being reduced. Although this is an effective treatment there are many drawbacks to it. Stem cell transplants are very expensive and complicated; this is because of the procedure that you have to go through to collect a healthy sample that is large enough. Although through the current donation of umbilical cords it is relatively easy to gather them, the stem cells must then be screened for infectious diseases [18]. They must then be manipulated or tested to make sure they are compatible before finally being administered to the patient. A compatible stem cell is one from a donor whose cells possess similar cell surface antigens to those of the patient. If the antigens are 17 Fierce Biotechs page on Apremilast: http://www.fiercebiotech.com/story/celgene-delivers-mixed-dataapremalist-preps-arthritis-app/2012-07-12 18 Mayo Clinic page on stem cell transplant, Written by and unnamed Mayo Clinic Employee: http://www.mayoclinic.org/tests-procedures/stem-cell-transplant/basics/definition/prc-20013565 19 Stem Cell Institute page on Rheumatoid arthritis: https://www.cellmedicine.com/stem-cell-therapy-forrheumatoid-arthritis/ 12 | P a g e different, the host’s immune system will recognise the cells as alien and trigger an immune response against them. This process costs a lot of money due to the length and difficulty of the procedure and is therefore not preferential as a treatment of rheumatoid arthritis [19]. It also does not do anything to stop the self-reactive tendencies in the whole body as this treatment only targets specific areas. The self-reactivity could possibly, in the future, be treated using stem cells by removing the current bone marrow stem cells and introducing new ones that can produce properly functioning lymphocytes. However this would involve a very complex operation and multiple extra drugs to help patients cope with it. Currently, stem cell treatments of rheumatoid arthritis have had reasonable success when treating animals but have so far rarely been used to treat humans [19]. If this treatment is perfected and becomes more effective and less costly then it could easily become a contender to immunomodulatory therapies in the discussion of the most effective treatment. Gene therapy: Gene therapy, like stem cell therapy, is also a treatment that has the possibility of treating a multitude of different diseases and conditions. Currently, three different methods of gene therapy are being investigated: replacing a mutated gene with its normal form, inactivating a mutated gene or introducing a healthy gene into the body to help counteract the condition. Effectively all these will result in a healthy, functional copy of the gene in question being the only type present and active thereby reducing the effects caused by the mutated copy20. The most promising of these in regards to treating rheumatoid arthritis is the replacement of the mutated gene. The idea of treating rheumatoid arthritis with gene therapy is not a new one. Current biological agents such as TNF- α inhibitors are effective but have serious limitations in the form of their dangerous side effects, leading to the need for multiple different drugs. By introducing the correct gene into the damaged joints, the immune system will then be able to regulate the levels of TNF- α and other inflammatory biological substances. In recent tests, the gene IL 1RN, the gene that encodes for IL 1Ra (interleukin 1 receptor antagonist), has been inserted in vitro into cells removed from a rheumatoid arthritis sufferer’s synovial joint. This was then tested to check for functionality before being reintroduced to the sufferer’s joints. IL 1 Ra is a protein that inhibits IL 1, a cytokine that regulates immune and inflammatory responses. The functional gene IL 1RN was inserted using a viral vector. This is a deactivated virus so as not to cause the separate problem of an infection. The use of this vector takes advantage of viruses’ unique ability to inject their genetic material into that of the host cell. This stems from their inability to reproduce on their own. By first introducing a working copy of the gene into the viral genetic material, when the virus infects the host cell and inserts its own genetic material, the working gene will also be inserted and work properly. This method has been found to produce promising results in phase 1 clinical trials, after success in treating rabbits, mice and rats21. Although this may seem like a very promising and viable solution, the main bulk of papers on this specific topic are from the late 1990s and early 2000s. There are very few recent papers that could be found covering this topic in the last 10 years, unlike those concerning stem cell treatments and immunomodulatory therapies. This is because although gene therapy is indeed a promising treatment, the technique is hard to perfect and carries certain risks with it. For example, when the virus inserts its genetic material into the host DNA, there is a chance that it inserts it in an exon, therefore disrupting a functioning gene and potentially causing more harm than good. Gene therapy 20 21 Genetics Home Reference, Page on Gene Therapy: http://ghr.nlm.nih.gov/handbook/therapy/genetherapy J D Mountz, J Chen H-C Hsu: Rheumatoid Arthritis: Safe and sound. Gene Therapy November 2005. 13 | P a g e is also exclusively being tested for serious diseases that have no other treatments, and although current treatments for rheumatoid arthritis have their flaws and limitations, they do work [20]. This implies that although in the future gene therapy may be an excellent treatment for rheumatoid arthritis, currently it is not one that is being investigated as a top priority. Are novel immunomodulatory therapies the most promising treatment? The evidence put forward by this dissertation shows clearly that immunomodulatory drugs, similar to apremilast, are a viable method for an easier and more effective treatment of rheumatoid arthritis. The inhibition of tumor necrosis factor alpha production without the hazardous compromise to the immune system will reduce both symptoms of rheumatoid arthritis and the risk of contracting diseases as a side effect. The increase in quality of life of sufferers would be significant, due to them no longer needing to take a variety of pills to help offset the damaging effect of immunosuppressive drugs. The ease of oral delivery is another of apremilast’s great advantages over adalimumab, which has to be applied through injection [13]. Despite the fact that treatment of psoriatic arthritis using apremilast has shown some side effects such as a slight increase in depression, this can be counteracted by alerting the doctor responsible for the patient of said risks. This would enable them to monitor the patient in order to identify any signs early on in their development. Although the production of drugs is expensive, the need to produce fewer drugs and a lower number of operations needed would likely reduce the overall cost of treating rheumatoid arthritis [16]. Another issue that must be considered when choosing the best potential treatment is how quickly it can be developed and made available to patients. People who suffer from rheumatoid arthritis need to be treated as soon as possible to alleviate an extended period of disease progression and to limit the time during which current treatments can prevent them from living a normal life [12]. The fact that needs to be considered is that currently no better treatment for rheumatoid arthritis exists so the questions really are: which treatment will be readily available first? And will it be the most effective? Although stem cell treatments are relatively close to becoming commonplace treatments, it is possible that there will be a lack of viable umbilical cord stem cells ready to treat the large numbers of people affected by rheumatoid arthritis. This lack of supply of stem cells may cause the cost to patients of this therapy to increase hugely in countries without a system like the NHS, or maybe restrict the number of people who can have the operation in the first place [18]. Without a reliable source of gathering these precious cells that does not rely upon donations, then stem cell therapy is perhaps not the most promising of the treatments. Also the fact that these are known to be successful but are not used in favour of current drug therapies shows they are not the treatment that is being looked for by the medical world. Gene therapy has not made it past phase 1 clinical trials and so by default is not ready [21]. Although it is promising, before a method has been found to stop the viral vector from interrupting functioning genes (although this is rare), then gene therapy will not be available. Another issue with gene therapy is that once a cell that has been injected with the functioning gene dies, then the therapy will have to be repeated to increase the number of functioning genes in the body [2]. This process disrupts the sufferers’ lives by their having to make routine trips to the hospital in order to receive a booster. With comparatively very little research being done currently into using gene therapy for rheumatoid arthritis, it is unlikely that it will be readily available in the near future. 14 | P a g e Novel immunomodulatory therapies have the bonus of patients only having to take one pill on a regular basis and so do not greatly interrupt the sufferers’ usual lives22. This also means that local chemists would possibly be able to supply the drug, avoiding the need for regular hospital visits. With the great success of Apremilast in treating psoriatic arthritis, it seems very likely that investigation into a similar drug would be the quickest route to an effective treatment for rheumatoid arthritis. There is clear evidence that a lot of research is going into developing immunomodulatory drugs to treat rheumatoid arthritis. A very recent paper reports on a similar drug to adalimumab, called golimumab, being newly available for the treatment of rheumatoid arthritis. The advantage of this drug over adalimumab is that it only needs to be injected once a month, so reducing the disruption to the patient’s life23. With regards to this information, immunomodulatory therapy targeted at TNF- α production in the synovial joints appears to be the most promising of the novel therapies of treating rheumatoid arthritis. It has the advantages of being nearer to common place use and being far more accessible to sufferers due to its nature of being a drug, making it cheaper than stem cell and gene therapy, whilst also not needing an operation or complicated injection to be delivered into the body. The only disadvantage of this therapy is that, unlike the others, it does not treat the original cause. Thymic education will still be malfunctioning, leading to mutated and self-reactive cells whilst the other therapies counteract this. Immunomodulatory therapies treat only the damaging results of this breakdown. However with proper use and taking the drug as prescribed this should not be a problem as the faulty immune system will not be able to damage the synovial joints. If prescribed after the damage to the joints has been done, an operation may be worthwhile due to the immunomodulatory therapy preventing any further damage. The development of a safe and effective immunomodulatory drug to treat rheumatoid arthritis is most likely a few years from fruition. However in 2007 a paper was published that involved the review of published literature in Medline (PubMed) on the subject of induction of antigen specific tolerance and its effect on autoimmune arthritis, including the recent work on B cell mediated tolerance from their laboratory. The years included in the review were 1975 to 2007, with a lot of the articles belonging to the period 1990 to 2007. The subject of this paper was to 'review various antigen-specific tolerogenic and immunomodulatory approaches for arthritis in animal models and patients'. This involved looking into each of the treatments’ efficacy, mechanisms of action and limitations. The relevant main, as well as cross-referenced, articles were then obtained through the links within PubMed and reviewed. The results were that antigen-specific treatment had been successful in the prevention and/or treatment of arthritis in animals, but not yet in humans. The administration of soluble antigen or an altered peptide ligand native to that organism intravenously, orally, or nasally along with the delivery of the DNA segment encoding a particular antigen by gene therapy had been the main part of immunomodulation. Later on, the methods for in vitro expansion of CD4+CD25+ regulatory T-cells were improved. It had also been discovered that interleukin-17, a pro-inflammatory cytokine that works along with TNF- α, might be a promising new therapeutic target in arthritis24. 22 Fiona E McCann, Andrew C Palfreeman, Melanie Andrews, Dany P Perocheau, Julia J,Inglis, Peter Schafer, Marc Feldmann, Richard O Williams and Fionula M Brennan: Apremilast, a novel PDE4 inhibitor, inhibits spontaneous production of tumour necrosis factor-alpha from human rheumatoid synovial cells and ameliorates experimental arthritis. Arthritis Research and therapy 2010 23 Papagoras C1, Voulgari PV, Drosos AA. : Golimumab, the newest TNF- α blocker, comes of age. Clinical and experimental rheumatology January 20 2015 24 Shailesh R. Satpute, MBBS, Malarvizhi Durai, PhD, and Kamal D. Moudgil, MD: Antigen-Specific Tolerogenic and Immunomodulatory Strategies for the Treatment of Autoimmune Arthritis. Seminars in Arthritis and Rheumatism December 2008 15 | P a g e The paper concluded that antigen-specific treatment against autoimmune arthritis is still not quite perfect. However, insights into newly discovered mechanisms of disease pathogenesis provide hope for the development of effective and safe immunotherapeutic strategies in the near future. In the 7 years since this paper was published, current immonomdulatory therapies have become the most successful and widely used treatment for rheumatoid arthritis with all current treatments involving at least one variety [16]. If this current level of development continues, it is very likely that a drug specifically designed to target TNF- α in the synovial joints of rheumatoid arthritis sufferers will soon be developed. Further Reading Whilst researching the condition and treatment of Rheumatoid arthritis, a very interesting article on a possible cure for multiple sclerosis (MS) was found. Like rheumatoid arthritis and psoriatic arthritis, multiple sclerosis is an autoimmune disease and so is similar to treat, or in this case cure. The paper comprised the research conducted by scientists in the University of Bristol, and the paper was published in the journal Nature Communications. The study involved injecting mice with a very small level of myelin, the perceived antigen that the immune system attacks, then gradually increasing the dose. Over time the mice’s immune systems became less reactive to the myelin and symptoms disappeared. This is an old concept but the researchers described it as ‘a new take on an old idea’, with them saying that the key to success was the dosage and the way the myelin was injected. They did this by preparing myelin molecules so small that they were soluble in water, therefore making them easier to deal with by the immune system25. Although one paper is not conclusive, it does at least provide extra information on the molecular mechanisms of autoimmune diseases, and at best reveals a potential cure for MS or even all autoimmune conditions. This is due to most autoimmune diseases having very similar mechanisms of self-reactivity, with the only difference usually being the antigen the immune system becomes intolerant of. The main obstacle for this treatment would then be identifying the ‘offending’ antigen, as for many autoimmune diseases it is unknown or unclear. Bibliography and Source Review 1. Brocker C, Thompson D, Matsumoto A, Nebert DW, Vasiliou V Evolutionary divergence and functions of the human interleukin (IL) gene family. Human Genomics 5 (Oct 2010) This paper was useful to help grasp the specific function and therapeutic uses of the Interleukin group of cytokines. As it was published in a scientific journal, this source will have been peer reviewed and therefore all information contained within will be valid. 25 Health Line Article: Scientists Find Off Switch for Autoimmune Diseases like Multiple Sclerosis, written by Cameron Scott, 5/9/2014: http://www.healthline.com/health-news/off-switch-for-autoimmune-diseases090514#1, Original Paper: Bronwen R. Burton, Graham J. Britton, Hai Fang, Johan Verhagen, Ben Smithers, Catherine A. Sabatos-Peyton, Laura J. Carney, Julian Gough, Stephan Strobel & David C. Wraith: Sequential transcriptional changes dictate safe and effective antigen-specific immunotherapy. Nature Communications, September 2014 16 | P a g e 2. The glossary was mostly comprised of words and definitions that could be found in the Alevel textbook: Salters –Nuffield Advanced Biology for Edexcel A2 Biology. Published by Pearson Education Limited in 2009. Due to the nature of this source being a textbook for A-level Biology, it is very likely that all information on the basic word definitions it was used for will be highly reliable. The only real problem would be that information will have been simplified. However all terms were cross referenced with other sources such as: Bablyon.com http://www.babylon.com/define/18/Biology-Terms.html. When it was found that both sources had similar and just as detailed information, it was decided that the definitions from the textbook were detailed enough. This source was also used to provide simple information on some medical techniques used throughout the dissertation. 3. John W. Baynes & Marek H. Dominiczak: Medical Biochemistry Second Edition. Published by Elsevier Mosby. (2005) The author, John W Baynes, has his MSc in both laboratory medicine and chemistry and has a doctoral degree in physiological chemistry. He clearly has a great deal of authority in the field of medical biochemistry and so information taken from his book is likely to be both valid and reliable. All information published in his book will have been edited; this is the process of review of the information by other professionals at a similar level in the same field to prevent false or misleading information from being published. This source could also be cross-referenced with other sources, particularly with 'Immune regulatory function of B cells', proving its reliability. 4. Mauri Claudia & Bosma Anneleen, Immune regulatory function of B cells (2012) Annual review of immunology, January 2012 As suggested by the title, this paper was used to extend the description of B cell function, specifically on the B cells release of a variety of cytokines. Professor Claudia Mauri and Anneleen Bosma (PhD) have published a multitude of scientific papers between them on the immune system with an emphasis on the innate immune response. As it was published in a journal, the paper will have been peer reviewed and so the source is likely to be reliable. 5. Alberts B, Johnson A, Lewis J, Raff M, Roberts K, Walter P: Molecular Biology of the Cell (2002) published by Garland science: New York. This in depth textbook on cell biology was critical in both researching and cross-referencing facts from other sources. The most useful chapters were: Chapter 24. The Adaptive Immune System and Chapter 25: Pathogens, Infection and Innate Immunity. The main author, Bruce Alberts is known most for his study of the protein complexes that enable chromosome replication in mitosis. This implies that the book is a valid source as information contained within it will likely be correct. Although this is an old book, the information taken from it is still relevant as similar information was also found in: Mauri Claudia & Bosma Anneleen, Immune regulatory function of B cells (2012) Annual review of immunology, January 2012 6. Arthritis Research UK website: http://www.arthritisresearchuk.org/arthritisinformation/conditions/rheumatoid-arthritis/what-is-rheumatoid-arthritis.aspx: A lot of the information on symptoms and treatments were taken from the Arthritis Research UK website. This website was exceedingly useful as it provided information on current treatments for rheumatoid arthritis and also the causes of symptoms. It is likely a very reliable source as, being an official organisation, Arthritis Research UK will have many 17 | P a g e sources from which to gather information which is then presented on the website. This website is kept up to date with new information or news stories almost daily. All information on the current treatments of rheumatoid arthritis could be cross-referenced with the current NHS regimens as shown on the NHS page for arthritis treatment: http://www.nhs.uk/Conditions/Rheumatoid-arthritis/Pages/Treatment.aspx. 7. Keffer J, Probert L, Cazlaris H, Georgopoulos S, Kaslaris E, Kioussis D, Kollias G (December 1991) Transgenic mice expressing human Tumor Necrosis Factor: a predictive model of arthritis. The EMBO Journal, December 1991 The experimenters found that injecting the mice with monoclonal antibodies against human TNF- α completely stopped the development of rheumatoid arthritis. This information can then be transferred to humans to create a 'predictable genetic model'. However, the results do not indicate whether this treatment will work in humans, as mice are not human and so will have slightly different physiology. Although this information comes from an old paper, it appears to still be relevant as very few articles could be found that update its information. 8. Holmes N, Immunology Division, Department of Pathology, University of Cambridge: Lecture 14: Hypersensitivity (1999) This source was used to gain extended information on hypersensitivity, specifically type IV. As this journal was published properly, it was definitely peer reviewed, and with Dr Nick Holmes researching immunity and host defences at Cambridge University, it is highly likely that this source is valid. Due to this paper being an old source, information contained within it was cross referenced with a more recent paper. The paper used for this was: Abbas, Abul K. and Andrew L. Lichtman. Basic Immunology: Functions and Disorders of the Immune System. 3rd ed. Philadelphia, PA: Saunders Elsevier, 2009. 9. Dimitrios A. Pappas, MD, Assistant Professor of Medicine, Aura Geraldino- Pardilla, MD, Assistant Professor of Medicine, Joan M. Bathon, MD, Professor of Medicine: Immune Modulation of Rheumatoid Arthritis. Best Practice and Research clinical Rheumatology, December 2011. This source gave very in-depth information on many rheumatoid arthritis treatments since the first TNF- α inhibitor was approved, whilst also containing information on possible future treatments. The main author, Prof Joan Bathon, is Professor of Medicine at Columbia University College of Physicians and Surgeons, with the two others being her assistants. From this it can be inferred that information contained within the papers will be valid and reliable. 10. Ellen J. Wehrens, Femke van Wijk, Sarah T.Roord, Salvatore Albani and Berent J. Prakken: Treating arthritis by immunomodulation: is there a role for regulatory T cells? Rheumatology (Oxford, England) September 2010 This paper reviewed recent (2010) studies on the presence, phenotype and function of T cells in patients with rheumatoid arthritis and Juvenile idiopathic arthritis. The most useful information extracted from this paper was the methods of how to target the T cells causing these diseases. Authors of this papers EJ Wehrens and F van Wijk often work together and have produced many papers on regulatory T cells, this being their first. 11. Arthur Kavanaugh, MD, University of California, San Diego, Professor of Medicine, Director of the Centre for innovative Therapy, Division of Rheumatology Allergy and Immunology: Novel Immunomodulatory therapies for Rheumatoid Arthritis. Reumatologia 21 March 2005 This paper written by Arthur F. Kavanaugh, who earned his AB (biology) at the Massachusetts Institute of Technology in Cambridge, MA and later an MD (Medicine) at St. Louis Medical School in St. Louis, MO. This implies that information used from 'Novel 18 | P a g e Immunomodulatory therapies for rheumatoid arthritis' will be reliable and valid. All information published in his paper will have been peer-reviewed; this is the process of review of a paper by other professionals at a similar level in the same field to prevent false or misleading information from being published. Information from this source could be cross-referenced with many other sources on many topics from the pathophysiology of rheumatoid arthritis to the number of people affected by it in the world. This implies that the sources are reliable. The information contained within this source is almost 10 years old, however there are many other papers referenced that follow up on this for example; Papagoras C, Voulgari PV, Drosos AA. : Golimumab, the newest TNF- α blocker, comes of age. Clinical and experimental rheumatology January 20 2015. Novel Immunomodulatory therapies for Rheumatoid Arthritis was mainly used as a point of reference as to when it was first realised that inhibiting TNF- α could potentially hold the key to treating autoimmune arthritis. 12. This regimen is that used by a family friend who provided me with personal information on rheumatoid arthritis and how they live with it. 13. Drugs.com Page on Humira: http://www.drugs.com/humira.html: This website contained a large amount of information on Humira, and other drugs involved in this dissertation. It gave very detailed information on everything from function to dosing of the drug. From this very large and seemingly accurate amount of information, it is very likely that drugs.com is a reliable source. This website will be kept up to date, taking peer reviewed data from: Micromedex, Cerner Multum, Wolters Kluwer and others. Its last update was January 15th 2015 and it has links to all its information sources. 14. Drugs.com Page on Methotrexate: http://www.drugs.com/methotrexate.html As with the Drugs.com page on Humira and Naproxen, it gave full and comprehensive detail on everything that needed to be known about Methotrexate and its function. 15. Drugs.Com Page on Naproxen: http://www.drugs.com/naproxen.html Like both other drugs.com pages, the page on Naproxen offered all information needed. 16. John Hopkins Arthritis centre page on Apremilast: http://www.hopkinsarthritis.org/arthritis-news/psoriatic-news/apremilast-otezla-approvedby-fda/ Johns Hopkins University is located in Baltimore, Maryland and U.S. News & World Report has ranked the Arthritis Centre number 1 for Rheumatology in the USA. From this it is clear that research and publishing from this source on the topic of Arthritis are likely to be reliable. The information taken from this source was used to help understand the nature of Apremilast, how it is currently used and when it was approved for use. 17. Fierce Biotechs page on Apremilast: http://www.fiercebiotech.com/story/celgene-deliversmixed-data-apremalist-preps-arthritis-app/2012-07-12 This page contained an article written by John Carroll summarising Celgene’s report on Apremilast’s success in treating psoriatic and rheumatoid arthritis. Carroll has 36 years of Biotech analysis experience and is clearly a reputable reporter both within the fierce biotech network and outside. His report on Apremilast clearly outlined the success with psoriatic arthritis and how this was not mirrored in rheumatoid arthritis, whilst giving sufficient detail on why this is the case and how it is not a dead end. 19 | P a g e 18. Mayo Clinic page on stem cell transplant, Written by and unnamed Mayo Clinic Employee: http://www.mayoclinic.org/tests-procedures/stem-cell-transplant/basics/definition/prc20013565 Mayo Clinic is a US hospital with a high reputation. It has a page dedicated to its research where it can be seen that all work is peer reviewed and published in scientific journals. This page was very useful to grasp the basic concept of how stem cell therapies worked, although it was in a general context not in that of RA. 19. Stem Cell Institute page on Rheumatoid arthritis: https://www.cellmedicine.com/stem-celltherapy-for-rheumatoid-arthritis/ This page was used to help understand the concepts behind the possibility and reality of treating rheumatoid arthritis with stem cell therapies. The Stem Cell Institute Panama is one of the world’s leading stem cell research facilities. As both research and operations based, they are well equipped to provide information on the methods, risks and successes of stem cell treatments across the board. The information from this source was useful to help put stem cell treatments into context and realize how rare they are currently, with the Stem Cell Institute of Panama having only conducted 2000 treatments in the last 9 years. 20. Genetics Home Reference, Page on Gene Therapy: http://ghr.nlm.nih.gov/handbook/therapy/genetherapy The Genetics Home Reference website is a service provided by the U.S. National Library of Medicine, meaning it is a government owned website. This organization is extremely reputable, with it also owning PubMed, the online database used to find medical papers. The page on Gene Therapy gave an overview of the three main areas of research as well as why replacement of the gene with a healthy one is the most promising, and also why gene therapy is not a large area of research at the moment. 21. J D Mountz, J Chen, H-C Hsu: Rheumatoid Arthritis: Safe and sound. Gene Therapy November 2005. This paper briefly outlined the method and results gathered from a trial of using Gene Therapy to treat RA. The Division of Clinical Immunology and Rheumatology, Department of Medicine, University of Alabama at Birmingham employs all three of the authors who worked on this paper. 22. Fiona E McCann, Andrew C Palfreeman, Melanie Andrews, Dany P Perocheau, Julia J. Inglis, Peter Schafer, Marc Feldmann, Richard O Williams and Fionula M Brennan: Apremilast, a novel PDE4 inhibitor, inhibits spontaneous production of tumour necrosis factor-alpha from human rheumatoid synovial cells and ameliorates experimental arthritis. Arthritis Research and therapy 2010 This paper contained results from early tests of Apremilast on mice, however it was used mostly to illustrate the advantages Apremilast has over current treatments such as Adalimumab. As it is a scientific paper published in a respectable journal, its information is likely to be valid and reliable. The corresponding author, Fiona E McCann, is employed at the Nuffield Department of Orthopaedics, Rheumatology and Musculoskeletal Sciences at Oxford University. 23. Papagoras C, Voulgari PV, Drosos AA. : Golimumab, the newest TNF- α blocker, comes of age. Clinical and experimental rheumatology January 20 2015 This paper was published only a week before the final hand in date for the dissertation. It was used mainly to show how there appears to be a greater level of research into immunomodulatory therapies for the treatment rheumatoid arthritis compared to that of 20 | P a g e gene therapy and stem cell therapy. As it was published in a scientific journal it will have been peer reviewed and so the information contained will be reliable. 24. Shailesh R. Satpute, MBBS, Malarvizhi Durai, PhD, and Kamal D. Moudgil, MD: AntigenSpecific Tolerogenic and Immunomodulatory Strategies for the Treatment of Autoimmune Arthritis. Seminars in Arthritis and Rheumatism December 2008. This paper involved the review of many different papers found on PubMed. It is therefore very high in validity as all sources used to gather information will individually have been peer-reviewed as well as the final paper published. As all authors have earned qualifications like MMBS, PhD and MD it is very likely that the paper contains valid information. All information in this review could be cross-referenced with the original sources found on PubMed. 25. Health Line Article: Scientists Find Off Switch for Autoimmune Diseases like Multiple Sclerosis, written by Cameron Scott, 5/9/2014: http://www.healthline.com/health-news/offswitch-for-autoimmune-diseases-090514#1, Original Paper: Bronwen R. Burton, Graham J. Britton, Hai Fang, Johan Verhagen, Ben Smithers, Catherine A. Sabatos-Peyton, Laura J. Carney, Julian Gough, Stephan Strobel & David C. Wraith: Sequential transcriptional changes dictate safe and effective antigen-specific immunotherapy. Nature Communications, September 2014. Review of PubMed PubMed was the one of the most invaluable resources for finding information used in this dissertation. It is an online search engine owned by the National Centre for Biotechnology Information, U.S. National Library of Medicine and contains over 24 million citations from biomedical literature with links to the original documents. The ease by which reliable scientific papers on the treatment of rheumatoid arthritis can be found is really what makes this source stand out above the rest. All papers contained will originally have been published in scientific journals, for example: Clinical and experimental rheumatology. This means they will all have been peer reviewed and, by displaying this, PubMed gives all the information required for proper citations. Whilst not all scientific papers were found on PubMed, the vast majority were. The quality of this resource is shown by how up to date it is kept and how easy it is to find relevant sources. A few papers have been published in recent weeks that describe progress in the development of immunomodulatory therapy for rheumatoid arthritis, for example source 23: Golimumab, the newest TNF- α blocker, comes of age. This source could only be found because of PubMed’s incredible versatility. 21 | P a g e