Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
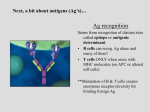
Elevating the Process of Clot Regulation GRAFTON HIGH SCHOOL The Role of Endothelial Protein C Receptor in Blood Clotting and the Immune System Grafton SMART Team: Lisa Borden, Mariah Fox, Sean Gasiorowski, Grace George, Lucas Mullens, Emily Volkmann, Jacob Zirbel Advisor: Dan Goetz, Fran Grant Mentor: Andrea Ferrante, M.D. Abstract The coagulation of blood is essential to normal bodily function, but is especially important upon blood vessel injury. An excess of coagulation can lead to complications as well. One regulatory mechanism between pro- and anti-coagulant mechanisms involves Protein C. Protein C assists in the regulation of blood clotting by acting in a negative feedback response to the production of thrombin, a protein with procoagulant activity in the serum. Thrombin loses its procoagulant functions when it interacts with a membrane-bound protein expressed on endothelial cells called thrombomodulin. The thrombin/thrombomodulin complex promotes conversion of Protein C into Activated Protein C (APC). If protein C binds to the thrombin/thrombomodulin complex in the presence of endothelial protein C receptor (EPCR), the rate of this activation increases twentyfold. As a soluble molecule in the bloodstream, APC functions as an anti-coagulant factor. When APC remains bound to EPCR, the APC/EPCR complex can interact with the receptor protein, Protease-activated Receptor 1 (PAR1), resulting in decreased tissue damage during inflammation. Because EPCR is similar in structure to the Major Histocompatibility Complex (MHC), an important receptor in activating an immune response by presenting antigens to T-cells, it may have a similar function. While the MHC binds to peptides to perform its immune activation function, EPCR is thought to bind to lipids and may potentially be involved in cytoprotective mechanisms during sepsis. Because of its importance in blood clotting and its possible immune function, the Grafton High School SMART (Students Modeling A Research Topic) Team chose to model EPCR using 3D printing technology. The Importance of Clot Regulation Within the United States, 140,000 people die from strokes each year1. This statistic, coupled with the common occurrence of heart attacks, demonstrates the importance of blood clot regulation. While these disorders are caused by an excess of clotting, hemophilia and other similar disorders are prime examples of the dangers of too little clotting. As such, it is important for the body to have a finely controlled and properly functioning mechanism for maintaining homeostasis in the bloodstream. The functioning of a few specific molecules is crucial to this homeostatic condition, as well as to the prevention of widespread development of clotting disorders and the preservation of human life. Protein C Activation Possible Immune Function The interaction of Protein C with the thrombin/thrombomodulin complex is weak. Without EPCR, it interacts only when the chance of “bumping” into the thrombin/thrombomodulin complex is higher, such as in small blood vessels. EPCR allows this close contact to occur anywhere in the bloodstream, specifically in larger vessels, and greatly facilitates the molecular interaction. • The immune system operates through the activation of various processes in response to the physical-chemical features of “trigger” particles known as antigens. • The Major Histocompatibility Complex (MHC), is a molecule responsible for presenting antigens to T-cells (a subset of white blood cells). If T cells exist that can recognize that particular antigen/MHC complex, an antigen-specific immune response is initiated. • EPCR and MHC have similar shapes, which would suggest a similar function. • However, there is no conclusive evidence for such a potential immune function. Structural Comparison of MHC and EPCR 1 www.strokecenter.org/patients/about-stroke/stroke-statistics Influence of EPCR on Protein C The Protein C Anticoagulant Pathway • This graph shows the effect of EPCR on the rate A of Protein C activation (APC). • The data was gathered by measuring the rate of activation at various concentrations of Protein B C using phosphatidylcholine vesicles (structures similar to cells) that contained thrombomodulin. Activation rate was measured both with and without EPCR. • It can be seen that the rate of production of Activated Protein C with EPCR (line A = ▵) is faster than the rate without EPCR (line B = ○). Key: The third line (line ●) does not pertain to the In the presence of EPCR = Line A (▵) focus of this poster. In the absence of EPCR = Line B (○) Steps preceding the anticoagulation response of Protein C: 1. Vascular injury or endotoxin/inflammatory cytokines 2. Initiation of coagulation cascade 3. Generation of thrombin, formation of blood clot 4. Thrombin binds to thrombomodulin on endothelial cells Activated protein C (APC), a physiological anticoagulant, is generated from the inactive precursor protein C "on demand" in response to thrombin formation. Briefly, vascular injury or endotoxin/inflammatory cytokines initiates the coagulation cascade, ultimately resulting in thrombin generation and blood clot formation. Excess thrombin then triggers the protein C pathway which provides feedback inhibition of coagulation. The protein C pathway is initiated when thrombin (T) binds to thrombomodulin (TM) on the endothelial cell surface. The thrombin-thrombomodulin complex rapidly converts zymogen protein C (PC) to its active form APC. Protein C activation is augmented by the endothelial cell protein C receptor (EPCR) which binds circulating protein C and presents it to the thrombin-thrombomodulin complex. APC then dissociates from EPCR and, in combination with its cofactor protein S (S), acts as an anticoagulant by degrading factors Va and VIIIa, key cofactors in coagulation. Adapted from diagram in Lisa J. Toltl, Lucy Y.Y. Shin, Patricia C. Y. Liaw. (2007) Activated protein C in sepsis and beyond: Update 2006. Frontiers in Bioscience 12, 1963-1972 3HLJ.pdb 1L8J.pdb MHC EPCR As visible in the above figure, MHC proteins and EPCR feature a striking structural similarity. MHC molecules have a membrane-proximal domain, which allows for the “anchoring” of the protein to the membrane, and a membrane-distal domain, which is the known peptide binding site. Here, the binding site is shown from the top, as a T cell would “see” it with its receptor. This binding site is a groove formed by two parallel alpha-helices and a floor of beta-sheets. ©1999 by American Society for Biochemistry and Molecular Biology The Structural Basis of EPCR Activity • Glu86 (Dark Green) binds to Ca2+ ions on Protein C to facilitate activation • Thr157, Leu82 (Green) and Tyr154 (Light Blue) create a network of hydrophillic interactions with Protein C • Gln150 and Arg87 (Blue) create hydrogen bonds with Protein C 1L8J..pdb Conclusion EPCR is a vital part of the blood clotting process. Without EPCR, people would be more susceptible to thrombosis and cardiovascular events. Thus, EPCR constitutes a crucial molecule for the maintenance of blood homeostasis. In addition, the structural similarities between Endothelial Protein C Receptor and the Major Histocompatibility Complex may be an indication of a potential immune function for EPCR. Addressing this hypothesis would further enhance our understanding of the immune system and lead to an increased ability to treat diseases. Oganesyan, Vaheh. "The Crystal Structure of the Endothelial Protein C Receptor and a Bound Phospholipid."Journal of Biological Chemistry. 277.28 (2002): 24851-24854. Print. A SMART Team project supported by the National Institutes of Health Science Education Partnership Award (NIH-SEPA 1R25RR022749) and an NIH CTSA Award (UL1RR031973).