Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Immune system wikipedia , lookup
DNA vaccination wikipedia , lookup
Adaptive immune system wikipedia , lookup
Psychoneuroimmunology wikipedia , lookup
Anti-nuclear antibody wikipedia , lookup
Adoptive cell transfer wikipedia , lookup
Immunocontraception wikipedia , lookup
Innate immune system wikipedia , lookup
Molecular mimicry wikipedia , lookup
Cancer immunotherapy wikipedia , lookup
Polyclonal B cell response wikipedia , lookup
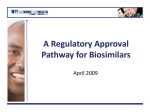
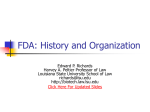
ORIGINAL ARTICLE P E E R-R EVI EW E D L. Revers An introduction to biologics and biosimilars. Part I: Biologics: What are they and where do they come from? Leigh Revers, MA, DPhil; Eva Furczon, HBSc, MBiotech E. Furczon We wrote this article because we recognize a need for today’s generation of pharmacists to become better informed about the history of biologics, and to learn how they differ from the more conventional small-molecule drugs that are prevalent in pharmacopeias. Nous avons rédigé cet article, car nous reconnaissons que les pharmaciens d’aujourd’hui doivent mieux connaître l’histoire des produits biologiques et savoir en quoi ils diffèrent des médicaments traditionnels à petites molécules, si fréquents dans la pharmacopée actuelle. 134 Introduction In recent times, the term biologics has come to be synonymous with a new class of protein-based therapeutics that are produced using living organisms, including plants, animals and microorganisms such as yeast and bacteria. Compared to the more traditional drugs, such as Aspirin, this new class of medicine is inherently more complex and cannot be synthesized in the laboratory by chemical means alone. Given the intricate nature of biologics, it is important that pharmacists become well informed about the origins of these new therapeutics and how they differ from conventional, small-molecule drugs. This review is the first in a two-part series on biologics. In Part I, we seek to define biologics and briefly examine their heritage. In Part II, featured in the next issue, we will explore the diversity of biologics and discuss the challenges for “follow-on,” or generic, versions known as biosimilars. The goal of both articles is to introduce the fundamentals of biologics and to explain how they are different and what these differences mean for pharmacists. In search of a definition The use of the expression biologics has become commonplace in the language of the pharmaceutical industry.1 It is most often used (imprecisely) to describe the new wave of protein-based therapeutics, predominantly the monoclonal antibodies (MAbs), which are among the fastest-growing medicines today. But what exactly is a biologic? The rather surprising answer is that even in 2010 there remains considerable confusion as to what does or does not constitute a biologic. In this article, we will present some of the plausible definitions. Furthermore, we maintain that the term only really makes sense if you understand where it comes from. Our brief survey of the history of biologics in Part I will set the stage for a more indepth discussion in Part II of some of the unique challenges faced by today’s major pharmaceutical manufacturers, as well as by their rivals, the generic drug manufacturers. In particular, an understanding of these challenges will illuminate the growing debate surrounding the emerging class of drugs known as biosimilars — a term coined to describe generic, or “follow-on,” biologics that will compete with the established big-name brands once their patents expire.2 Our first inkling of a meaning for the term biologics comes from the word itself: an adjectival noun originating from biology, the science of living organisms. In the narrower context of pharmaceuticals, this lends itself to the concept of biologic as a way to describe any of a class of medicines in which the active pharmaceutical ingredient (API) comes from a living organism. This would include substances obtained from plants and animals as well as from microorganisms such as yeast and bacteria. It would also cover human blood products and even tissue transplants. Such a simple demarcation is rather broad, however. Plants, in particular, produce a myriad of molecules with well-established pharmaceutical value — among them products as diverse as salicin, the penicillins, quinine, digoxin and paclitaxel — that are conventionally termed “natural products,” and these are clearly not bioC P J / R P C • M AY / J U N E 2 0 1 0 • V O L 1 4 3 , N O 3 logics according to the industry’s accepted vernacular. The reasoning behind omitting natural products from the biologics roster is obvious when you realize that commercialization of such medicines relies on their bulk manufacture using industrialscale chemical synthesis, so, in that sense, they are synthetic, not biologic. Indeed, the entire pharmaceutical business is built squarely on the capabilities of medicinal chemists to synthesize such drug molecules with relative ease. A tighter definition, then, is that biologics are APIs derived from living organisms that cannot reasonably be synthesized by chemical means. This is far better, but it also begs the following question: Which molecules today are chemists unable to make? The rather roundabout answer to that is just about any biological molecule or mixture of biological molecules that is too complex; for example, proteins or large pieces of DNA or even intact whole cells and tissues from organisms. Hence, all vaccines are biologics, as are insulin, blood factors such as coagulation factor VIIa (NovoSeven RT) and epoetin alfa (EPOGEN), and all of the therapeutic MAbs, such as trastuzumab (Herceptin) and rituximab (Rituxan). These molecules of biological origin, sometimes called macromolecules, are simply far too complicated to be prepared by chemical synthesis alone; instead, we must farm living organisms to produce them for us. Yet, we find that even this “beyond-chemicalreach” definition fails to address the underlying molecular properties that distinguish biologics from conventional medicines. Furthermore, biologics today have become inextricably intertwined • The application of biotechnology to produce with biopharmaceuticals, modern medicines or “biologics” began about to the point where they are 40 years ago when the techniques of recomsynonymous. As an alterbinant technology were first put into practice. native, then, you need only • Since then a number of increasingly complex consider 2 properties of an biologic drugs have been approved for the API when deciding from treatment of patients worldwide. first principles whether • It is important for pharmacists to know the or not it is a biologic: the origins of these new therapeutics and how first is the relative molecuthey differ from conventional, small-molecule lar size of the API, and the drugs. second, its compositional uniformity. The relative molecular mass (Mr) is the molecular mass of a substance relative to 1/12 the mass of an atom of carbon-12. The relative molecular mass, and by direct relation, the size, is a primary defining feature of any molecule, yet, amazingly, this often goes unappreciated and is not specified on drug labels. In a very real sense, size is everything in the world of molecular medicine. Why? Because all APIs are information carriers. This information takes the form of the drug’s unique 3-dimensional shape, a shape defined by its underlying molecular structure, and the complexity of that information is size-dependent and, therefore, mass-dependent. The bigger the molecule, the greater the number of atoms that make up its structure and the more complex and information- Key points Molecular size comparison of a small molecule drug (Aspirin) to 3 different classes of biologics* FIGURE 1 *Relative molecular masses are shown in parentheses. Images: Molecule of the month, adapted with permission from the RCSB Protein Data Bank website, with attributions to David Goodsell.3 C P J / R P C • M AY / J U N E 2 0 1 0 • V O L 1 4 3 , N O 3 135 rich it becomes and hence the more biologically sophisticated. The flipside of this coin is equally significant: bigger, more complex APIs are less portable than their smaller cousins. In a patient, small molecules administered intravenously can travel just about anywhere unimpeded, almost always unnoticed by the immune system. However, bulkier APIs encounter barriers, such as membranes, that can block their entrance into cells or across the blood-brain barrier, and they are much more likely to trigger an immune response. To gain perspective on the relative sizes of different molecules, we need only compare common Aspirin, with an Mr of 180, to some archetypal biologics (Figure 1).3 Insulin, a simple biologic, has an Mr of 5808, over 30 times larger than Aspirin; the hormone erythropoietin has an Mr of 30,400, which is 5 times larger again; and MAbs weigh in at an enormous 150,000, another 5 times larger. Biologics, then, are molecular heavyweights — comparing Aspirin to a MAb is like comparing a 2 kg bag of sugar to an average-size family car. Thus, as a rule of thumb, we suggest defining a biologic as any API that is 5 or more times larger than Aspirin (i.e., with an Mr > 1000). There are provisos to this. First, we must exclude synthetic biopolymers, molecules with highly repetitive structures, because these are readily manufactured by chemists. We also prefer to avoid including vaccines because, although FIGURE 2 136 strictly falling under the biologics umbrella, the field of vaccines, like that of natural products, is already well established and has been reviewed elsewhere.4,5 The second characteristic property of biologics is the possibility of molecular diversity. Small APIs are uniform in their composition because they are chemically synthesized with precise control, and any contaminants or unwanted side products can be purified away. This is not true of biologics, which often comprise a wide range of closely related variants or are intentionally a mixture of different biomolecules. We will revisit this topic of heterogeneity in greater detail later in Part II, but now that we have some working definitions for biologics, we will review some of the historical milestones behind their rise to prominence. A glimpse into the history of biologics Biologics are a 20th-century development (Figure 2).6-10 The isolation of the first-ever biologic, the hormone insulin, was achieved by Frederick Banting and Charles Best in Toronto in 1921.11,12 Insulin (from the Latin insula) is named for the islets of Langerhans in the pancreas, which secrete the hormone. Banting and Best isolated the substance from the pancreatic ducts of dogs and later used it to correct the inborn insulin deficiency in type 1 diabetic patients. Several decades later, in Timeline: Biologics development 6-10 C P J / R P C • M AY / J U N E 2 0 1 0 • V O L 1 4 3 , N O 3 1955, it was identified by Frederick Sanger as a protein composed of 51 amino acids, with an Mr of 5808.13 The molecule is an archetype for the socalled replacement therapy category of biologics, in that it is introduced into the body to correct a physiological deficiency. While extraction of insulin from the pancreas of cattle and pigs quickly became a commercial success,5 it was soon apparent that there were allergic complications in some people, because insulin is large enough to be monitored by the immune system. In these cases, the subtle difference between the human and animal forms of insulin caused the latter to be recognized as foreign. The real breakthrough in insulin production came with the advent of recombinant DNA technology, first described by Herbert Boyer and Stanley Cohen and colleagues in 1973.14 After hearing about Boyer and Cohen’s breakthrough, a venture capitalist by the name of Robert Swanson placed a call to Boyer and requested a meeting.15 Famously, Boyer agreed to give Swanson 10 minutes of his time.16 Swanson’s enthusiasm for the technology and his faith in its commercial viability was contagious, and the meeting extended from 10 minutes to 3 hours; by its conclusion, the world’s first biotechnology company, Genentech, was born. Using Boyer and Cohen’s techniques, a team at Genentech was able to introduce the human C P J / R P C • M AY / J U N E 2 0 1 0 • V O L 1 4 3 , N O 3 insulin gene into bacteria, enabling the isolation of biosynthetic insulin that was indistinguishable from human insulin. Though • Le recours à la biotechnologie pour fabriquer Swanson and Boyer faced des médicaments modernes ou « produits skepticism from both the biologiques » a débuté il y a 40 ans avec academic and business l’utilisation des techniques de recombinaison communities, by 1982, in génétique. partnership with pharma• Depuis lors, un certain nombre de médicaceutical giant Eli Lilly, they ments biologiques de plus en plus complexes ont had succeeded in obtainété approuvés pour le traitement de patients à la ing the FDA’s approval for grandeur de la planète. the drug, which has been • Il est important que les pharmaciens connaismarketed successfully ever sent l’origine de ces nouvelles thérapies, ainsi que since under the trade name ce qui les distingue des médicaments traditionHumulin. In 2008, Lilly nels à petites molécules. reported collective sales of US$2.8 billion17 for its family of recombinant insulin products, which includes both the Humulin range and Humalog, a more recent insulin variant. The second biologic essential to our story is another hormone, erythropoietin (EPO). It too is a replacement therapy. EPO is a blood factor that regulates red blood cell production, and its existence was first postulated in 1906 by Paul Carnot in Paris based on transfusion experiments he conducted in rabbits.18 By the middle of the 20th century, it was found that rats breathing a low-oxy- Points clés 137 gen atmosphere had elevated levels of EPO in their blood, and, by the 1960s, the hormone was discovered to originate from the kidneys. Human EPO was first purified from human urine by Eugene Goldwasser and his team at the University of Chicago in 1977.19 Subsequently, the limited quantities available were used to successfully treat patients with anemia. EPO has since been identified as a glycoprotein — a protein with chains of sugar molecules attached to it — with a molecular mass of 30,400. It comprises a 165 amino acid polypeptide with 4 sugar side chains. EPO circulates in the blood plasma at a very low concentration (about 5 picomolar). The presence of the sugar components is of particular interest, because they are essential to the molecule’s biological activity and because they highlight that biologics can have added layers of complexity beyond just protein structure.20 Amgen Inc. became the first company to isolate and patent the human gene responsible for making EPO and to reproduce the drug in large quantities by inserting the gene into hamster ovary cells. The company brought the resulting recombinant drug to market in 1989 under the trade name Epogen, despite a bitter legal battle with rival Genetics Institute, Inc., over alleged patent infringements. Today, 3 main variants of EPO are available to patients in North America: Amgen’s Epogen and Aranesp, and Johnson & Johnson’s Procrit. Amgen’s advances with Epogen and related molecules such as the granulocyte colony-stimulating factor filgrastim (Neupogen) ran in parallel with the emergence of the second major category of biologics, the MAbs. The first MAb, Ortho Biotech’s muromonab-CD3 (Orthoclone), was approved by the FDA in 1986.21 The original concept of antibodies (more correctly termed immunoglobulins) as molecules that bind to specific targets, or antigens, emerged at the turn of the 19th century through the pioneering work of Paul Ehrlich, Emil von Behring and Shibasaburo Kitasato, and Karl Landsteiner.22 In the second half of the 20th century, it became clear that antibodies consisted of an extremely diverse family of glycoproteins circulating in blood with molecular masses of approximately 150,000. MAbs are comprised of not 1, but 4 polypeptides — 2 heavy and 2 light chains — interwoven into a Y-shaped structure, as first postulated by Rodney Porter in 1962.23 Like EPO, antibodies are proteins with sugar side chains, although in lesser proportion. The first therapeutic antibodies were obtained by von Behring as far back as 1890, in the form of serum from animals that had been immunized with a suitable antigen.9 The antisera contained 138 polyclonal antibodies — a mixture of immunoglobulins, only some of which were active against the antigen — that were capable of neutralizing invading pathogens in acute disease as well as acting prophylactically. But the immune system’s response to the antisera triggered a range of side effects (called serum sickness) that were potentially life-threatening. The modern discovery that revolutionized antibody therapy came 85 years later, in 1975, when César Milstein and Georges Köhler, working together in Cambridge, UK, developed a relatively simple method for custom-producing antibodies in the laboratory.24 They fused together B lymphocytes, the white blood cells that generate antibodies, with immortal myeloma (cancer) cells from bone marrow, inventing a new type of cell that they called a hybridoma. The hybridoma inherited both the lymphocyte’s ability to produce antibodies and the cancer cell’s capacity for endlessly dividing and proliferating. Careful segregation of the hybridomas, so as to isolate only those individual cells capable of producing the most specific antibodies to a given antigen, allowed access to an inexhaustible supply of antibodies that were no longer a mixture of molecules with differing antigen specificities. The monoclonal antibody, or MAb, had arrived. Yet again, there were complications. The large size of these molecules and their recognition as foreign invaders by the immune system almost ended in premature disaster.25 This stemmed from the fact that hybridoma technology relied on mouse cells to produce the desired MAbs, which the human immune system could discriminate as non-self molecules. More recent advances in the technology have led to the development of part-mouse, part-human MAbs called chimeras (e.g., rituximab [Rituxan] and cetuximab [Erbitux]), as well as humanized antibodies (e.g., trastuzumab [Herceptin] and bevacizumab [Avastin]) that contain a bare minimum of non-human amino acid sequences. In 2002, the first completely human therapeutic MAb, Abbott’s adalimumab (Humira), received market approval. Usually, the more human the MAb, the better, although some argue that immune reactions triggered by foreign MAb components can be beneficial, particularly in oncology.6 Today, there are over a dozen MAbs, with collective oncology market sales in 2006 of over US$7.8 billion and sharp growth predicted over the next decade.6 We will only briefly mention the third and final category of biologics. These are the “hybrid” biologics, such as MAb conjugates and protein fusions: APIs that comprise 2 or more different molecules C P J / R P C • M AY / J U N E 2 0 1 0 • V O L 1 4 3 , N O 3 with different biological functions linked together. Sometimes this approach can be as conceptually straightforward as weaponizing an MAb by attaching a suitable “warhead,” such as a radioactive element (e.g., yttrium-90, iodine-131) that delivers a deadly, short-range burst of radiation only to those cells targeted by the antibody. Examples of such radiolabelled MAbs include ibritumomab tiuxetan (Zevalin) and tositumomab (Bexxar).26 Another related strategy involves weaponizing the MAb by chemical linkage to a bacterial toxin, such as calicheamicin, in order to specifically target antigenpresenting cancer cells, as in the case of Wyeth’s gemtuzumab ozogamicin (Mylotarg). A more sophisticated paradigm is Eisai Inc.’s denileukin diftitox (ONTAK), which is an example of a protein fusion between the enzymatically active portion of the diphtheria toxin and the human cytokine interleukin-2 (IL-2).27 The resulting chimeric molecule can bind to the IL-2 receptor and introduce the diphtheria toxin into cancer cells that present these receptors, killing the cells. These biologics are the subject of most recent research and are expected to be areas of considerable growth in the future. End of Part I We have chosen in this brief review to describe what we believe the term biologics has come to mean and to highlight a few of the most significant advances that have defined this emerging field in recent times. In Part II, we will explore the unique diversity of biologics, where that diversity comes from and why it is one of the foremost topics in the present drug development climate. From the Master of Biotechnology Program, University of Toronto, Toronto, Ontario. Contact leigh.revers@ utoronto.ca. References Acad Sci USA 1973;70(11):3240-4. 1. Ropp KL. Just what is a biologic, anyway? FDA Consumer 15. Goeddel DV, Levinson AD. Obituary: Robert A. Swanson 1993;27(3). (1947–99). Nature 2000;403(6767):264. 2. Covic A, Kuhlmann M. Biosimilars: recent developments. Int 16. Abate T. The birth of biotech: how the germ of an idea Urol Nephrol 2007;39(1):261-6. became the genius of Genentech. San Francisco Chronicle. 2001 3. Protein Data Bank. A resource for studying biological mac- April 1. Available: http://articles.sfgate.com/2001-04-01/busi- romolecules. Available: www.pdb.org/pdb/home/home.do ness/17593472_1_herb-boyer-genentech-s-south-san-fran- (accessed May 4, 2009). cisco-bay-area (accessed April 23, 2009). 4. Waldman TA. Immunotherapy: past, present and future. Nat 17. Eli Lilly & Company. Annual report. Indianapolis (IN): Eli Med 2003;9(3):269-77. Lilly & Company; 2008. 5. Plotkin SA. Vaccines: past, present and future. Nat Med 18. Jelkmann W. Erythropoietin after a century of research: 2005;11 Supp 4:S5-11. younger than ever. Eur J Haematol 2007;78(3):183-205. 6. Gricks C, Cann CI, Merrin A. Antibody therapies in oncology. 19. Miyake T, Kung CK, Goldwasser E. Purification of human Waltham (MA): Decision Resources, Inc.; Jun 2008. erythropoietin. J Biol Chem 1977;252(15):5558-64. 7. Westphal NJ, Malecki MJ. Biosimilars 2007–2017: shifting 20. Dordal MS, Wang FF, Goldwasser E. The role of carbohydrate payer and physician opinion increases the hurdles to uptake. in erythropoietin action. Endocrinology 1985;116(6):2293-9. Waltham (MA): Decision Resources, Inc.; 2008. 21. Smith S. Ten years of Orthoclone OKT3 (muromonab- 8. Biotechnology Institute. Historical events in biotechnology. CD3): a review. J Transpl Coord 1996;6(3):109-19. Available: www.biotechinstitute.org/what_is/timeline.html 22. Kaufmann SH. Immunology’s foundation: the 100-year (accessed May 2, 2009). anniversary of the Nobel Prize to Paul Ehrlich and Elie Metch- 9. Nobelprize.org. Emil von Behring: the founder of serum ther- nikoff. Nat Immunol 2008;9(7):705-12. apy. 2001 Dec 3. Available: http://nobelprize.org/nobel_prizes/ 23. Steiner LA. Rodney Robert Porter (1917–1985). Nature medicine/articles/behring/index.html (accessed May 11, 2009). 1985;317(6036):383. 10. Glassman RH, Sun AY. Biotechnology: identifying advances 24. Köhler G, Milstein C. Continuous cultures of fused from the hype. Nat Rev Drug Discov 2004;3(2):177-83. cells secreting antibody of predefined specificity. Nature 11. Sneader W. History of insulin. Encyclopedia of life sciences. 1975;256(5517):495-7. 2001 April 25. Available: http://mrw.interscience.wiley.com/ 25. Ezzell C. Magic bullets fly again. Sci Am 2001;285(4):34-41. emrw/9780470015902/els/article/a0003623/current/abstract? 26. Goldsmith SJ. Radioimmunotherapy of lymphoma: Bexxar hd=All,w&hd=All,sneader (accessed March 11, 2010). and Zevalin. Semin Nucl Med 2010;40(2):122-35. 12. Rosenfeld L. Insulin: discovery and controversy. Clin Chem 27. Manoukian G, Hagemeister F. Denileukin diftitox: a novel 2002;48(12):2270-88. immunotoxin. Expert Opin Biol Ther 2009;9(11):1445-51. 13. Strettona AO. The first sequence: Fred Sanger and insulin. Genetics 2002;162(2):527-32. 14. Cohen SN, Chang AC, Boyer HW, Helling RB. Construction of biologically functional bacterial plasmids in vitro. Proc Natl C P J / R P C • M AY / J U N E 2 0 1 0 • V O L 1 4 3 , N O 3 139