Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Generalized anxiety disorder wikipedia , lookup
Community mental health service wikipedia , lookup
Psychiatric and mental health nursing wikipedia , lookup
Mental health professional wikipedia , lookup
Diagnostic and Statistical Manual of Mental Disorders wikipedia , lookup
Deinstitutionalisation wikipedia , lookup
Mental disorder wikipedia , lookup
Classification of mental disorders wikipedia , lookup
Bipolar II disorder wikipedia , lookup
History of psychiatric institutions wikipedia , lookup
Mental status examination wikipedia , lookup
Abnormal psychology wikipedia , lookup
Causes of mental disorders wikipedia , lookup
History of psychiatry wikipedia , lookup
Controversy surrounding psychiatry wikipedia , lookup
Emergency psychiatry wikipedia , lookup
Biology of depression wikipedia , lookup
Child psychopathology wikipedia , lookup
Major depressive disorder wikipedia , lookup
History of mental disorders wikipedia , lookup
Behavioral theories of depression wikipedia , lookup
Evolutionary approaches to depression wikipedia , lookup
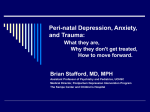
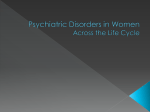
Picasso PERINATAL MOOD DISORDERS Spectrum of Perinatal Mood Disorders • Antepartum depression • Postpartum depression • Postpartum psychosis DEPRESSION DURING PREGNANCY • Between 10-20% of women will experience significant depression during pregnancy • This will be a first episode for one third Antenatal Risk Assessment • Do you have a history of depression, bipolar disorder or anxiety? • Have you ever been treated with antidepressant medication or other psychiatric medication? • Did you recently stop your antidepressant or other psychiatric medication? • Do you have a family history of depression or bipolar disorder? • Are you currently struggling with or being treated for depression or anxiety? • Are you feeling a lack of support during your pregnancy or worry that you will be without enough support after the baby is born? JAMA STUDY February 2006 • “Relapse of Major Depression During Pregnancy of Women Who Maintain or Discontinue Antidepressant Treatment” Lee Cohen et al. at MGH • Women from 3 specialty centers who were not depressed for at least 3 months prior to pregnancy and on antidepressant treatment. • 43% had a relapse in their major depression • 26% of those who continued their medication had a relapse (50% in first trimester) • 68% of those who discontinued their medication had a relapse (50 % In the 1st trimester, 90% by the end of the 2nd trimester) JAMA STUDY February 2006 CONCLUSIONS: • Pregnancy puts women with a history of depression at higher risk of recurrence and is not protective. • Women who are stable on antidepressants at the time of pregnancy need to be aware that there is a much higher risk of relapse associated with discontinuing their antidepressant medication • These issues should be part of the discussion with women when weighing the risk/benefit ratio of using antidepressants during pregnancy PREGNANCY IS NOT A TIME OF “PROTECTION” FROM MOOD OR ANXIETY DISORDERS SIGNIFICANCE Untreated depression during pregnancy is associated with serious risks for mother and her baby. OBSTETRICS AND GYNECOLOGY April 2008 "Advising a pregnant or breastfeeding woman to discontinue medication exchanges the fetal or neonatal risks of medication exposure for the risk of untreated mental illness." Untreated or inadequately treated maternal mental illness "may result in poor compliance with prenatal care, inadequate nutrition, exposure to additional medications or herbal medicines, increased alcohol and tobacco use, deficits in mother-infant bonding, and disruptions within the family environment.” OBSTETRICS AND GYNECOLOGY April 2008 Guidelines • Level A evidence (from good and consistent scientific evidence): – Lithium exposure in pregnancy may be associated with a small increase in congenital cardiac malformations, with a risk ratio of 1.2 to 7.7. – Valproate exposure in pregnancy is associated with an increased risk for fetal abnormalities and should be avoided if possible, especially during the first trimester – Carbamazepine exposure during pregnancy is associated with fetal carbamazepine syndrome and should be avoided if possible, especially during the first trimester. – Maternal benzodiazepine use shortly before delivery is associated with floppy infant syndrome. OBSTETRICS AND GYNECOLOGY April 2008 • Level B evidence (from limited or inconsistent scientific evidence): – Paroxetine use in pregnant women and women who are planning to become pregnant should be avoided, if possible, and fetal echocardiography should be considered when fetuses are exposed to paroxetine in early pregnancy. – Prenatal benzodiazepine exposure increased the risk for oral cleft (absolute risk increased by 0.01%). – Lamotrigine is a potential maintenance therapy option for pregnant women with bipolar disorder and has a growing reproductive safety profile relative to alternative mood stabilizers. – Untreated or inadequately treated maternal psychiatric illness may have various negative consequences. OBSTETRICS AND GYNECOLOGY April 2008 • Level C evidence (primarily from consensus and expert opinion): – Multidisciplinary care management involving the patient's obstetrician, mental health clinician, primary health care provider, and pediatrician is recommended whenever possible. – Use of a single medication at a higher dose is favored vs the use of multiple medications to treat psychiatric illness during pregnancy. – Close monitoring of lithium during pregnancy and postpartum is recommended. OBSTETRICS AND GYNECOLOGY April 2008 – Measuring serum drug levels in breast-fed neonates is not recommended. – Treatment with selective serotonin-reuptake inhibitors, selective norepinephrine reuptake inhibitors, or both during pregnancy should be individualized. – A fetal echocardiogram examination should be considered when the fetus is exposed to lithium during the first trimester of pregnancy. RISKS OF UNTREATED DEPRESSION DURING PREGNANCY • Lack of adequate prenatal care • Higher use of alcohol and drugs • Obstetrical and neonatal complications Higher rates of premature labor Higher rates of miscarriage Higher incidence of placental abruption Increased bleeding during gestation Increased risk of preeclampsia (five-fold in one large study) RISKS OF UNTREATED DEPRESSION DURING PREGNANCY More painful labor and higher use of analgesia Small for gestational age infants Lower APGAR scores Low birth weight Neonatal growth retardation Increased rate of stillborns (six times in one study) Increased admissions to neonatal ICU RISKS OF UNTREATED DEPRESSION DURING PREGNANCY • More likely to have colicky, irritable babies • Suicide • Subsequent Postpartum Depression or recurrent depression TREATMENT OF DEPRESSION DURING PREGNANCY • Mild to moderate depression may respond to supportive, cognitive or interpersonal therapy or other nonpharmacolologic treatments • More severe depression warrants medication use BIPOLAR DISORDER 75% of women with bipolar disorder experience recurrent illness if they discontinue treatment during pregnancy Postpartum Depression Peak lifetime prevalence for psychiatric disorders and hospital admissions for women occurs in the first 3 months after childbirth (Kendall et al, 1981, 1987) 70 Epidemiology of Postpartum Episodes Admissions/Month 60 50 40 30 20 Pregnancy 10 0 –2 Years – 1 Year Childbirth +1 Year +2 Years Kendell RE et al. Br J Psychiatry. 1987;150:6 THE MOST COMMON COMPLICATION OF CHILDBIRTH IS DEPRESSION BABY BLUES • Baby Blues usually develop 3-5 days after delivery • Hallmark is emotional reactivity • Occur in 70-80 % of all new mothers • Normal reactions to the hormonal changes and stress of having a baby POSTPARTUM DEPRESSION • Prevalence – 15% of postpartum women (1 out of 7 new mothers) • Higher-risk groups – Young, low socioeconomic status, poor social support – Family history of mood disorders – Past depression 25-40% risk of PPD – Prior PPD 30-50% risk recurrence Gaynes et al, 2005; www.ahrq.gov/clinic/epcsums/peridepsum.htm Wisner K et al. N Engl J Med. 2002;347:194-199 PRESENTATION OF PPD • Usually develops slowly over the first three months, most often beginning within the first 4 weeks, though some women have a more acute onset • More persistent and may affect ability to care for the baby • Signs and symptoms are those of Major Depression---depressed mood, irritability, loss of interest and appetite, fatigue insomnia. • Often complain of being physically and emotionally exhausted, but unable to sleep. PRESENTATION OF PPD • CLASSIC SYMPTOMS OF DEPRESSION WITH SOME TYPICAL FEATURES: • Often express concerns about her ability to care for her baby or anxiety about the baby’s well being • Anxiety symptoms are common including frank panic disorder, hypochondriasis, and most common, generalized anxiety disorder • Women are often unable to sleep even when given the opportunity PRESENTATION OF PPD • Frequently have intrusive, obssessional ruminations, usually focused on the baby, often violent in nature, but they are egodystonic and there is not a problem with reality testing i.e. non-psychotic. One study showed 50% of women with PPD had these. Such obsessional thoughts do not increase the risk of harm to the baby and are important to distinguish from psychosis. Duration of PPD • Untreated depression often persists for months to years after childbirth, with lingering effects on physical and psychological functioning following recovery from depressive episodes (England, Ballard & George, 1994). – 25%-50% women have episodes lasting 7 months or longer (O’Hara, 1987). – The most significant factor in the duration of PPD is delay in receiving treatment (England, Ballard & George, 1994). RISK FACTORS • Depression during pregnancy is the best predictor of post partum depression • Prenatal anxiety also a strong predictor of PPD • History of depression, especially PPD • Family history of depression • History or family history of late luteal phase disorder • Obstetrical complications at delivery • Complicated pregnancy • Neonatal loss or illness • Difficult infant temperament RISK FACTORS • • • • • • • • • Ambivalence about pregnancy Marital conflict Lack of social support Number of children Recent loss History of sexual abuse Low self esteem Recent stressful life events Breastfeeding difficulties Risks of Untreated PPD To mother: • Diminished capacity to care for self and baby • Substance abuse • Increased healthcare costs • Stressful impact on relationship between woman and her partner. • Suicidal thoughts more likely to be accompanied by homicidal thoughts • Kindling phenomenon---development of a chronic low grade depression with more susceptibility to repeated episodes of MDD Risks of Untreated PPD To child: • Poor attachment, bonding, and less nurturing maternal interaction • Poor weight gain • Sleep problems • Less likely to be breastfed • Less likely to receive preventative healthcare and child safety practices • Poor cognitive, language and and motor development • Behavioral problems—future conduct disorders, hyperactivity, and school behavior problems • Future depression and anxiety disorders • Risk of future medical illnesses as well —maternal depression is an “Adverse Childhood Experience” MATERNAL POST PARTUM MOOD IS ONE OF THE STRONGEST PREDICTORS OF NEUROCOGNITIVE DEVELOPMENT IN CHILDREN MEASURED UP TO AGE SIX Summary: Impact of PPD Diminished maternal ability to function in many roles particularly the core parenting role with long lasting adverse effects on child’s health, cognitive and emotional development and ongoing risk to mother’s emotional, physical, and social wellbeing. Treatment for mother is prevention or early intervention for child POST PARTUM ANXIETY DISORDERS Postpartum Onset Anxiety/Panic Disorder 10% of new mothers Postpartum Obsessive/Compulsive Disorder (PPOCD) 3-5% of new mothers Postpartum Stress Disorder (PPTSD) 1-3% of new mothers may develop. Mothers who have had a traumatic childbirth experience, premature birth and loss of child are at most risk for onset of PPTSD. Mothers who have experienced a history of childhood sexual or physical abuse are also at higher risk. POST PARTUM PSYCHOSIS • Typical onset is within 2 weeks after delivery, first symptoms often within 48-72 hours • Earliest signs are restlessness, irritability and insomnia • Often very labile in presentation • Often looks “organic” with a lot of confusion and disorientation • Most often consistent with mania or a mixed state POST PARTUM PSYCHOSIS • Includes agitation, paranoia, delusions, disorganized thinking and impulsivity • Thoughts of harming the baby are frequently driven by delusions—Child must be saved from harm, child is malevolent, dangerous, has special powers, is Satan or God • Rates of infanticide associated with untreated postpartum psychosis have been estimated to be as high as 4%. Risk Spectrum for Postpartum Psychosis • Highest-prior history of psychosis, particularly postpartum • Moderate --Bipolar disorder • At risk--Previous postpartum depression TREATMENT OF POSTPARTUM PSYCHOSIS Postpartum psychosis warrants emergency level care and usually requires inpatient hospitalization • Treat as affective psychosis—i.e. as Bipolar disorder • Medication treatment is necessary beginning with an antipsychotic/mood stabilizer such as Zyprexa Suicide in the Postpartum Period • Any indication of self-harm or suicidal ideation should be taken seriously • Further assessment and intervention are urgently required when a woman scores positive on item #10 on EPDS or question # 9 0n the PHQ-9 • Severe postpartum psychiatric disorder is associated with a high rate of death from natural and unnatural causes, particularly suicide • Suicide risk in the first postnatal year is estimated to be increased by 70-fold (Appleby et al 1998) Age at Death for Infants Dying From Intentional or Suspicious Causes, US, 1990-97 50% 44% 45% 40% 42% 35% 30% 25% 20% 15% 10% 5% 8% 2% 4% 0% <1 day 2-6 days 7-28 days 1-3 months 4-11 months Source: Centers for Disease Control and Prevention. WONDER, compressed mortality file, 2000. DESPITE MULTIPLE CONTACTS WITH MEDICAL PROFESSIONALS FOLLOWING THE BIRTH OF A CHILD, POSTPARTUM DEPRESSION MOST OFTEN GOES UNDIAGNOSED. All women should be considered at risk for PPD and should be screened Need for Patient Education • Lack of knowledge about PPD, treatment options, and community resources is common in postpartum women and their families, and frequently leads to delay in seeking treatment • Delay in treatment for PPD results in a longer illness • Information about PPD should be provided to women in the prenatal period, soon after delivery, and further encounters with healthcare providers in the first postpartum year. Screening for Postpartum Depression • Postpartum depression is often not recognized • Despite the availability of many screening tools, PPD remains under • Absence of screening often means untreated depression and poor outcomes for the mother, her newborn, and family • Postpartum depression can be screened for with simple and validated screening tools Validated Screening Tools EPDS- Edinburgh postnatal Depression Screen PHQ-9 Patient Health Questionnaire PHQ-2 PPDS Postpartum Depression Scale Beck Depression Inventory-IICenter for Epidemiological Studies-Depression Scale (CES-D) EPDS Please UNDERLINE the answer that comes closest to how you have felt in the last seven days, not just how you are feeling today. 1. I have been able to laugh and see the funny side of things. As much as I always could Not so much now Definitely not so much now Not at all 2. I have looked forward with enjoyment to things. 3. I have blamed myself unnecessarily when things went wrong. 4. I have been anxious or worried for no good reason. 5. I have felt scared or panicky for not very good reason. EPDS 6. 7. 8. 9. 10. Things have been overwhelming me. I have been so unhappy I have had difficulty sleeping. I have felt sad or miserable. I have been so unhappy that I have been crying. The thought of harming myself has occurred to me. Scoring: 0-3 points per question Score > 10 warrants further assessment EPDS SCREENING H/O BIPOLAR DISORDER EPDS 5-9 EPDS 10 OR MORE ANSWERS YES TO QUESTION # 10 OR RISK OF SUICIDE OR HARM TO INFANT EPDS 10 OR MORE Patient at increased risk Discuss signs and symptoms Follow more closely MENTAL HEALTH REFERRAL ER OR CRISIS TEAM ASSESSMENT INTERVIEW EVALUATION PPD CONFIRMED MEDICATION INDICATED AND RISKS BENEFITS DISCUSSED AND DOCUMENTED PPD NOT CONFIRMED or medication not indicated Clinical jugdement to determine the following: Rescreen at next visit Follow clinically Mental health provider referral Support Group PATIENT ACCEPTS PATIENT DECLINES USE GUIDELINES AND PATIENT HISTORY TO CHOOSE MEDICATION http://www.hfs.illinois.gov/assets/0820 07_mch.pdf Refer to support group or counseling Involve partner/family Mental health referral Support Group Referral Consider the following recommendations: bright light therapy, omega fatty acid therapy, exercise EVALUATE 4-6 WEEKS OUTCOME NEGATIVE MENTAL HEALTH REFERRAL OUTCOME POSITIVE DOCUMENT EVIDENCE IN MEDICAL RECORD CONTINUE MEDICATION 9-12 MOS AFTER SYMPTOMS REMIT EVALUATE EVERY 3 MONTHS PHQ-9 Over the last 2 weeks, how often have you been bothered by any of the following problems? Little interest or pleasure in doing things 2. Feeling down, depressed, or hopeless 3. Trouble falling or staying asleep, or sleeping too much 4. Feeling tired or having little energy 5. Poor appetite or overeating 6. Feeling bad about yourself—or that you are a failure or have let yourself or your family down 7. Trouble concentrating on things, such as reading the newspaper or watching television 8. Moving or speaking so slowly that other people could have noticed. Or the opposite—being so fidgety or restless that you have been moving around a lot more than usual 9. Thoughts that you would be better off dead, or of hurting yourself in some way PHQ-9 Patient uses the following rating for each question: Not at all Several days More than half Nearly every day Score Depression Severity 1-4 Minimal depression 5-9 Mild depression 10-14 Moderate depression 15-19 Moderately severe depression 20-27 Severe depression 10. If you checked off any problems, how difficult have these problems made it for you to do your work, take care of things at home, or get along with other people? PHQ-9 is adapted from PRIME MD TODAY, developed by Drs Robert L. Spitzer, Janet B.W. Williams, Kurt Kroenke, and colleagues, with an educational grant from Pfizer Inc. For research information, contact Dr Spitzer at [email protected]. Use of the PHQ-9 may only be made in accordance with the Terms of Use available at http://www.pfizer.com. Copyright ©1999 Pfizer Inc. All rights reserved. PRIME MD TODAY is a trademark of Pfizer Inc PHQ-9 SCREENING H/O BIPOLAR DISORDER PHQ-9 <5 PHQ-9 5-10 PHQ-9 >10 OR MENTAL HEALTH REFERRAL NO INTERVENTION RISK OF SUICIDE OR HARM TO INFANT ER OR CRISIS TEAM EVALUATION ASSESSMENT INTERVIEW PPD NOT CONFIRMED or medication not indicated PPD CONFIRMED MEDICATION INDICATED AND RISKS BENEFITS DISCUSSED Clinical jug dement to determine the following: Rescreen at next visit Follow clinically Mental health provider referral Support Group PATIENT ACCEPTS PATIENT DECLINES USE GUIDELINES AND PATIENT HISTORY TO CHOOSE MEDICATION http://www.hfs.illinois.gov/assets/082 007_mch.pdf Refer to support group and counseling Involve partner/family Mental health referral Support Group Referral Involve partner/family Consider the following recommendations: bright light therapy, omega fatty acid therapy, exercise EVALUATE 4-6 WEEKS OUTCOME NEGATIVE MENTAL HEALTH REFERRAL OUTCOME POSITIVE DOCUMENT EVIDENCE IN MEDICAL RECORD CONTINUE MEDICATION 9-12 MOS AFTER SYMPTOMS REMIT EVALUATE EVERY 3 MONTHS PHQ-2 Over the past two weeks, how often have you been bothered by any of the following problems? 1. Little interest or pleasure in doing things. 2. Feeling down, depressed, or hopeless. • 0 = Not at all • 1 = Several days • 2 = More than half the days • 3 = Nearly every day Perinatal Depression Screening When to screen: Antenatal early risk assessment and screening during pregnancy. ACOG recommends the PHQ-2 once per trimester If at high risk (prior history, neonatal loss, obstetrical complications, etc): Upon discharge from hospital. Need to assess support plan post discharge At early (2 week) follow up appointment Perinatal Depression Screening Postpartum OB/midwife visit 6-7 weeks Well child pediatrician visits for the first year Other possible times: Lactation consultant visit Visiting home nurse Perinatal Depression Screening • In a national sample, 57% of pediatricians felt responsible for recognizing maternal depression (Olson AL et al. Pediatrics. 2002;110:1169-1176) • Well-child visit is an ideal time to look for signs of PPD in the mother (See pediatric provider frequently first year) • “Pediatricians should ascertain the physical and mental health of the parents in their practice and periodically review the importance of parents’ attention to their own mental health needs.” – AAP: Report of the Task Force on the Family Perinatal Depression Screening • Recognition is key: risk factors, warning signs, symptoms, early identification • Be alert for plans or intent to harm self (suicide), infant, others • Indications for emergency intervention: psychosis, risk of suicide or harm to the infant • Refer to mental health professional if concomitant substance abuse, bipolar symptoms or history of bipolar disorder, history of psychiatric hospitalization Training for Office Staff • Familiarize office staff with screening tools • Train staff to ask the appropriate questions when woman call • Have accessible and up to date contact for local emergency mental health care • Have up to date information for other mental health resources: outpatient mental health providers, support groups, support associations such as PSI Perinatal Depression Screening Selection of treatment: first requires good evaluation, review of prior history, patient education and assessment for sociality/dangerousness Individual psychotherapy--CBT /IPT Medication with discussion of risks and benefits Bright light therapy Support group Support programs Hospitalization ECT Obstacles to Screening • Lack of familiarity (health care provider and patient • Lack of training • Lack of protocols • Patient’s reluctance to disclose feelings • Lack of easy assess to mental health resources • Lack of time • Lack of reimbursement What Do Women Need To Talk About? • Negative childbirth experiences—especially with trauma • Concerns about their infants—their temperaments, health issues • Interactions with their babies and caring for them • How this time differs from their expectations • Feelings of isolation What Do Women Need To Talk About? • Loss—of prior employment role, closeness with spouse or older child • Feelings of frustration , inadequacy in mothering • Breastfeeding difficulties • Loss of care and attention received during pregnancy • Ambivalence about returning to work and sense of loss when that is a necessity Maine LD 792 An Act to Promote Postpartum Mental Health Education Modeled after other state initiatives— i.e. New Jersey http://www.maine.gov/dhhs/data_reports.shtml#healthrelated http://www.maine.gov/dhhs/publications.shtml#legislative MAPP PPD PROJECT A statewide project funded by a grant from the American Psychiatric Association for the purpose of collaborating with other medical specialties and other members of the mental health community to promote understanding of postpartum depression as a psychiatric illness with serious consequences to mothers and infants, decrease stigma, and increase recognition and treatment of PPD PPD Resources www.postpartum.net Postpartum Support International Crisis hotline for postpartum depression and psychosis: 1-800-PPD-MOMS www.mededppd.org NIMH supported website Excellent resource, regularly updated 9 educational modules aimed at different provider categories offering CME’s www.womensmentalhealth.org MGH Center for Women’s mental Health 1-800-PPD-MOMS Crisis hotline for postpartum depression and psychosis: 1-800-573-6121 Illinois Perinatal Mental health Consult Service—telephone consultation by perinatal mental health experts for any health care provider with prescriptive authority