Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
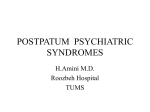
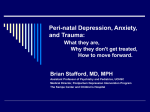
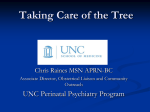
“The burden of mental disorders, such as depression and anxiety, fall disproportionately on women of childbearing and childrearing age.” Psychiatric Clinics of North America, 2007 Rates of severe mental illness similar between men and women, but differences in diagnoses, age of onset, course. Rates of Major Depression and Dysthymia are about twice as high for women as for men Prevalence rates for most Anxiety Disorders (panic disorder, agoraphobia, specific phobia, GAD, PTSD) are 2-3x higher in women (exceptions are OCD and social phobia: rates are =) Bipolar Disorder – Type I rates = in men and women, Type II women > men › More mixed episodes, rapid cycling › Later age of onset, more depressive episodes Schizophrenia – Lifetime prevalence = in men and women. › Women have later age of onset (25-35) with bimodal distribution › Higher premorbid functioning and social functioning › More “benign” course Eating Disorders – Anorexia Nervosa 95% female; Bulimia 80% female Substance Abuse : Men 2-4 x more likely to have dx of substance abuse or dependence › Women with affective illness more vulnerable Personality Disorders: › Women > Men in Borderline, Histrionic (?) › Men > Women in Antisocial, Narcissistic, Obsessive-Compulsive 25 20 15 Female Male 10 5 0 MDE DD SAD PMDD BPD Biologic Vulnerability Reproductive Events Psychosocial Factors Gender based violence (rape, sexual abuse, domestic violence) Socioeconomic status Caregiving responsibilities, multiple roles Menstrual Cycle Infertility Pregnancy Postpartum Period Menopausal Transition/Perimenopause Hormonal Therapies Higher incidence of MDD in women starting at puberty, less marked post-menopause Suicidal behavior may be more common in low estrogen states 5% rate of PMDD Rates of postpartum admissions and psychosis elevated immediately after childbirth Perimenopausal mood d/o’s vs. postmenopause Kessler et al, 1993 (National Comorbidity Survey) Fig. 1. Phases of the menstrual cycle positively correlated with suicide attempts and changes in oestrogen concentration during the cycle. * Denotes studies where results were statistically significant. Saunders et al, 2006 Estrogen Progesterone FSH LH Testosterone HCG Prolactin TRYP Estrogen 5HT 5HT Re-uptake Site E2 PROG MAO: Monoamine Oxidase COMT: Catechol-O-Methyl Transferase 5HT: Serotonin MAO / COMT E2 MAO & COMT - 5HT PROG MAO & COMT - SHT Psychological Symptoms Depression Anger, Irritability Affective lability Anxiety Sensitivity to rejection Poor concentration Sense of feeling overwhelmed Social withdrawal Physical Symptoms Lethargy or fatigue Sleep disturbance (usually hypersomnia) Appetite disturbance (usually increased) Abdominal bloating Breast tenderness Muscle aches, joint pain Swelling of extremities Affects 3-8% of menstruating women Symptoms begin during Luteal Phase, resolve completely with onset of menses ≥5 symptoms in most cycles Marked decrease in social or occupational functioning Distinguish from underlying mood disorder (no symptoms Follicular Phase) Abnormal serotonin neurotransmission? Lifestyle interventions, exercise Calcium, Vit B6, Magnesium, Vit E Herbal remedies (chasteberry) Psychotherapy SSRI’s (fluoxetine, paroxetine, sertraline) › Immediate effect › Intermittent vs. continuous dosing Hormonal therapies Increased risk for first episode depression during menopausal transition Lower risk for first episode depression in post-menopausal women Women with a history of depression remain at risk for future episodes Estrogen replacement effective for mild symptoms, but not Major Depression Is pregnancy a time of emotional wellbeing for women? Pregnancy is NOT protective against psychiatric illness Rates of Major Depression during pregnancy 10-15% Anxiety disorders may be higher. High rate of relapse when antidepressant medications are stopped during pregnancy (~50-70%) Pregnant Bipolar women have same risk for relapse off meds as non-pregnant Bipolar women. Post partum risk 4x higher. Past history of depression Poor overall health Greater alcohol use Smoking Being unmarried Unemployment Lower education level Level of suffering – for mom and partner Decreased ability to care for herself and the pregnancy – suicide risk in severe cases Increased risk for pre-term delivery, preeclampsia, and low birth weight Higher rates of smoking, alcohol and substance use Risk of post-partum depression, negative effects on child and family Non-Pharmacologic Treatments: Psychotherapy Light Therapy Omega-3 Fatty Acids Psychosocial supports Psychotropic Medications in Pregnancy – are they safe? No Psychotropics are FDA-approved for use during pregnancy All medications cross the placenta Principals of management: maximize non-medication options, minimize exposure to meds and to depression Teratogenesis › No increase in overall rate of fetal malformations › Some evidence linking inc risk of rare defects (i.e. paroxetine and cardiac malformations) Pregnancy Outcomes › Mixed evidence on birth weight, early pregnancy loss, preterm labor (depression effects?) Neonatal Toxicity › Neonatal Abstinence Syndrome › Persistent Pulmonary Hypertension of the Newborn Long-term effects › No evidence to date of long-term developmental effects in children exposed in utero “Baby Blues” Postpartum Depression Postpartum Psychosis Y axis: Rates of psychiatric hospitalization X axis: Years pre- and post- childbirth “When I delivered the placenta, I felt like I fell off a cliff.” Occurs in 50-85% of women Characterized by mood lability, tearfulness, anxiety and irritability Symptoms peak at day 4-5 May last a few hours to several days Symptoms do not interfere with functioning Reassurance rather than treatment If symptoms persist > 2 weeks, patient should be evaluated for a more serious mood disorder Occurs in 1-2 per 1000 women Onset 24hrs – 3 weeks postpartum Rapid mood swings, insomnia, obsessive thoughts Delusions, hallucinations, impaired reality testing. Delusions involving infant are common Shifting mental status , disorientation, confusion, disorganized behavior High risk of suicide and/or infanticide Psychiatric emergency – needs evaluation immediately Differential: medical causes of delirium, PPD, SCZ >70% appears to be a presentation of bipolar disorder. Bipolar women at very high risk of PPP Estimates of prevalence between 10-15% Risk factors: › Prior episodes depression or anxiety, › › › › › including during pregnancy Marital discord Unwanted or unplanned pregnancy Infant medical problems Lack of social support Low socioeconomic status Differential: anemia, diabetes, thyroid Symptoms: • Depressed mood • Tearfulness • Loss of interest in usual activities • Feelings of guilt • feelings of worthlessness or incompetence • Fatigue • Sleep disturbance • Change in appetite • Poor concentration • Suicidal thoughts Milder cases overlap with normal feelings in the postpartum period – i.e. fatigue, altered sleep, appetite, energy Hopelessness, worthlessness, suicidal ideation are not normal in the postpartum period Comorbid anxiety with obsessional thoughts about the baby is common › Important to distinguish from psychosis Edinburgh Postnatal Depression Scale › 10-item self-rating scale measuring mood, anxiety and SI Psychotherapy: IPT, CBT, Supportive, Psychodynamic, Couples, Group Improved social supports Help with infant care Light therapy Medications: SSRI’s, Tricyclics, Benzodiazepines for comorbid anxiety All psychotropic medications are secreted into breast milk Concentrations in breast milk vary widely Peak concentrations are attained at 6-8 hours Infant toxicity depends on exposure and hepatic metabolism Relationship between infant serum concentrations and infant physiology, behavior and development is unknown Carefully monitor breast fed infants Mood and Anxiety disorders disproportionately affect women of reproductive age Times of hormonal change may be periods of particular vulnerability Many women are reluctant to seek treatment, diagnoses often missed Treatment of psychiatric illness is complicated by potential pregnancy, pregnancy, postpartum issues Risks and benefits of both treatment and nontreatment must be carefully considered