Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Major histocompatibility complex wikipedia , lookup
Polyclonal B cell response wikipedia , lookup
Cancer immunotherapy wikipedia , lookup
Management of multiple sclerosis wikipedia , lookup
Adoptive cell transfer wikipedia , lookup
Molecular mimicry wikipedia , lookup
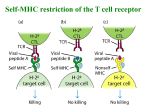
TRANSLATIONAL RESEARCH New Therapies for MS Dennis Bourdette, M.D. and Arthur A. Vandenbark, Ph.D. •TCR peptide therapy •Recombinant TCR ligand (RTL) therapy Therapeutic Vaccination of MS Patient Stimulus: TCR BV5S2 Peptide Myelin Basic Protein EDSS 7 6 10 5 4 3 1 2 1 0.1 0 0 13 26 39 Weeks on Therapy 52 65 EDSS LDA Frequency x 10-6 100 TCR Peptide Vaccination Pilot Trials: Composite Phase I and II Studies Clinical Responses Responders Improved Stable Worse Strong 3 1 0 Moderate 0 6 2 Non-Responders 1 6 13 Strong Response: Moderate Response: > 8 cells/million 2 - 8 cells/million P < 0.001 0020963B Fraction of Active MRI Scans: TCR Responders vs. Non-Responders 70% 60% 50% TCR Responder 40% 30% TCR NonResponders 20% 10% 0% Baseline 16 wks 20 wks 24 wks Conclusions: TCR Peptide Therapy Safe and well tolerated May induce missing regulatory T cell population in MS patients Peptide cocktails more effective Timeline for development of TCR peptide therapy • • • • • • • • 1988: Aha!! 1989: Treatment of EAE. 1991-94: Phase I Clinical Trial. 1996: Phase I/II Pilot Trial Suggests Efficacy. 2001-02: Treatment with Peptide Cocktail. 2003: Open Label Study to Improve Assays. 2007: Phase II/III Proof of Principle Trial 2010?: FDA Approval. Translational Aspects • Patent applied for through VAMC • Rights to invention were assigned to The Immune Response Corporation (IRC) • Two initial trials were Investigator initiated • Remaining trials were run through IRC • Basic science advances continued throughout clinical testing through NIH and NMSS funding RTL (Recombinant TCR Ligand) Therapy for MS Arthur A. Vandenbark, Ph.D., Gregory G. Burrows, Ph.D., Halina Offner, Dr. Med., Dennis Bourdette, M.D. Funded by NIH, NMSS, VA, Virogenomics T cell activation Responsive ResponsiveTTCell Cell T Cell Receptor T Cell Activation Myelin Basic Protein (MBP) peptide CD4 1 1 2 2 Inflammatory Inflammatory Factors factors MHC II β2 domain of MHC II contains key binding site for CD4 protein Recombinant T Cell Receptor Ligand 1. Safe and effective in animal models of MS. 2. Specific target = fewer side effects 3. Platform to treat other inflammatory diseases (e.g. arthritis) 4. Attractive manufacturing and commercial properties p-a linker linker P-β Interchangeable Peptide 1 b-a linker linker α-β 1 Effect of RTL on T Cell activation PRO-inflammatory cytokines are NOT released, causing a local reduction of T cell response in inflamed area T Cell Receptor Antigenic Peptide P-α linker RTL 1 Portion of MHC II molecule; without lower 2 and 2 chains ANTI-Inflammatory cytokines (IL-10) released: Suppress neighboring inflammatory cells Protect lesions from further attack (bystander suppression) 1 β- linker 2 X 2 CD4 no longer binds, since it lacks the 2 domain of the MHC II. Thus, activation is altered Treatment of Relapsing EAE with RTLs Control 6 RTL401 3d i.v. RTL401 8d.i.v. 4 RTL401 s.c. 2 Days Post Immunization 46 44 42 40 38 36 34 32 30 28 26 24 22 20 18 16 14 12 0 10 Mean Disease Score RTL401 4d.i.v. Mean EAE Score 6 5 4 VG312(100ug) VG312(33ug) VG311 or 303 vehicle (Tris, pH 8.5) 3 2 1 0 0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 Days after initiation of treatment Treatment Incidence Onset VG312(100ug) VG312(33ug) VG311 or 303(100ug) Vehicle 11/11 9/9 8/8 17/17 9.6 ± 1.4 9.6 ± 2.5 9.9 ± 0.6 10.2 ± 1.6 # Mean Score at start of treatment Mean Score at end of treatment * 2.3 ± 0.5 2.6 ± 0.5 2.9 ± 0.5 1.8 ± 0.3 a = Significant difference between vehicle and experimental group (p 0.4 ± 0.1a 0.2 ± 0.4a 3.4 ± 0.5 3.8 ± 0.4 CDI 10.8 ± 2a 15.1 ± 3.7a 55.6 ± 17.4 55 ± 4 < .0001; Mann-Whitney Test) * = Significant difference between each group (H = 29.96; p < .001; Kruskal-Wallis Test) # = Significant difference between each group (H = 31.27; p < .001; Kruskal-Wallis Test) Conclusions: RTL Therapy Potent therapy in animal models for MS Induced long-lasting, highly specific T cell tolerance to myelin peptides Changed the cytokine profile of encephalitogenic T cells Induced neuroprotection TIMELINE FOR RTL THERAPY • • • • 1996 – Aha!! 1998 – Therapeutic activity in rats 1999 – First patent filed 2002 – Therapeutic activity in DR2 transgenic mice using monomer • 2006 – IND approved by FDA • 2007 – Phase I Safety Trial initiated Translational Aspects • Patents applied for through OHSU • Rights to invention were licensed to Artielle ImmunoTherapeutics, Inc. • Company was responsible for producing GMP grade RTL1000, toxicity studies, FDA interactions • OHSU lab tested clinical variables for therapy to support IND application • Basic science advances continued throughout clinical testing through NIH, NMSS & VA funding