Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Molecular mimicry wikipedia , lookup
Inflammation wikipedia , lookup
Immune system wikipedia , lookup
Lymphopoiesis wikipedia , lookup
Polyclonal B cell response wikipedia , lookup
Adaptive immune system wikipedia , lookup
Cancer immunotherapy wikipedia , lookup
Psychoneuroimmunology wikipedia , lookup
Adoptive cell transfer wikipedia , lookup
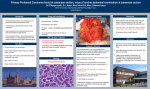
PERITOINE ET INFLAMMATION Pierre Moine Department of Anesthesiology University of Colorado Health Sciences Center Peritonitis general phases [Bartlett JG. Arch Surg 1978] 1. Bacteriemic phase Phase of rapid removal of contaminants from the peritoneal cavity into the systemic circulation. This phase predominently involves Gram-negative aerobes 2. Aerobs and anaerobs synesgistic interaction phase 3. Infection localization The normal peritoneal cavity • About 300 cells/mm3 • Mainly macrophages (45%), lymphocytes (T cells 45% - NK cells 6% - B cells 2% (peritoneal CD5+ B1 cells)), dendritic cells (2%), mast cells and desquamated PMCs • Peritoneal-associated lymphoid tissue (omental milky spots, lymphocytes within the peritoneal fluid, and the draining lymph nodes) Peritoneal mesothelial cells PMCs have the same mesodermal origin as the endothelial cells; both types of cell can express specific surface markers that enable them: 1. To promote the margination and migration of neutrophils, 2. To interact with extracellular matrix proteins, 3. To present antigens to immune cells, 4. To produce inflammatory mediators such as proinflammatory cytokines, NO, growth factors, tissue plasminogen activator and plasminogen activator inhibitor. ‘‘Milky spot’’: They consist of macrophages, B and T lymphocytes and mast cells, immersed in a network of connective tissue, vascularized by fenestrated capillaries and lymphatic vessels. Near milky spots, the mesothelium is practically devoid of basement membrane so that macrophages and lymphocytes do not encounter any obstacles in the peritoneal lumen. Milky spots may also be associated with stomata. Diagram of the proposed sequence in the morphogenesis of Lymphatic stomata [Nakatani T et al, Anat Rec 1997] BL E G L M P S Basal lamina Lymphatic endothelial cell Gap Lymphatic cavity Peritoneal mesothelial cell Peritoneal cavity Lymphatic stoma The PMCs lining the muscular portion of the diaphragm are interrupted by a large number of intermesothelial gaps (Stomata). Defects in the basement membrane allow the stomata to communicate directly with the underlying lymphatic lacunae. The peritoneal infection • Leukocytes influx into the peritoneal cavity is a characteristic and diagnostic feature of peritoneal infection. • Leukocyte influx is characterized by increases in both polymorphonuclear leucocytes (PMN) and mononuclear cells (mononuclear phagocytes and lymphocytes). • Initially PMNs predominate and they are subsequently replaced by mononuclear cells as the main cell population as infection resolves. Early phase of the peritoneal inflammatory response The peritoneal cavity (1) • Under normal circumstances, 1/3 of the fluid draining from the peritoneal cavity passes through the diaphragmatic lymphatics, and the remainder exits through the parietal peritoneum • The action of the diaphragm generates a cephalad flow of peritoneal fluid • Relaxation of the diaphragm generates a negative pressure that sucks fluid and particles into the stomata. • Contraction of the diaphragm closes the stomata and forces lymph to the mediastinum. The peritoneal cavity (2) • After exposure to P aeruginosa, there are larger stomata (4-10 mm to 23 mm) and lymphatic lacunae. New stomata are also formed. This adaptation is aimed at enhancing peritoneal clearance. • In experimental animals, 1/2 of the bacteria placed within the peritoneal cavity are removed via the diaphragmatic lymphatics, and they appear in the thoracic duct within 6 minutes. • Depression of spontaneous respiration under general anesthesia decreases the rate of bacterial clearance from the peritoneal cavity The powerful absorptive capacity of the peritoneum Mechanical clearance of irritants from the peritoneal cavity Diaphragm Omentum Mesenteric peritoneum Pelvic peritoneum Clinical issues It explains • the rapid onset of systemic signs of peritonitis • The primacy of early antimicrobial therapy • The need to avoid organizational delays before surgery Natural antibodies and complement link innate and acquired immunity [Ochsenbein et al, Immunology Today 2000] Mechanisms of how NAs protect against infections. Protection can occur directly or indirectly (via the complement system), and also by enhancing the specific Ab response, leading to a more efficient control of the infection. These links to adaptive immunity are highlighted in blue. Abbreviations: TI, T-cell independent; TD, T-cell dependent. Role of the classical pathway of complement activation in experimentally induced polymicrobial peritonitis [Celik I et al, Infect Immun 2001] - Natural IgM antibodies (peritoneal CD5+ B1 cells) - Early adaptative immune response C1qa-/-: functional lectin and alternative pathways H2-Bf/C2 -/-: Deficient in all 3 complement activation pathways (classical, lectin, and alternative) 2. Bacterial activation of PMC 3. Peritoneal macrophages – PMC interaction 1. Direct recruitment Peritoneal cavity IL-1 TNF-a MCP-1 RANTES ICAM-1 VCAM-1/2 PMC Peritoneal mesothelial cell and basement membrane PMN Peritoneal macrophages IL-8 CD11/18 Submesothelium IL-8 Mechanisms of leukocyte recruitment to the peritoneal cavity [Topley N, Kydney Int 1996] Chemokines in the septic inflammatory response - C-X-C Chemokines [Neutrophil chemotactic and stimulatory activity] IL-8 (murine analog MIP-2) ENA-78 NAP-2 IP-10 GRO-a (murine KC) MIP-1a MCP-1 - C-C Chemokines [Monocyte/macrophage chemotactic and stimulatory activity] MCP-1 (murine analog JE) RANTES C10 MIP-1a MIP-1b Peritoneal interleukin-8 in acute appendicitis [Zeillemaker Am et al, J Surg Res 1996] Chemokines produced by mesothelial cells huGRO-a, IP-10, MCP-1 and RANTES [Visser CE et al., Clin Exp Immunol 1998] ND TNF-a huGRO-a IP-10 MCP-1 RANTES (U/ml) (ng/ml) (ng/ml) (ng/ml) (ng/ml) 0 1.3 ± 1.4 ND 4.9 ± 1.1 ND 0.6 2.3 ± 0.6 ND 1.0 ± 1.1 ND 6.25 3.7 ± 1.1 ND 1.1 ± 0.9 ND 62.5 4.3 ± 0.8 ND 2.9 ± .4 0.1 ± 0.3 625 15.7 ± 2.0 ND 9.1 ± 2.5 0.2 ± 0.3 6250 32.4 ± 4.1 ND 14.9 ± 3.2 0.5 ± 0.7 TNF-a + IFN- 6.8 ± 1.5 70.6 ± 4.5 64.3 ± 6.6 3.8 ± 1.8 TNF-a + IL-1b 2.9 ± 1.5 0.5 ± 0.3 41.8 ± 2.2 0.4 ± 0.3 Chemokines produced by mesothelial cells huGRO-a, IP-10, MCP-1 and RANTES [Visser CE et al., Clin Exp Immunol 1998] mRNA expression of MCP-1 Densotometric 15 10 5 0 2 4 8 12 24 IL-1b 2 4 8 12 24 TNF-a 2 4 8 12 24 IFN- * † Control * IL-1b + IFN- † TNF-a + IFN- Leukocyte migration across human peritoneal mesothelial cells is dependent on directed chemokine secretion and ICAM-1 [Li FK et al, Kydney Int 1998] Chemokine concentration pg/105HPMC % of total chemokine secretion 20000 100 10000 50 0 0 IL-8 Control apical IL-1bapical MCP-1 Control basolateral IL-1bbasolateral IL-8 RANTES Control apical Control basolateral Production of IL-1b and TNF-a by peritoneal macrophages depends on the bacterial species and the inoculum [Visser CE et al, Adv Perit Dial 1997] Peritoneal interleukin-8 in acute appendicitis [Zeillemaker Am et al, J Surg Res 1996] IL-8 secretion by human mesothelial cell monolayers after 24 hr incubation with bacteria (108/ml), cultured from peritoneal fluid samples of patients with perforated appendices. Leukocytes (106/cavity) Time after CLP (Days) J Immun 1999; 163:6148 MIP-2 : human analog IL-8 Infect Immun 1997; 65:3847 Infect Immun 1997; 65:3847 MIP-2 : human analog IL-8 Infect Immun 1997; 65:3847 MIP-2 : human analog IL-8 MIP-2 : human analog IL-8 Infect Immun 1997; 65:3847 MCP-1 (ng/ml) MCP-1 (ng/cavity) Peritoneal fluids Serum Time after CLP (Days) J Immun 1999; 163:6148 % Survival Control Anti-MCP-1 antiserum injected 2 h before CLP Time after CLP (Days) J Immun 1999; 163:6148 Anti-MCP-1 Neutrophils Total leukocytes CFU/10 ml peritoneal fluids Macrophages Control Time after CLP (Days) J Immun 1999; 163:6148 Control LTB4 receptor antagonist MCP-1 (ng/cavity) Leukocytes (106/cavity) Effects of a specific LTB4 receptor antagonist on the leukocyte infiltration and on the production of MCP-1 after CLP Total leukocytes Macrophages Neutrophils Control LTB4 antagonist J Immun 1999; 163:6148 % Survival Effects of a specific LTB4 receptor antagonist on the survival of mice after LCP Control LTB4 receptor antagonist Time after CLP (h) J Immun 1999; 163:6148 Role of the resident peritoneal macrophages and mast cells in chemokine production and neutrophil migration in acute inflammation: Evidence for an inhibitory loop involving endogenous IL-10 [ Ajuebor MN et al., J Immunol 1999] Peritoneal neutrophils x 106 mMCP-1 / mouse ng per cavity 10 6 5 3 0 0 Control Resident Mast cell macrophages depleted depleted Control Resident Mast cell macrophages depleted depleted 24 hr post i.p. injection of 1 mg/kg LPS Differing responses of mast cells to allergen and to bacteria Piecemeal Selective release of Histamine Leukotrienes TNF, IL-6 Th2-associated cytokines (IL-10, IL-5, IL-13) Neutrophil recruitment Bacterial clearance Caveolar chamber with viable bacteria IgG opsonized bacteria Phagolysosome with degraded bacteria Malaviya R & Abraham SN, Immunological reviews 2001 Histamine Serotonine LTB4 LTC4 IL-10 IL-5 IL-13 TNF-a LTB-4 Mast cell MN TNF-a MCP-1 IL-1 RANTES IL-17 LTB-4 VCAM-1 HLA-DR CystLT PGF1a PGE2 PAF IL-8 LTB-4 LTB-4 IL-8 Bacteria IFN- IL-10 MCP-1 PMC GRO-a IP-10 CD40 IL-15 PMN NO CD154 IL-6 sIL-6R MCP-1 RANTES CD4 T cell ORS Late phase of the peritoneal inflammatory response Chemokine C10 promotes disease resolution and survival in an experimental model of bacterial sepsis [Steinhauser ML et al., Infect Immun 2000] C10 is involved in the late stages of the inflammatory process Kaplanski G et al., Trends in Immunology 2003 Modulation of the PMN recruitment IFN- deficiency IL-6 deficiency 1. Delay in the initial rate of PMN accumulation 2. Delay in neutrophil clearance 3. Reduction in overall PMN numbers 4. Increased C-X-C KC/MIP-2 expressions 5. Defective PMN apoptosis 1. Greater PMN infiltration (but the initial rate of PMN infiltration is unaffected) 2. Increased KC/MIP-2 expressions 3. Delay in neutrophil clearance 4. Defective PMN apoptosis Innate immunity CXC chemokines IFN- IL-1b - TNF-a dependant MIP-2 (IL-8) - KC CD40-CD154 dependant CD40-CD154 IL-6-sIL-6R + IL-1b - TNF-a dependant + IL-17 - TNF-a IL-1b + IFN- + PMC - IL-6 IFN- CD40-CD154 + IFN- - IL-1b - TNF-a dependant IFN- Neutrophils Macrophages Natural killer cells + “Switching” between infiltrate phenotypes + IL-6-sIL-6R + CC chemokines MCP-1 - RANTES – C10 Lymphocytes Acquired immunity Current paradigm of contemporary sepsis research Uncontrolled inflammatory response vs Inadequate immune response IL-10-deficient mice demonstrate multiple organ failure and increased mortality during Escherichia coli peritonitis despite an accelerated bacterial clearance [Sewnath ME et al., J Immunol 2001] IL-10-deficient mice demonstrate multiple organ failure and increased mortality during Escherichia coli peritonitis despite an accelerated bacterial clearance [Sewnath ME et al., J Immunol 2001] IL-10-/- mice have an enhanced bacterial clearance IL-10-deficient mice demonstrate multiple organ failure and increased mortality during Escherichia coli peritonitis despite an accelerated bacterial clearance [Sewnath ME et al., J Immunol 2001] IL-10 mice have elevated TNF and chemokine concentrations in peritoneal fluid and plasma IL-10-deficient mice demonstrate multiple organ failure and increased mortality during Escherichia coli peritonitis despite an accelerated bacterial clearance [Sewnath ME et al., J Immunol 2001] IL-10-/- mice have more severe multiple organ damage IL-10-deficient mice demonstrate multiple organ failure and increased mortality during Escherichia coli peritonitis despite an accelerated bacterial clearance [Sewnath ME et al., J Immunol 2001] IL-10-deficient mice demonstrate multiple organ failure and increased mortality during Escherichia coli peritonitis despite an accelerated bacterial clearance [Sewnath ME et al., J Immunol 2001] Control Anti-IL-4 Anti-IL-13 J Immunol 2000 Signal transducer and activator of transcription (STAT) STAT 4 and STAT6 are transcription factors that are essential in mediating responses to IL-12 and IL-13 respectively WT J Exp Med 2001 J Exp Med 2001 Peritoneal levels IFN-y level was not augmented in STAT6-/Mice J Exp Med 2001 STAT6-/- mice showed an altered cytokine profile in the peritoneum in favor of bacterial clearance. J Exp Med 2001 These data suggest that more effective bacterial clearance in the peritoneum may result in a reduction in organ inflammation and damage J Exp Med 2001 J Exp Med 2001 J Exp Med 2001 Systemic organ damage initiated by CLP was ameliorated in STAT4-/mice without affecting bacterial load in the peritoneum and peripheral blood J Exp Med 2001 Aberrant inflammation and lethality to septic peritonitis In mice lacking STAT3 in macrophages and neutrophils [Matsukawa A et al., J immunol 2003] - Increased lethality to CLP in mice lacking STAT3 - Exacerbated systemic inflammation and organ damage - Failure to facilitate effective bacterial clearance despite increased numbers of infiltrating leukocytes and enhanced cytokine production -Impaired innate immune response in leukocytes * These data suggest that impaired bacterial clearance is not likely the cause of increase lethality * The present data highlight evidence that the innate immune cells appear to be essential not only for the initiation and development of inflammatory response but also the resolution of the response, playing multifunctional roles in innate immunity during sepsis. Conclusions 1. Cellular interactions: PMCs / macrophagesmonocytes / Mast cells / Lymphocytes / 2. Neutrophil recruitment 3. Uncontrolled inflammatory response