Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Heart failure wikipedia , lookup
Antihypertensive drug wikipedia , lookup
Lutembacher's syndrome wikipedia , lookup
Management of acute coronary syndrome wikipedia , lookup
Hypertrophic cardiomyopathy wikipedia , lookup
Mitral insufficiency wikipedia , lookup
Cardiac surgery wikipedia , lookup
Coronary artery disease wikipedia , lookup
Cardiac contractility modulation wikipedia , lookup
Myocardial infarction wikipedia , lookup
Quantium Medical Cardiac Output wikipedia , lookup
Jatene procedure wikipedia , lookup
Dextro-Transposition of the great arteries wikipedia , lookup
Arrhythmogenic right ventricular dysplasia wikipedia , lookup
Atrial fibrillation wikipedia , lookup
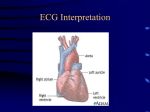
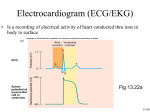
RT 30 Final Exam Review What is the blood flow through the heart? 1) Blood enters the heart thru the inferior and superior vena cava 2) It then flows into the right atrium. 3) Thru the tricuspid valve into the Right Ventricle. 4) It then passes thru the pulmonic semilunar valve. 5) Then thru the pulmonary bed of the R. and L. lungs and back into the left atrium. 6) It then flows thru the bicuspid valve. 7) And into the left ventricle 8) Thru the aortic semilunar valve and into the aorta and systemic vascular system. What is the normal conduction through the heart? SA AV BH PF What is endocarditis? What can cause it? An inflammation of the inner layer of the heart, It usually involves the heart valves Other structures that may be involved include the interventricular septum, the chordae tendineae. Endocarditis is characterized by a prototypic lesion, the vegetation, which is a mass of platelets, fibrin, microcolonies of microorganisms, and scant inflammatory cells Injection of bacteria through dirty needles What is Pericarditis? •Fluid accumulation surrounding the heart, may lead to a life threatening condition called cardiac tamponade •Cardiac tamponade is compression of the heart that occurs when blood or fluid builds up in the space between the myocardium and the pericardium What is Myocarditis? Myocarditis is most often due to infection by common viruses, less commonly nonviral pathogens such as Borrelia burgdorferi (Lyme disease) or Trypanosoma cruzi, or as a hypersensitivity response to drugs. The definition of myocarditis varies, but the central feature is an infection of the heart, with an inflammatory infiltrate, and damage to the heart muscle, without the blockage of coronary arteries that define a heart attack (myocardial infarction) What is Valvular disease? Valvular heart disease is characterized by damage to or a defect in one of the four heart valves: the mitral, aortic, tricuspid or pulmonary. The mitral and aortic valves are the ones most frequently affected by valvular heart disease. Valvular heart disease is characterized by damage to or a defect in one of the four heart valves: the mitral, aortic, tricuspid or pulmonary. The mitral and aortic valves are the ones most frequently affected by valvular heart disease. Describe the following CHFCADMICor PulmonaleHTN- Pulm HTNWhat are characteristics and treatments of each? What are the names of the coronary arteries? Left Coronary artery Anterior Descending Artery ◦ Supplies anterior sulcus and apex ◦ Widow maker heart attack Circumflex Artery ◦ Supplies posterior side of left ventricle What are the names of the coronary arteries? Together supply most of left ventricle, left atrium, 2/3 of intra ventricular septum, half of intra atrial septum, and part of right atrium Right Coronary Artery Posterior Descending Artery ◦ Supplies posterior intraventricular sulcus Has numerous smaller branches Supplies anterior and posterior portions of right ventricular myocardium, right atrium, sinus node, posterior 1/3 of intraventricular septum, and portion of base of right ventricle Coronary Veins Closely parallel the arterial system oSome coronary venous blood enters the heart through the Thebesian veins ◦ Thebesian veins empty directly into all chambers thus creating some venous admixture lowering Pa02 What is a MI? What causes it, how is it treated? MONA •Immediate assessment (<10 minutes) •Measure vital signs (automatic/standard BP cuff) •Measure oxygen saturation •Obtain IV access •Obtain 12-lead ECG (physician reviews) •Perform brief, targeted history and physical exam; focus on eligibility for fibrinolytic therapy •Obtain initial serum cardiac marker levels •Evaluate initial electrolyte and coagulation studies •Request, review portable chest x-ray (<30 minutes) •Immediate general treatment •Oxygen at 4 L/min •Aspirin 160 to 325 mg •Nitroglycerin SL or spray •Morphine IV (if pain not relieved with SVR and PVR formula The Vascular System-Systemic Vascular Resistance (SVR) Sum of all frictional forces opposing blood flow through the vascular circulation SVR = Mean Aortic Pressure-Right Atrial Pressure x80 Cardiac Output ◦ Mean Aortic Pressure - Use Systolic Pressure (normal mean = 90mmhg) ◦ Right Atrial Pressure - Use Central Venous Pressure (normal mean = 4mmhg) ◦ Cardiac Output normal mean = 5L/min PVR Formula: MPAP – PCWP / CO x 80 The Vascular System-Blood Pressure Systolic Pressure Diastolic Pressure ◦ Pressure during contraction phase of heart ◦ Pressure during relaxation phase of heart ◦ Normal value: 90 – 140 mmHg ◦ Normal value: 60 – 90 mmHg http://www.nlm.nih.gov/medlineplus/ency/anatomyvideos/000013.htm Mean Arterial Pressure MAP = (2 x diastolic pressure) + (systolic pressure) 3 A MAP of about 60 is necessary to perfuse coronary arteries, brain, kidneys. Cardiac Output Cardiac Index ◦ Volume of blood pumped by the heart per minute divided by body surface area CI = CO BSA ◦ Normal range of cardiac index is 2.5 - 4.0 L/min per square meter. Low values can indicate cardiogenic shock Stroke Volume End-Diastolic Volume (EDV) Volume to which the ventricles fill during diastole Formula: SV = EDV – ESV Normal value: 60 – 130 ml/beat Stroke Volume Ejection Fraction (EF) ◦ Proportion of EDV ejected on each stroke EF = SV EDV ◦ Normal Value – 70% Factors Affecting Stroke Volume Preload ◦ Initial stretch of the ventricle ◦ The greater the preload, the greater the tension on contraction Factors Affecting Stroke Volume Afterload ◦ Force against which the heart must pump ◦ In clinical practice, left ventricular afterload equals systemic vascular resistance. Factors Affecting Stroke Volume Contractility ◦ Amount of systolic force exerted by heart muscle at any given preload. ◦ Increases in contractility leads to higher EF, lower end systolic volume, and higher stroke volume Inotropic (drugs that increase cardiac contraction) Chronotropic (drugs that increase cardiac rate) Factors Affecting Stroke Volume Contractility ◦ Decreases in contractility lead to lower ejection fraction, higher end systolic volume, and decreased stroke volume. Inotropism: Is any factor which affects the contractility of the heart ◦ Positive Inotropism ◦ Higher stroke volumes for a given preload: indicating an increase in contractility. Factors Affecting Stroke Volume Contractility Negative inotropism Decreased stroke volumes for a given preload: indicates a decrease in contractility Factors Affecting Stroke Volume Heart Rate (60-100) Autonomic Nervous System oSympathetic: fight or flight: HR, RR, BP, pupilary dilation and bronchodilation. oParasympathetic: rest and digest Factors Affecting Stroke Volume Heart Rate ◦ Cardiac output directly proportional to heart rate ◦ Relationship exists up to 160 to 180 beats/min ◦ Filling time for ventricles insufficient at higher rates Arrhythmia Review Initial Approach—Analysis 4 Questions Rate? ◦ Normal ◦ Bradycardia, Tachycardia Rhythm? ◦ Regular or Irregular Are there P waves? ◦ Is each P wave related to a QRS with 1:1 impulse conduction? QRS normal or wide? Premature Atrial Contraction (PAC) • Rate • Rhythm • P waves • P → QRS • Therapy QRS Normal Sinus rate Irregular—interrupted by PAC Incomplete compensatory pause Different morphology Usually conducted with normal QRS Treat underlying cause 34 Atrial Fibrillation • Rate • Rhythm • P waves • F → QRS • Therapy Atrial rate cannot be measured Ventricular rate—variable Irregular (irregularly irregular) Absent (fibrillation waves) Conduction irregular Slow ventricular rate Treat underlying cause 35 Atrial Flutter QRS Normal • Rate • Rhythm • P waves • F → QRS • Therapy Atrial rate 250-400/min (often 300) Ventricular rate—variable Regular (2:1 AV block common) Absent (flutter waves) Conduction regular (unless variable block) Slow ventricular rate: terminate arrhythmia Treat underlying cause 36 Self-Assessment What are the rate and rhythm? A B 37 Clinical Correlation This patient is unresponsive and BP is 70/50 mm Hg. What is the rhythm? What is your next action? 38 PVC Morphology—Match the Name • Unifocal PVCs • Multifocal PVCs • • Bigeminy • Torsades Ventricular Tachycardia 39 Ventricular Fibrillation (VF) Ventricular Fibrillation (VF) Polymorphic VT TX without pulse: ◦ CPR ◦ DEFIB ◦ EPI/Mg 2g Ventricular Tachycardia Monomorphic* *Sustained—requires intervention for >30 seconds • Rate • Rhythm • P waves • P → QRS • Therapy Atrial rate normal Onset tachycardia abrupt Regular Present—obscured Blocked—fusion complexes possible Antiarrhythmic agent, cardioversion, high-energy (defibrillation dose) shock Polymorphic VT* *Torsades de pointes—QT prolonged • Rate • Rhythm • P waves • P → QRS • Therapy Atrial rate normal (obscured) Onset tachycardia abrupt Irregular Present—obscured Blocked—fusion complexes possible Unsynchronized high-energy shock, magnesium (beneficial with baseline QTC prolongation) Ventricular Fibrillation Coarse VF • Rate • Rhythm • P waves • P → QRS • Therapy Chaotic, uncountable Onset abrupt Irregular Absent; no normal QRS complexes Not applicable Immediate shock(s) Ventricular Fibrillation Fine VF • Rate • Rhythm • P waves • P → QRS • Therapy Chaotic, uncountable Onset abrupt Irregular Absent; no normal QRS complexes Not applicable Immediate shock(s) Asystole Agonal Complexes Pulseless Electrical Activity • • • • • Rate Rhythm P waves P → QRS Therapy ASYSTOLE Absent None—“flatline” Absent Not applicable CPR, vasopressor Pulseless Electrical Activity (PEA) ARTERIAL PRESSURE • Rate • Rhythm • Therapy Variable—depends on baseline rhythm PEA is not a single rhythm but any organized rhythm without a pulse Identify and treat underlying cause CPR, vasopressor Self-Assessment What are the rate and rhythm? A C B A B What rhythms do we defibrillate? Cardiovert? 1. 2. Epinephrine • Epinephrine is a naturally occurring catecholamine with both - and - adrenergic agonist activity • Administer 1 mg (10 mL 1:10 000 IV bolus) every 3 to 5 minutes during cardiac arrest • Stimulation of -adrenergic receptors increases peripheral vasoconstriction and as a result increases coronary and cerebral blood flow Epinephrine Stimulation of -adrenergic receptors • Increases heart rate, contractility, and conduction velocity • Increases conduction through the atrioventricular node • Decreases the ventricular muscle refractory period: these latter effects may increase the likelihood of arrhythmias Epinephrine in Cardiac Arrest Epinephrine may be administered IV/IO Endotracheal administration provides uncertain doses Remember to flush with 20 mL of fluid and elevate the arm or leg Special Considerations Cautions—Contraindications Important to REMEMBER: High doses can cause arrhythmias High doses do not improve survival and may contribute to postresuscitation myocardial dysfunction • A naturally occurring hormone, also known as antidiuretic hormone (ADH) • Causes vasoconstriction by directly stimulating smooth muscle receptors • Causes no increase in myocardial oxygen consumption during CPR— no -receptor activity Vasopressin Clinical studies have shown vasopressin equivalent to epinephrine for treatment of cardiac arrest Vasopressin Vasopressin can be substituted for the first or second dose of epinephrine Give 40 units IV/IO bolus Coronary perfusion pressure Vital organ blood flow Median frequency VF Cerebral oxygen delivery Bradycardia First-Degree AV Block Sinus Node P • Underlying sinus rhythm • One P wave • PR interval >0.20 second • One P wave for each QRS AV Node AV Nodal Tissue >0.20 seconds QRS <0.12 His-Purkinje System 57 Second-Degree AV Block—Mobitz I Wenckebach Phenomenon Sinus Node • Underlying sinus rhythm • P wave fails to periodically conduct • PR interval prolonged • One P wave for each QRS until block P AV Nodal Tissue >0.20 seconds PR interval X QRS His-Purkinje System 58 Second-Degree AV Block—Mobitz II PR intervals unchanged Sinus Node P Block • Underlying sinus rhythm • One P wave • PR interval usually normal, no prolongation • One P wave for each QRS until sudden block and dropped QRS AV Node Often AV Normal Nodal Tissue Often normal QRS complex His-Purkinje System 59 Third-Degree AV Block—Junctional Escape P waves unrelated to QRS Sinus Node • Underlying sinus rhythm (usual) • Escape junctional rate 40-60 • PR interval variable • P waves unrelated to QRS P QRS from AV-His escape AV Node QRS <0.12 • Narrow QRS = block above His junction His Purkinje System 60 AV Block—Which Type? Properties of Heart Muscle Excitability ◦ Ability to respond to electrical, chemical, or mechanical stimulation Properties of Heart Muscle Excitability This is important as the heart will respond to defibrillation, cardioversion, and medication Properties of Heart Muscle Automaticity ◦ Ability of cardiac muscle to initiate a spontaneous electrical impulse (only cell capable of doing this) ◦ Highly developed in specialized areas – pacemaker or nodal tissue Automaticity Automaticity of the heart is produced by spontaneous and repetitive depolarization of certain cardiac cells, known as pacemaker cells. The depolarization of these cells leads to the generation of action potentials, which are electrical signals that are propagated throughout the cardiac muscle tissue and result in contractions. Understanding depolarization is essential to comprehending cardiac electrophysiology as a whole. Automaticity Depolarization: The process of depolarization occurs at the cellular level and involves changes in the electrical environment of a cell. This electrical environment is determined by the difference in the concentrations of charged particles between the inside and outside of the cell. Automaticity Resting Membrane Potential: At rest, the inside of a myocardial cell has a charge that is more negative than its surroundings. Therefore, the cell is said to have a negative resting membrane potential. This potential is normally around -90 millivolts, meaning the charge inside the cell is 90 millivolts lower than the surrounding environment. Properties of Heart Muscle Conductivity ◦ Ability to radiate electrical impulses ◦ Impaired in response to necrotic tissue from ischemic injury (MI) Contractility ◦ Ability to contract in response to an electrical impulse ◦ Impaired by hypertrophy, cardiomyapathy, CHF Activation of Central Chemoreceptors by changes in arterial Pco2 Medulla Chemoreceptors IN H2O CO2 H2CO3 H+ HCO3- CO2 CSF BBB plasma capillary Performing an EKG Basic Electrocardiography-Terms Polarization ◦ Difference in electrical potential between two points in tissue; the resting state of cardiac muscle Basic Electrocardiography Peripheral and central chemoreceptors respond to changes in blood chemistry, mainly CO2, pH and O2. Low O2 = increase HR and RR High CO2 (H+ in medulla) = Increased HR and RR Low pH (aciditc) = Increase HR and RR Baroreceptors: Increase pressure = Increased HR, decreased pressure = increased HR And contractility Basic Electrocardiography-Terms Depolarization ◦ Influx of sodium into the interior portion of the cells causing muscle contraction Repolarization ◦ Rapid return of the cell to the polarized state EKG Paper The Electrocardiogram P Wave ◦ Produced by atrial depolarization ◦ Normally 0.06 to 0.11 seconds in duration The Electrocardiogram QRS Complex ◦ Produced by ventricular depolarization ◦ Normally 0.03 to 0.12 seconds in duration ◦ Repolarization of the atria occurs simultaneously with QRS and is hidden by the QRS complex The Electrocardiogram T Wave ◦ Produced by ventricular repolarization ◦ Normally 0.14 to 0.26 seconds The Electrocardiogram PR Interval ◦ Time from beginning of atrial depolarization to beginning of ventricular depolarization ◦ Normal interval is 0.12 to 0.20 seconds The Electrocardiogram RR Interval ◦ Time from peak of one QRS complex to the next QRS complex ◦ Normally 0.6 to 1.0 seconds ◦ Used to measure total cardiac cycle The Electrocardiogram PP Interval ◦ Time from beginning of one P wave to the beginning of the next P wave ◦ Normally equal to RR interval ◦ Also used to measure total cardiac cycle The Electrocardiogram Event Time P Wave 0.06 – 0.11 Seconds PR Interval 0.12 – 0.20 Seconds QRS Complex 0.03 – 0.12 Seconds T Wave 0.14 – 0.26 Seconds PP/RR Intervals 0.6 – 1.0 Seconds ECG Leads Lead I: ◦ (-) Negative Electrode on Right Arm ◦ (+) Positive Electrode on Left Arm Sinus Bradycardia Rate less than 60 Rhythm is regular P wave prior to each QRS/QRS for each P wave PR interval normal QRS interval normal Sinus Tachycardia Rate greater than 100 Rhythm is regular P wave prior to each QRS/QRS for each P wave PR interval normal QRS interval normal Sinus Tachycardia Causes • • • • • • • • • • • Fever Anxiety Pain Dehydration Anemia Hypoxemia (generally first sign) If symptomatic: Anxiety Feelings of fear or panic Feelings of a pounding chest Treat underlying cause http://www.youtube.com/watch?v=cKXrzLrQOCc Atrial Fibrillation Rate 100-160 BPM Rhythm is irregular P waves absent and replaced by irregular electrical activity QRS interval normal to narrow Most common arrhythmia Atrial Fibrillation Causes: ◦ ◦ ◦ ◦ Disorganized electrical impulses that originate in the atria and pulmonary veins Hypertension Hyperthyroidism Primary heart disease If symptomatic: Palpitations SOB Exercise intolerance Clot formation within heart/lungs/brain/legs Ect. Dizziness/ somnolence/ decreased LOC http://www.youtube.com/watch?v=70QE1poMZ1E&feature=related Atrial Fibrillation Treatment • Anti-Coagulants • Beta Blockers If symptomatic: • Immediate Cardioversion • Oxygen http://www.youtube.com/watch?v=1rcg6Ce7p18 ECG Leads Lead II ◦ Negative Electrode on Right Arm, Positive Electrode on Left Leg ◦ Used Most Commonly in Acutely Ill Patients With Leads Placed on Chest Rather Than on Limbs ECG Leads Lead III ◦ Negative Electrode on Left Arm, Positive Electrode on Left Leg Leads I, II, and III Comprise Einthoven’s Triangle And Present Electrical Activity of The Heart From Three Different Orientations Electrocardiogram Einthoven’s triangle • Three standard limb leads • Voltage differences between corners of triangle • We will use “Lead II” ◦ Right shoulder to left leg 03 Sept. 2013 92 EKG-Lab.ppt Limb Leads ECG Leads Precordial Leads ◦ Leads V1, V2, V3, V4, V5, And V6 ◦ V1 – Positive Electrode Placed at Right Sternal Margin And Fourth Intercostals space ECG Leads Precordial Leads ◦ Successive Leads Placed Laterally to The Left With V6 at Mid Axillary Line ◦ Electrical Activity Measured From Six Different Locations And Depicted Differently For Each Lead Precordial Leads Sinus Bradycardia Rate less than 60 Rhythm is regular P wave prior to each QRS/QRS for each P wave PR interval normal QRS interval normal Sinus Tachycardia Rate greater than 100 Rhythm is regular P wave prior to each QRS/QRS for each P wave PR interval normal QRS interval normal Sinus Tachycardia Causes If symptomatic: • • • • • • • • • • Fever Anxiety Pain Dehydration Anemia Hypoxemia (generally first sign) Anxiety Feelings of fear or panic Feelings of a pounding chest Treat underlying cause http://www.youtube.com/watch?v=cKXrzLrQOCc Atrial Fibrillation Rate 100-160 BPM Rhythm is irregular P waves absent and replaced by irregular electrical activity QRS interval normal to narrow Most common arrhythmia Atrial Fibrillation Causes: ◦ ◦ ◦ ◦ Disorganized electrical impulses that originate in the atria and pulmonary veins Hypertension Hyperthyroidism Primary heart disease If symptomatic: Palpitations SOB Exercise intolerance Clot formation within heart/lungs/brain/legs Ect. Dizziness/ somnolence/ decreased LOC http://www.youtube.com/watch?v=70QE1poMZ1E&feature=related Atrial Fibrillation Treatment • Anti-Coagulants • Beta Blockers If symptomatic: • Immediate Cardioversion • Oxygen http://www.youtube.com/watch?v=1rcg6Ce7p18 Supraventricular Tachycardia Rate 140-220 Rhythm is regular P waves absent (buried in the T wave) QRS interval usually normal PR interval - impulses stimulating the heart are not being generated by the sinus node, but instead are coming from a collection of tissue around and involving the atrioventricular (AV) node Supraventricular Tachycardia •Causes: CAD Thyroid disease COPD Caffeine Stress • If symptomatic: Palpitations Dizziness Anxiety Chest pain Loss of consciousness http://www.youtube.com/watch?v=ReJo4aclOw8 Supraventricular Tachycardia Treatment Vagal manuvers Carotid massage Cardioversion: Electrical/Chemical (Adenosine) Medications Oxygen Ablation Pacemaker http://www.youtube.com/watch?v=xLzRFAT9uFA Basic ECG Interpretation NSRo Is the rate regular? o Is the rate between 60-100? o Is their a P wave prior to each QRS/ QRS for each P wave? o Is the PR interval normal - .12 to .2 Sec? (less than 1 big box) o Is the QRS interval less than .12 Sec? (less than 3 little boxes) PHARMACOLOGY (indications/dose and classification) Adenosine Atropine Amiodarone Lidocaine Epinephrine Dopamine Levophed Vasopressin Depolarizing Agents Bind to acetylcholine receptor sites causing a postsynaptic membrane depolarization Prevention of repolarization causes the postsynaptic ending to become refractory and unexcitable, resulting in muscle flaccidity Non-Depolarizing Agents Produce paralysis and muscle weakness by competing with acetylcholine for binding at the receptor site Prevention of the binding of acetylcholine prevents depolarization of the site, thereby preventing muscle contraction Action Action Prevents acetylcholine from binding at the receptor site Shorter acting than non-depolarizing agents Will cause total muscle paralysis in 60 to 90 seconds that lasts from 10 to 15 minutes Do not have reversing agents Generic name Proprietary name Succinylcholine Anectine Indications - Short acting paralytic ideal for intubation or similar procedures Competitive inhibition of acetylcholine at muscle post-synaptic receptor site Effects felt in 2 to 10 minutes and last for 30 to 60 minutes May be reversed by cholinesterase inhibitors, e.g., Neostigmine Generic Name Proprietary Name Tubocurarine d-tubocurarine Pancuronium Pavulon Metocurine Metubine Vecuronium Norcuron Rocuronium Zemuron, Esmeron Indications - Need for longer term paralysis - Patient-ventilator synchrony - Muscle relaxation during surgery - Indications - Reduction of intracranial pressure - Immobility in trauma patients- Minimize oxygen consumption Indications for NMBAs Endotracheal intubation Muscle relaxation during surgery Enhancement of patient-ventilator synchrony Reduction of intracranial pressure in intubated patients Minimizes oxygen consumption Facilitation of procedures or diagnostic studies Maintenance of immobility, e.g., trauma patients (Flail Chest) Narcotis and Analgesics Know opiods (high, mod, low potency) Morphine Oxymorphone Fentanyl Methadone Hydromorphone (Dilaudid) Demerol Percocet Oxycontin Codeine Narcotic Antagonist Narcan Sedative and Hypnotics Ativan Versed Xananax Valium Deprivan Haldol Pentothal Pentobarbital Phenobarbital Reversal of Benzos Ramazicon Other Meds Diruretics: Diamox, Lassix, Mannitol, Carbonic anyhydrase inhibitors Steroids: Side effects, indications… HEMODYNAMICS Values PAP, CVP, PCWP Causes of each to increase/decrease Indications for PICC, A-lines, Central and PA lines Troubleshooting PA and A-line tracings Cardiac output assessments Formulas CVO2= DO2= C(a-v)= SVO2= EF= PFT’S Spirogram Lung Volumes & Capacities Lung Volumes & Capacities Examples of Flow-Volume Loops in Disease States Examples of Flow-Volume Loops in Disease States SVC Purpose: To determine the maximum amount of the volume that can be taken in and exhaled with a single breath FVC To measure flow rates and lung volumes in order to determine the presence of obstructed or restricted lung impairment Spirometry Forced vital capacity (FVC) ◦ Technique – subject breaths normally for several breaths, then inspires maximally and exhales as forcefully and fully as possible ◦ Should be within 200 mL of VC Spirometry Forced expiratory volume (most commonly FEV1) ◦ Volume which can be exhaled in one second using maximum patient effort ◦ Determined from the FVC ◦ Decrease in value indicates obstructive changes in small airways Spirometry Spirometry FEF25%-75% ◦ Average expiratory flow rate of the middle 50% of the FVC ◦ Measured in liters per second ◦ Indicates flow from medium and small airways ◦ Changes from smoking occur in medium airways prior to changes in small airways MVV To measure muscle strength during times of increased exertion Measurements of RV/TLC Nitrogen Washout Helium Dilution Body Box Spirometry Maximum voluntary ventilation (MVV) ◦ Calculates the maximum volume of gas that a patient can ventilate in one minute ◦ Technique – subject is directed to breathe rapidly and deeply for 12 to 15 seconds; the total volume inspired or expired is measured; the volume is extrapolated to one minute DLCO To evaluate the ability of the lungs to take in oxygen from the air, and transfer the oxygen across the lungs into the blood stream Interpreting the PFT Report The FEV1/FVC ratio is a good place to start; reduced (<70%) with obstructive lung disease If TLC less than 80% of predicted normal and FEV1/FVC is normal, restrictive disease is present. If DLCO is <80% of normal, a diffusion defect is present. ◦ Reduced surface area = emphysema ◦ Thickened AC membrane = pulmonary fibrosis 132